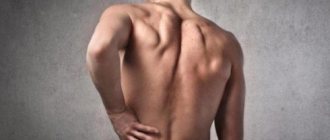
Quite often, girls and women with pain in the lower back or other parts of the back turn to gynecologists or therapists. Soreness can be observed even a month after birth and is accompanied by characteristic symptoms. In some females, the unpleasant sensations are less pronounced and almost unnoticeable, while others have a strong, aching or nagging pain that radiates to the legs.
If such symptoms have been observed for a long time, then it is better for the patient to contact the attending physician or gynecologist-obstetrician, who will carry out a series of diagnostic procedures and find out the cause of the pain. You should not put off visiting a specialist, as these symptoms indicate the presence of a pathological process.
Causes
When very severe, prolonged pain occurs, women begin to worry about why their back hurts after childbirth and what complications there may be. A qualified consultation with a specialist will help you understand the reason. It is not recommended to independently analyze your health status based on symptoms and the process of delivery.
The main causes in the lumbar region and other parts of the spine include the following factors:
- A sharp increase in weight during pregnancy. Weight gain causes a shift in the center of gravity, which can cause some vertebrae to shift or become movable under pressure.
- Consequences of epidural anesthesia. This anesthetic procedure is widespread in all hospitals and private clinics. Conducting epidural anesthesia helps the expectant mother to endure childbirth more easily and reduces pain to a minimum. A special substance is injected into the spinal space, after which the woman’s sensitivity decreases.
- Lifting heavy objects or a baby after childbirth. The weight of a baby or prolonged wearing of large weights affects the lumbar spine, so a woman may experience severe aching pain after walking or before bed.
- Stretching the muscle tissue of the abdomen and back. During the period of bearing a child, the abdominal muscles are greatly stretched, and in the lower back, the muscle tissue, on the contrary, contracts. As a result, the lumbar muscles are in constant tension. This phenomenon explains why the lower back hurts after childbirth.
- Displacement of the hip joints due to difficult childbirth. During delivery, injury to the hip joints or tailbone may occur. This phenomenon occurs rarely due to strong anesthesia or the large weight of the fetus.
- Displacement of internal organs due to enlargement of the uterine cavity. This phenomenon provokes strong pressure on the diaphragm, which can cause pain to radiate to the area of the shoulder blades.
- Inflammatory processes in the abdominal organs. Childbirth can cause inflammation of the uterine cavity and adjacent organs, so after delivery of the fetus, the woman needs to be under the supervision of a doctor for some time.
The cause of unpleasant and painful sensations may be postpartum depression. This symptom is purely psychological in nature, so treatment involves a large number of positive emotions
Types and causes of back pain
Factors that cause pain during pregnancy are of mechanical and hormonal origin.
- Mechanical factors:
- overload - a growing fetus , amniotic fluid, placenta located in front of the spine (+ 5 kg ) , enlarging mammary glands and uterus (+ 2 kg) and net weight gain (3-5 kg) give the pregnant woman an increase in body weight by 10-15 kg. Increased load on the spine causes pain due to a decrease in the height and density the intervertebral discs, compression of the roots and persistent irritation of pain receptors;
- change in posture - an expanding belly forces a woman to lean back to maintain balance. As a result, hyperlordosis is formed (excessive deflection of the lower back ). Violation of the center of gravity and body in space requires effort to maintain balance, which causes increased stress on the facet joints of the spine and stretching of the periarticular capsules. They are well innervated, so their defeat causes pain syndrome , which has a characteristic course. Facet pain is felt in the lower back above the joint, radiating to the groin and limb. Strengthening is observed in the morning, after rest and decreases with physical activity - the pregnant woman needs to “disperse”. After a small load, the pain intensifies and is felt when changing posture , extension/flexion of the spine , its rotation and is relieved again when sitting, leaning on objects, or lying down. With hyperlordosis, not only the joints are affected. The ligaments and muscles of the spine are . Hypertonicity leads to rapid fatigue, injury , inflammation and pain in the back, between the shoulder blades ;
- muscle divergence and hypertonicity – as the abdomen enlarges, the muscles of its walls stretch, diverge, and in the back area shorten, which causes pain , especially when bending over, carrying heavy objects, or squatting.
- Hormonal changes:
- During pregnancy, the level of relaxin and progesterone increases. Hormones prepare the musculoskeletal system for childbirth - they reduce the rigidity of the symphysis pubis, increase the elasticity of the pelvic ring and facilitate the passage of the child through the birth canal. They help wash calcium out of the mother's bones - the mineral is necessary for building the fetal .
