The spinal cord extends from the brain down the spinal canal in the spinal column. The spinal cord is surrounded by the dural sacs, which are a continuation of the membranes covering the brain. The membranes covering the brain are the dura mater; the arachnoid membrane, which contains cerebrospinal fluid; and the pia mater. The nerves that arise from the spinal cord (also called nerve roots) are extensions of the spinal cord and are responsible for transmitting signals to and from muscles and other structures throughout the body. These impulses allow the brain to interpret information from the body including pain, touch, and body position in space. Communication signals allow the brain to control the functioning of organs and muscle movements.
The spinal cord ends at the level of the first lumbar vertebra in the lower back, forming the conus medullaris. Fibrous traction of the spinal cord - filum terminale. The bundle of nerve roots below the conus medullaris is called the cauda equina.
Compression or inflammation of the nerve roots can cause symptoms such as pain, changes in reflexes, decreased muscle strength, and decreased sensation. Although these symptoms can be severe and in some cases lead to permanent disability, most often the symptoms respond quite well to conservative treatment.
An extreme variant of root compression or inflammation is cauda equina syndrome. Cauda equina syndrome is a very serious condition caused by compression of the roots in the lower spinal canal. Equine canal syndrome is a surgical emergency and, if untimely surgical intervention, can lead to persistent dysfunction of the bladder and paresis of the lower extremities.
Symptoms
Symptoms of cauda equina syndrome include:
- Pain in the lumbar region
- Radicular pain in one or both legs (pain begins in the buttock and radiates down the back of the thigh and lower leg).
- Numbness in the groin or in the area of the sacrum, coccyx
- Bladder and bowel dysfunction.
- Muscle weakness in the lower extremities and decreased sensitivity
- Decreased or absent reflexes in the lower extremities.
- Pain in the lumbar region can be divided into local and radicular pain.
- Local pain is a deep, chronic pain that occurs due to irritation of the soft tissues and vertebral body.
- Radicular pain is an acute pain that occurs as a result of compression of the nerve roots. Radicular pain is projected in the dermatomes (along certain areas that are innervated by a given root).
Bladder dysfunction in cauda equina syndrome is manifested by:
- Urinary retention
- Difficulty starting to urinate
- Decreased sensitivity of the urethral sphincter.
- Bowel problems may include the following symptoms:
- Incontinence
- Constipation
- Decreased tone and sensitivity of the anus.
Cauda equina syndrome is a serious surgical condition. Patients should seek medical attention if they have symptoms. Often, lower back pain and muscle weakness are associated with a disc herniation and do not require emergency surgical intervention.
Clinical studies have shown that the likelihood of regaining function and having a positive outcome is directly related to the duration of symptoms of cauda equina syndrome. Within 48 hours of the onset of symptoms of the cauda equina, surgical decompression is necessary - surgical removal of tissue causing compression of the roots (such as a herniated disc, osteophyte).
Causes of root damage
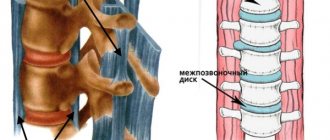
In normal condition, the spinal roots are located along the spinal canal quite freely, despite its small thickness. This ensures full passage of nerve impulses and stable operation of all roots. When the fibers are compressed, displaced, or broken, the conductive function is disrupted, partially or completely, and the areas for which the damaged roots are responsible lose sensitivity and mobility.
Common causes of such damage are:
- herniated intervertebral discs in the lumbar region;
- back injuries as a result of blows, falls, gunshot wounds;
- spinal cord tumor and metastases from prostate, lung, and breast cancer;
- inflammation, infectious lesions of the spinal cord;
- congenital pathologies;
- complications after surgery and medical procedures;
- hematomas formed as a result of spinal hemorrhages;
- narrowing of the spinal canal.
Diagnostics
A preliminary diagnosis of cauda equina syndrome is made based on the results of a patient examination, medical history, the presence of motor disorders in the lower extremities, impaired sensitivity in the perineal area, decreased reflexes in the lower extremities
Imaging tests include plain x-rays to help identify degenerative changes or injury. MRI (including with contrast) makes it possible to diagnose a tumor, infection, the presence of disc herniations and visualize nerve roots (their degree of compression). Based on the studies, the surgeon can plan the necessary treatment.
But not all people with low back pain and/or leg pain and changes in bowel or bladder function have cauda equina syndrome. Often, bladder problems are associated with a bladder infection (can be diagnosed with a urine test) or diabetes (can be diagnosed with a blood sugar test).
In addition, it is necessary to exclude the possibility of infection or oncological origin of symptoms. Therefore, it is necessary to conduct extensive laboratory tests such as general blood tests, blood biochemistry, serological tests (to rule out syphilis or Lyme disease).
Here is what allows you to reliably diagnose cauda equina syndrome:
- Disease history
- Physical examination: assesses muscle strength, reflexes, sensation, stability and motor abilities.
- Lab tests
- Magnetic resonance imaging (MRI) provides three-dimensional images of the spine.
- Myelogram - an x-ray method of imaging the spine with the introduction of contrast, allowing to determine the pressure on the spinal cord or nerves
- Computed tomography (CT).