Mechanical and hormonal factors lead to additional stress on the joints, feet, and spine , causing deformation, flat feet, and pain .
Rice. 1. Mechanical cause of neuralgic syndrome during pregnancy
Low back pain can cause spondylolisthesis. The lumbosacral joint is exposed to hormones pregnancy The area where of the spine transitions into the fixed sacrum does not have powerful muscles that stabilize the region . Increased body weight and a strong “bending” in the area of the L5 and S1 vertebrae leads to disc prolapse and the development of spinal disease - spondylolisthesis and the formation of an intervertebral hernia in the future.
The disease begins with minor, periodically occurring back pain . After physical activity, the pain radiates to the legs, the muscles of the limbs weaken. Pain is noted in the joints of the legs, in the area of the symphysis pubis, and the coccyx . Spasm of the muscles surrounding the spine leads to a decrease in motor activity.
During childbirth, back pain does not go away. She is called:
- sprain of ligaments and muscles during the passage of the fetus through the birth canal;
- birth injuries - divergence of the pubic symphysis, displacement of the hip and vertebral joints.
If the baby was heavy or the fetal was larger than the pelvic ring, then the likelihood of sprains and injuries increases. The risk group includes women with obesity, spinal diseases and connective tissue abnormalities. According to statistics, scoliosis ranks first in the causes of neuralgic pain in women in labor, and osteochondrosis ranks second.
Diseases can cause terminal conditions of a woman during childbirth, provoke hemodynamic disturbances, pulmonary and heart failure. Deformation of the spine causes changes in the location of the pelvis - with scoliosis, it is placed obliquely, and with kyphosis , the transverse size of the entrance to the pelvis is reduced, which makes it difficult for the baby through the birth canal and causes asphyxia of varying degrees of severity.
Restoring the structures of the musculoskeletal system takes considerable time, even if a woman had no problems with the spinal column before pregnancy. Why does my back hurt after childbirth ? “Memory” of tissues retains sensations in the postpartum period. Such pain is described by the woman as nagging, dull, worsening after physical activity. Chronic diseases of the spine that worsen during the gestation period can cause acute, shooting, burning pain . Its severity depends on the severity of the pathology.
About 65% of women who have undergone physiological childbirth report back pain . Of them:
- 70% in the first and second trimester of gestation;
- 30% immediately after birth.
Scientists have found out why the lumbar region hurts after childbirth . In the postpartum period, neurological syndromes are caused by the following:
- deterioration of blood supply to the neural structures of the lumbar spine ;
- impaired transport of electrolytes and swelling of the soft tissues of the back ;
- degenerative-dystrophic changes in vertebral and intervertebral discs.
The lower back and tailbone hurt after an error during epidural anesthesia.
After childbirth, the back and spine hurt , because... a young mother carries a baby for a long time, staying in an uncomfortable position and increasing the overload of the lower back and muscles of the whole body . The pain radiates under the shoulder blade , in the lower back, tailbone . It feels like a burning sensation, the strength of the sensation decreases after rest.
If your lower back continues to hurt 6-8 weeks after giving birth, the pain cannot be ignored. It is a symptom of serious disorders of the musculoskeletal system and pelvic organs.
Further actions
The question often arises of what to do if your back hurts badly for a long time. As soon as the pain becomes more pronounced or does not go away after 3-4 days, you should consult a doctor or follow general recommendations to reduce the severity of pain.
Such recommendations include:
- limit lifting heavy objects or children - a woman should avoid sudden lifting or bending so as not to strain her back muscles;
- change the sleeping position to one in which the mother feels comfortable and the pain is less pronounced;
- if your back does not stop hurting for too long, and the pain syndrome becomes more and more pronounced, it is recommended to take a painkiller (this can be either a local ointment or oral tablets);
- contact your doctor or therapist for diagnosis and determination of etiology.
[node:field_similarlink]
Pain after epidural anesthesia
Women who have undergone epidural anesthesia during childbirth often associate the appearance of back pain with the manipulation performed. But in fact, this method of pain relief is extremely rarely the cause of back pain.
What is epidural anesthesia
Epidural anesthesia is used during childbirth - both natural and caesarean sections - as well as during operations on the urinary system and lower extremities.
The anesthesiologist makes an injection and injects a painkiller (anesthetic) into the space between the spine and the membrane of the spinal cord, after which you will no longer feel pain below the injection site, and you will also temporarily (while the anesthetic is active) be unable to move your legs or feel touch from the lower ribs to the tips of the toes.
Such anesthesia is much easier to tolerate than general anesthesia - an epidural has less impact on the overall well-being and functioning of internal organs, and recovery after the procedure is faster. Nevertheless, many patients unfairly consider this manipulation to be the cause of long-term back pain.
Back pain that patients complain about after epidural anesthesia can be divided into two groups: pain directly related to the procedure, and pain for other reasons.
Pain associated with manipulation
In the vast majority of cases, pain after epidural anesthesia goes away on its own within a few hours or days. This may include:
- Point pain at the injection site. Like many medical procedures, epidural anesthesia can cause discomfort for the patient. In this case, they are associated with damage to the ligaments and muscles at the injection site. Unpleasant sensations may bother you for the first few hours after the end of epidural anesthesia. They usually go away without treatment, do not pose a threat to life and health, and therefore you should not worry about pinpoint pain.
- Pain along the nerves that radiates to one or both legs. These sensations are associated with irritation of the nerve roots during injection and administration of the medicine. A “shooting” type of pain is characteristic, usually appearing immediately after the injection and quickly passing without treatment. Don't worry, this is a normal reaction of the body to an epidural.
Pain caused by complications during epidural anesthesia occurs very rarely (less than 1% of all procedures performed). Their cause may be vascular injury or infection at the injection site. Pain at the injection site does not occur immediately, but after several hours; it can have a different nature and clinical manifestations (weakness and loss of sensation in the legs, urinary incontinence, increased body temperature and other symptoms may occur). In this case, you should immediately consult a doctor; there may be a serious danger to your health.
Pain due to other reasons
Most often, the cause of long-term back pain that patients complain about after epidural anesthesia is an exacerbation of existing back problems. For example:
- an uncomfortable position of the patient during surgery can provoke an exacerbation of arthrosis of the joints of the lumbar spine/sacrum or intervertebral hernia;
- Bearing a child and childbirth themselves can cause overload and strain on the ligaments, muscles and joints of the lumbar spine and pelvic bones, which leads to back pain during pregnancy and its intensification after childbirth.
Studies have shown that epidural anesthesia is an extremely rare (less than 0.05%) cause of long-term back pain. However, there is a so-called risk group: overweight patients, as well as those with intervertebral hernias. They experience pain somewhat more often than the average population.
It also happens that back pain is psychological in nature. The very fact of an “injection in the back” can lead to pain in the back in some patients - so-called psychosomatic pain.
Psychosomatic and neurological pain can bother you for months and even years, but they are not directly related to epidural anesthesia. If the discomfort is severe or continues to bother you for a long time, then you need to consult a neurologist.
Examination and treatment
Since pain is most often not associated with epidural anesthesia, a neurologist may recommend further examination in the form of MRI of the spine and electroneuromyography (a study of impulse transmission along nerves) to determine the real causes of pain.
Treatment usually includes a short course of nonsteroidal pain medications (eg, ibuprofen, diclofenac), physical therapy, and manual therapy (if there are no contraindications to it).
Remember: pain directly associated with epidural anesthesia is short-term and usually goes away without treatment. If you experience or increase pain after this procedure, be sure to consult a doctor.
Be healthy!
Maria Meshcherina
Photo istockphoto.com
Related products: (ibuprofen), (diclofenac)
Diagnosis
Diagnostic methods allow you to find out exactly why your back hurts after childbirth and what was the cause. These methods of analysis include: examination by the attending physician or gynecologist - palpation of the lower back and abdomen is carried out in order to determine tumors or tissue deformations; instrumental diagnostics - the patient is referred to one of the methods of instrumental diagnostics (CT, MRI or radiography).
Computed tomography and radiography are based on the use of x-rays, which are recorded by a special device in the tissues of the subject. The doctor may additionally prescribe the administration of a contrast agent, which will enhance the visualization of the body structures being studied. The main contraindication to the administration of a contrast agent is the period of lactation.
A woman must refrain from breastfeeding for several days until the contrast agent has completely left the body.
Magnetic resonance imaging uses electromagnetic radiation to diagnose structural changes in tissue or neoplasms of various etiologies. Unlike CT, this technique is safe and suitable for girls who suffer from claustrophobia, since diagnostic devices are of the open type.