Treatment
Treatment options depend on the underlying causes of cauda equina syndrome. Anti-inflammatory drugs such as ibuprofen (Advil, Motrin) and corticosteroids such as methylprednisolone (Solu-Medrol, Depo-Medrol) may be effective in patients with inflammatory conditions, including ankylosing spondylitis (ankylosing spondylitis). In rare cases, such as spinal metastases, it may be necessary to consider radiotherapy, especially if surgery is contraindicated.
In patients with cauda equina syndrome caused by infection, adequate antibiotic therapy must be prescribed. Patients with spinal cord tumors require radiation therapy or chemotherapy.
Treatment tactics for cauda equina syndrome should be extremely careful. If there are signs of primary cauda equina syndrome (numbness in the perineum, dysfunction of the bladder and intestines, weakness in the legs), then the patient can only undergo conservative treatment for 24 hours. Lack of effect is an indication for emergency surgery (surgical decompression minimizes the effects of compression on nerves and neurological deficits in the future)
In patients with a herniated disc (the cause of cauda equina syndrome), a laminectomy or discectomy is performed.
Many studies have been conducted to identify the dependence of various factors in determining the prognosis after surgical treatment for cauda equina syndrome.
- Patients with bilateral sciatica had a less favorable prognosis than people with unilateral sciatica.
- Patients with complete perineal anesthesia are more likely to have persistent bladder palsy.
- The degree of sensitivity impairment in the perineal area is considered the most reliable prognostic criterion.
Causal factors
The main reason for the development of almost any disease of the spine is its congestion, which occurs when lifting heavy objects, prolonged sitting or incorrect posture.
There are a number of reasons that cause compression and damage to the terminal nerve bundle, as well as diseases that lead to the development of the syndrome.
Ossification of the cartilage of the intervertebral disc and loss of its shock-absorbing properties are observed in osteochondrosis. The nerve endings are compressed by a rigid connection and become pinched, which results in pain. If left untreated, degenerative and dystrophic processes in the intervertebral discs lead to their prolapse and the development of a serious complication of the disease - intervertebral hernia, which further compresses the nerve fibers. This pathology is the most common cause of the syndrome.
- Subluxations of the vertebrae, fractures of the sacrum and coccyx are usually accompanied by damage to the nerve trunks. Hematomas formed after injury cause compression. This group of causes also includes iatrogenic injury, which is a complication of epidural anesthesia, neurosurgical operation or spinal diagnostic puncture.
- Benign tumors compress nerve roots, and malignant tumors grow into nerve bundles, causing their destruction. Metastases from malignant tumors of other organs can also provoke the syndrome.
- Congenital narrowing of the lower segments of the spinal column is the cause of compression of the nerve bundles.
- Spondylosis and spondyloarthrosis are acquired deformities of the spine caused by age-related changes in the human body.
- Infectious and inflammatory processes - neuroinfections, osteomyelitis and epidural abscess. The source of infection is chronic foci in the human body: caries, otitis media, tonsillitis, sinusitis, pharyngitis, furunculosis.
- Spondylolisthesis is the slippage of one vertebra from another.
- Demyelination of nerve fibers is a consequence of multiple sclerosis.
- Pathology of the vessels that supply the spinal cord and bleed under some circumstances can cause compression of the nerves.
Damage to the spinal nerves first causes their irritation and hyperexcitability, which is accompanied by pain. Gradually, the function of the nerve trunks weakens. Under the continuous influence of the causative factor, it completely fades away, which leads to motor and sensory disorders in the innervation zone.
Risk factors contributing to the development of pathology:
- Floor. Men are at higher risk of developing the syndrome than women. This is due to faster wear of cartilage and bone tissue.
- Injuries. The occurrence of pathology is facilitated by operations on the spine, injuries, sharp turns and falls on the back.
- Obesity. Fat deposits increase the load on the back, which negatively affects the condition of the intervertebral discs. In obese individuals, muscle tone decreases, and the spine gradually loses its flexibility.
- Smoking. Toxins disrupt the blood supply to the intervertebral discs and increase the risk of developing the disease many times over.
- Passive lifestyle. Office workers, drivers and salespeople are much more likely to develop the syndrome than people in other professions.
- Hereditary predisposition is the presence of diseases of the spine and peripheral nervous system in close relatives.
- Heavy lifting and vibration have a negative impact on the spine.
To study Dorsopathy: what is it?
Prevention
Prevention of equine syndrome is aimed at identifying the symptoms of this syndrome. In most cases, patients with lower back pain, leg pain, or leg weakness do not develop cauda equina syndrome. Bowel or bladder symptoms or sensory disturbances in the groin area should be of particular concern.
Irreversible changes in nerve fibers often occur and surgical intervention does not eliminate persistent neurological deficits. Therefore, the patient will have to live with this deficiency. Therefore, in such cases, the support of a number of specialists such as a physiotherapist, social worker, and sexologist will be necessary. In addition, it will be necessary to adhere to certain rules if you have bladder and bowel dysfunction:
- Use a catheter to drain urine from the bladder (3-4 times a day).
- Drink enough fluids and practice good hygiene to prevent urinary tract infections.
- If you have constipation, do a cleansing enema or use suppositories.
- Wearing sanitary pads for possible episodes of incontinence.
In addition, it is necessary to regularly consult with your doctor regarding the presence of pain or episodic natural bowel movements. The outlook for cauda equina syndrome depends on the duration of symptoms before surgical treatment. The longer a patient has had symptoms before appropriate treatment, the less likely they are to make a full recovery.