Magnetic resonance imaging is prescribed when the doctor suspects diffuse degenerative pathologies of the back
Diagnosis for back pain
Neuralgic pain in pregnant women is conventionally divided into:
- gestational;
- non-gestational.
Gestational pain is caused by natural (physiological) reasons and will go away on its own after childbirth. Non-gestational pathologies are caused by various pathologies and they need to be diagnosed in a timely manner. The doctor does the following step by step:
- interviews the patient;
- analyzes the anamnesis;
- conducts physical examinations - examination, measurements, palpation, checking tendon reflexes, determining pain and temperature sensitivity;
- examines the range of movements, posture, gait.
Rice. 2. Methods for diagnosing neuralgic syndrome during pregnancy
To exclude gestational pain, the following studies are prescribed:
- clinical blood and urine tests;
- hormonal levels;
- pathology markers;
- biochemical examination of vaginal smears.
For acute and chronic pain, the listed methods are sufficient to make a diagnosis. If there are neurological and somatic signs, the doctor prescribes instrumental studies:
- Ultrasound;
- MRI;
- CT.
X-rays are not performed for pregnant women.
When your back hurts badly after childbirth , the doctor prescribes the tests listed above and may refer you for a consultation to specialists - a neurologist, endocrinologist, gastroenterologist, etc.
Treatment
Depending on the etiology, the treatment of painful sensations and the factor that caused them is selected. In case of weakened back and abdominal muscles, the doctor recommends therapeutic exercises, the purpose of which is to strengthen the muscular corset of the back and reduce the load on the spine.
Back cushion for the spine
This gymnastics consists of a number of exercises:
- It is necessary to find a vertical, flat surface, and then lean on it so that the shoulder blades, heels, gluteal and calf muscles are in contact with the surface. Next you need to lift one bent leg in turn, then the other. The leg should be fixed for 15–20 seconds. Number of repetitions: 15 times on each leg.
- Bend and twist your torso in different directions. All actions should be slow so as not to damage weakened back muscles. Number of repetitions: 10–20 times on each side.
- Standing on all fours, bend your back first up, then down. The torso should be parallel to the floor. The number of approaches is 15 times with fixation for 10 seconds.
In addition to exercise, your doctor may recommend medications such as Paracetamol, Diclofenac or Ibuprofen. Self-prescription of drugs is not recommended, since it is necessary to take into account the lactation period and general contraindications.
No ads 2
Additional therapy for pain and discomfort is therapeutic massage and wearing a bandage after childbirth. The bandage supports the muscles of the back and abdomen, making it easier for a woman to bear heavy loads and long walks.
Ibuprofen is a non-steroidal anti-inflammatory drug whose action is aimed directly at the site of inflammation. It effectively relieves severe pain, inflammation, swelling and discomfort in the back area
Myofascial pain syndromes localized in the back
O. V. Vorobyova, Doctor of Medical Sciences, Professor of the State Budgetary Educational Institution of Higher Professional Education First Moscow State Medical University named after. I. M. Sechenova Ministry of Health of the Russian Federation, Moscow
At an outpatient clinic, patients with back pain make up from 30% to 50% of patients, depending on the doctor’s specialization. The etiology and mechanisms of formation of back pain are extremely variable.
There are at least four most significant factors leading to pain:
structural changes in cartilage tissue (pathology of intervertebral discs, degenerative arthritis);
chronic muscle dysfunction (tension, spasm);
damage to the nerve fiber primarily due to compression (disc herniation, osteophyte, spinal canal stenosis);
psychological factors contributing to the complex components of psychosocial dysfunction.
In most patients, pain is caused by a combination of several factors that are the source of primary pain and/or support the persistence of pain. Musculo-ligamentous disorders almost obligately accompany back pain, and sometimes are the root cause of pain. They often remain unrecognized, which is due to the low awareness of medical specialists. The pathology of the musculo-ligamentous apparatus of the back is most clearly reflected by myofascial pain syndrome (MPS), characterized by muscle dysfunction and the formation of local painful compactions in the affected muscles. Approximately a quarter of all unilateral back pain syndromes are caused exclusively by MFS. How to diagnose myofascial pain?
Diagnosis of myofascial pain is based on anamnestic characteristics of pain and clinical examination. It is important to determine the type, intensity, duration and location of pain, as well as the factors influencing the intensity of pain. What facts should be clarified in the anamnestic? Particular attention should be paid to the facts of possible muscle injury. For acute pain, it is important to determine what movement caused the pain and test the muscles involved in that movement. With the gradual development of pain, it is important to examine chronically overworked muscles that are subject to microtrauma.
What examination should the clinician perform? Clinical examination necessarily includes assessment of passive and active movements and muscle tone. MFS is characterized by an asymmetric restriction of the motor pattern. An integral part of the diagnosis of MFS is muscle palpation and identification of trigger points (TP). When examining the effector muscle, extremely sensitive “nodules” called trigger points are palpated within the spasmodic muscle cords. Most researchers recognize palpation as the main method for diagnosing MFS; with sufficient knowledge of this technique, it is possible to identify 85–90% of TT. TTs localized superficially or in the area of localized spasm are most easily detected. To more accurately identify the localization and activity of TP, it is advisable to first relax the spasmodic, painful muscles. For this purpose, the post-isometric relaxation technique or, in the absence of special skills, passive mechanical relaxation can be used.
Depending on the location and volume of the muscle, various palpation techniques can be used (direct pressure on the TT with fingers, superficial palpation, pinch palpation). For superficially located small muscles, gentle palpation is performed with the fingertips. Easily accessible muscles (eg, sternocleidomastoid, upper trapezius, hip adductor, and others) are grasped between the thumb and fingers and the muscle fibers are passed between the fingers (pinch palpation). Finally, deep palpation is used for deep-lying muscles (gluteal, piriformis and others). It is necessary to wait 2–5 seconds after finger pressure on the TT and evaluate the reproducibility of the referred pain. The effectiveness of the method increases when using topographic maps of the favorite location of TP in muscles. Associated dermatomal sensitization and trophic swelling can be assessed using skin plucking. Additional research methods (electromyography, algometry, thermography, ultrasound techniques) play a supporting role in the diagnosis of MFS, since they have low sensitivity and specificity. How to clinically evaluate a trigger point? On palpation, the trigger point is felt as a clearly limited area of sharp pain. The CT size on average varies between 2 and 10 mm. Usually it is detected along one cord as the most painful point. When palpating the active TT, pain is observed under the examiner’s finger and in the usual pain zone (zone of referred pain).
The intensity of the pain often reaches such an extent that the pain leads to a rejection reaction (jumping symptom). Active trigger points can also cause non-painful phenomena. The most common vegetative symptoms are: local vasospasm, local hyperhidrosis, pilomotor activity. Paresthesias may be equivalent to pain phenomena in the reflected zone. It is generally accepted to distinguish active and latent myofascial TP. In the active form, there is constant pain, decreased muscle elasticity, and the development of referred pain in response to direct pressure on the TT. The intensity of pain and the length of the pain zone depend mainly on the degree of excitability of the TT. Latent TT demonstrates the same clinical characteristics as active points, but is significantly less pronounced. In addition, in the latent form, the pain is induced rather than constant. The induced pain is usually localized to the area of the affected muscle and the referred area. Some researchers believe that latent TTs may be associated with the genesis of muscle spasm. Potentially, they can reorganize into an active state. In addition, TTs can be classified into primary and secondary. Primary are called TPs, which are formed as a result of acute or chronic overload of the muscle concerned and whose activity is not related to the activity of other muscles. Secondary or satellite TTs are the result of mechanical stress and/or neurogenic inflammation due to the activity of primary TTs. In the absence of supporting factors, TTs may spontaneously disappear if the muscle remains at rest for several days. On the contrary, negative factors, and most importantly, the persistence of the influence of the original pathogenic factor, contribute to the formation of secondary triggers and an increase in the area of pain. Thus, the main clinical markers of MFS, summarizing the clinical picture, are: local or regional pain, limiting range of motion; palpation determination of hypertonicity in the affected muscle with areas of increased sensitivity within the “tight” cord (trigger point); reproducibility of pain when trigger points are stimulated; reduction of pain when stretching the affected muscle.
What factors contribute to the formation of MFS in the back? The formation of the MFS is based on both the characteristics of the muscular system bearing the postural load and specific load factors. The actual anatomical features of the back muscles, namely the absence of long tendons with close interaction between the muscles, paraspinal ligaments and fascia, make these muscles especially vulnerable to the formation of MFS. In addition, the muscles of the back and neck are among the least trained, which limits their functional reserve. Loading factors vary somewhat at different levels of the spinal column.
1. Cervical level. Myofascial pain syndromes are the most common cause of pain in the neck, shoulder, and headaches. This is the reason why neck pain occurs in 30–85% of people. Chronic strain of the neck muscles is most often a consequence of: anti-physiological postures associated with work organization disorders (improper sitting at a school desk, when working with a computer monitor, etc.); neck position during sleep (pillow features); postural adaptation of the neck in the presence of primary pain in adjacent regions (shoulders, temporomandibular joint, etc.). Acute injury to the musculo-ligamentous system of the neck is most often associated with an acceleration/deceleration type injury (extensor mechanism of injury). Most whiplash injuries occur in transportation accidents, but they can occur in other situations, such as diving.
2. Lumbar level. Instability of the motion segment most often leads to overload of the trunk muscles. A decrease in the elasticity of the disc fibers and dehydration of its matrix is the cause of the most common functional disorder in the motion segment - hypermobility of the intervertebral disc. At an early stage, this is compensated by contraction of the trunk muscles. However, the functional reserve of the muscle is limited and depends on the training of the muscles. Muscle tissue can be injured during single or recurrent episodes of biomechanical overload. Modern working conditions expose the back muscles to additional overload associated with muscle imbalance. For example, with a sedentary lifestyle, the human body is subjected to static loads most of the time, at this time dynamic muscles are constantly inhibited and gradually become flabby, while at the same time postural muscles contract and gradually lose elasticity. Chronic muscle imbalance is characteristic of modern urbanization. Also, various postural disorders, such as scoliosis and other skeletal asymmetries, can contribute to muscle overstrain.
3. Pelvic level. MFS affecting the pelvic floor muscles occur almost exclusively in women [1]. This is primarily due to the anatomy of the female body and the structural changes that the female body experiences during reproductive life. During puberty after menarche, the girl's pelvis expands, the gluteal muscles increase in volume, and the hips rotate inward, leading to a lateral displacement of the patella. Constant internal rotation of the hips can negatively impact the pelvic diaphragm, which increases a woman's risk of developing pelvic floor spasms in the future. Pregnancy or weight gain increases this risk. Normally, the kneecap extends beyond the second toe, which helps maintain stable balance when standing. In many women, due to lateral deviation of the patella, the mobility of the joint decreases, which leads to a flattening of the arch of the foot. These structural changes in the lower extremities lead to disruption of the physiological maintenance of balance when standing and to excessive stress on the pelvic floor muscles. Ligaments in women are more extensible than in men, which is a necessary condition for maintaining joint stability and ensuring the process of physiological childbirth, but at the same time, this ability is a predisposing factor in the formation of fascial and ligament dysfunction in women. A fall on the buttocks can lead to limited mobility of the sacrum and the appearance of pelvic pain due to tension in the ligamentous apparatus of the pelvic floor muscles. In humans, the lower half of the body has more mass than the upper. Insufficiently developed muscles and muscle hypotonia can aggravate lumbar lordosis and increase the forward tilt of the pelvis. Increased lumbar lordosis is also observed during pregnancy. The reduction of estrogen during menopause is the main factor in the disruption of the physiological curves of the spine in old age. Changing the natural curves of the spine creates additional stress on the muscular frame, especially on the pelvic floor muscles. How to diagnose secondary muscle pain? Regardless of the primary source of pain and its pathogenetic characteristics, the muscles of the trunk are involved in the pathological process, becoming secondary sources of pain. Secondary pain occurs in the skeletal muscles outside the spinal motion segment due to a reflex increase in muscle tone. The physiological basis for muscle tension that follows any pain lies in the immobilization of the affected area of the body, the creation of a muscle corset. However, the muscle spasm itself leads to increased stimulation of the muscle's nociceptors. An increase in the flow of nociceptive impulses increases the activity of motor neurons in the anterior horns and contributes to increased muscle spasm. A reflex tonic muscle tension is formed. An additional factor in the development of painful muscle spasms is the antalgic posture. Transferring weight to one leg leads to curvature of the torso and asymmetrical position of the pelvis with the subsequent development of pain in the sacro-lumbar joints and the muscles that provide movement in these joints. The nature of secondary muscle pain is dull, aching, and pulling. Their intensity can vary widely. From a diagnostic point of view, it is important that pain is provoked by movements and is significantly intensified in positions in which the muscles surrounding the spinal column are stretched. Pain can also intensify when maintaining the same position for a long time (driving a car, sleeping in an uncomfortable position, long flight, etc.). There are no symptoms of loss.
With lumbar musculoskeletal pain, pseudo-Lasegue syndrome can be observed. If, when performing the Lasegue test, pain occurs only locally in the lower back, or hip, or under the knee, or in the lower leg, this is due to a stretch of spasmodic muscles (paravertebral or posterior thigh muscles) (“short” pain). On palpation, the paravertebral muscles are compacted, tense, and painful. Secondary muscle pain can become chronic and persist on its own even after the original cause has been eliminated. How to treat myofascial pain? Treatment of MFS requires multipronged approaches. Standard treatment includes: drug therapy with drugs such as nonsteroidal anti-inflammatory drugs (NSAIDs) and muscle relaxants; impact on TT, including physiotherapy; therapy aimed at restoring the normal functioning of muscle tissue: reducing muscle strain, strengthening the muscle frame, changing lifestyle. The main short-term task is to destroy trigger points, which leads to pain reduction. But the impact on TT should not be carried out in isolation. The long-term goal is to relax the muscles, restore the balance between postural and dynamic muscles, and neutralize predisposing factors, which reduces the risk of recurrence of pain. Warming the muscle can help it relax; for this, applications of “warming” ointments, gels, as well as hot wet wraps of the affected muscle, and wet warm compresses can be used. If you have certain skills, TT can be mechanically destroyed by injection of anesthetics (novocaine, lidocaine), which shortens the period of pain associated with the procedure. TT injections can provide excellent results. Less commonly used is “dry needling” without the use of an anesthetic. Specialized centers use muscle stretching exercises and gentle muscle relaxation techniques, such as post-isometric relaxation. In addition, traditional relaxation massage can be effective. The duration of therapy is significantly reduced with rapid and effective pain relief for the patient. Pain relief with NSAIDs is generally accepted for MFS - Nise, Diklak, Brufen SR, Movalis, etc. The prescription of NSAIDs is mandatory for any severity of pain - from mild (NSAID monotherapy) to severe (in combination with other drugs). Applications to painful areas of gels and ointments containing NSAIDs or their general dosage forms (tablets, suppositories, injection forms) can be used. The combination of NSAIDs and muscle relaxants in the treatment of MFS has become almost standard, making it possible to reduce treatment time. In addition, the simultaneous use of muscle relaxants and NSAIDs allows you to reduce the dose of the latter and, therefore, avoid the development of side effects of therapy. While taking muscle relaxants, post-isometric muscle relaxation, massage, and physical therapy are facilitated. It has been proven that the use of muscle relaxants makes it possible to rid the muscle not only of active, but also of latent TP, i.e., it improves the long-term prognosis, reducing the recurrence of MFS. Randomized controlled trials demonstrate the superiority of this class of drugs over placebo.
A study conducted by the Cochrane Physicians Society, which included over thirty controlled trials, also confirmed the usefulness of the use of benzodiazepine and antispastic muscle relaxants [2]. Domestic researchers prefer non-benzodiazepine central muscle relaxants. Usually tizanidine, tolperisone, and baclofen are used. These drugs have fewer side effects than benzodiazepines. Tizanidine (Sirdalud) is a prominent representative of central muscle relaxants. The drug is registered for the treatment of painful muscle spasm caused by musculoskeletal diseases and spasticity. The combination of tizanidine with NSAIDs demonstrates a more pronounced effect on pain reduction compared to NSAID monotherapy in patients with back pain [3, 4]. In addition to reducing pain, tizanidine reduces the need for NSAIDs and tranquilizers in patients, thereby reducing potential side effects from treatment. Placebo-controlled studies have shown the actual analgesic effect of tizanidine, as well as its effect on muscle tension and reduction of active trigger points [5]. Therapeutic tactics completely depend on the severity of the pain syndrome, its duration and the number of muscles affected by the MFS. In acute MFS, Sirdalud can be used in monotherapy. The recommended daily dose of Sirdalud is 6 mg per day in 2 or 3 divided doses. For severe MFS, combination treatment is used, combining pharmacological and non-pharmacological methods. Adding Sirdalud to a comprehensive treatment regimen allows you to reduce the duration of taking NSAIDs and avoid taking tranquilizers. Since the mild sedative effect of Sirdalud allows you to cope with mild anxiety without prescribing psychotropic therapy. Adjuvant treatments (antidepressants, anxiolytics, hypnotics): There are no high-quality randomized controlled trials on the use of these agents in patients with MFS. But numerous studies show the effectiveness of these drugs for treating chronic pain. It should be noted that chronic pain is often associated with depression, and effective treatment of depression can significantly reduce pain. The presence of comorbid syndromes requires mandatory targeted therapeutic efforts. A necessary component of treatment is the patient's physical activity. It is necessary to recommend that the patient return to normal daily activities. Physical therapy has a positive effect. Avoiding postural tension, daily physical therapy, mastering autogenic training with the ability to relax muscles is an effective defense against muscle pain. It is necessary to encourage the patient to make a positive change in life style (avoidance of anti-physiological poses, rational equipment of the workplace, stopping smoking, weight control, physical therapy, annual massage courses, mastering autogenic training with the ability to relax muscles).
Literature Vorobyova O.V. Painful spasm of the pelvic floor muscles as a cause of chronic pelvic pain in women // Farmateka. 2011, no. 5 (218): 51–55. Van Tulder MW, Touray T, Furlan AD, Solway S, Bouter LM Cochrane Back Review Group. Muscle relaxants for nonspecific low back pain: a systematic review within the framework of the cochrane collaboration // Spine. 2003, Sep 1; 28 (17): 1978–1992. Berry H., Hutchinson DR Tizanidine and ibuprofen in acute low-back pain: results of a double-blind multicentre study in general practice // J Int Med Res. 1988; 16:83–91. Pareek A., Chandurkar N., Chandanwale AS et al. Aceclofenac–tizanidine in the treatment of acute low back pain: a double-blind, double-dummy, randomized, multicentric, comparative study against aceclofenac alone // Eur Spine J. 2009; 18 (12): 1836–1842. Lepisto P. Muscle relaxants for nonspecific low back pain: a systematic review within the framework of the Cochrane Collaboration // J Int Med Res. 1981; 9 (6): 501–505.
The article was published in the journal The Attending Physician
Source: https://medblog.su/prochie-tematiki/miofastsialnye-bolevye-sindromy-lokalizovannye-v-oblasti-spiny.html © medical portal MedBlog.su
Link to publication: medblog.su
Prevention
To prevent back pain after childbirth, experts and doctors recommend adhering to the following preventive measures. Maintain an even posture. If there is curvature of the spinal column in different directions (kyphosis, lordosis or scoliosis), the girl should monitor her posture during pregnancy and perform gymnastic exercises that will help strengthen the back muscles.
Regardless of the presence of spinal pathologies, perform physical exercises that strengthen the muscular corset (in particular, the lumbar region). This could be swimming, gymnastics, yoga or gym classes. To prevent back pain due to heavy loads on the body and weight gain, a girl should monitor her body weight. You should not eat large amounts of fatty foods. It is important to remember that the more weight, the more pressure placed on the spinal column.
Choose the right orthopedic mattresses and other bedding items. Improper sleeping posture can cause discomfort and discomfort throughout the day. You should lead an active lifestyle and sit as little as possible. Staying in a sitting position for a long time causes discomfort and nagging pain in the lower back, which is something a pregnant woman needs to remember.
After childbirth, you should stop lifting heavy objects and carry your baby with care. Holding a baby for a long time can affect weakened back muscles. You should also take care of the surrounding space and objects. After giving birth, a girl is not recommended to bend over too low, so it’s worth adjusting the diaper changing table, baby’s crib and other necessary items in advance.
Back pain after childbirth - how to treat
If your back hurts after childbirth, treatment should begin after examination and consultation with a doctor . During this period, the mother is feeding the baby , so the use of most analgesics and anti-inflammatory drugs is undesirable. The main method of treatment at the Manual Medicine Clinic “Galia Ignatieva MD” is physiotherapy:
- massage of the lumbar area to enhance microcirculation, relieve pain , eliminate muscle ;
- exercises to strengthen the muscle corset and increase the elasticity of ligaments;
- gymnastics to strengthen the pelvic floor and intimate muscles ;
- exercises in the pool and balneological therapy to eliminate muscle hypertonicity.
Some experts advise resorting to unconventional methods of therapy - acupuncture, vipro- and pressotherapy. But such treatment must be agreed with the doctor .
The lower back will not hurt if you maintain physical “hygiene” during the postpartum period:
- avoid sudden movements – bending, turning;
- do not lift weights, especially jerking;
- distribute weight when carrying loads.
Drug therapy involves symptomatic treatment - the use of warming ointments, painkillers, analgesic injections if the lower back continues to hurt .
Rice. 3. Manual therapy after childbirth.
Therapeutic massage and spinal can only be performed by an experienced vertebrologist at the Manual Medicine Clinic “Galia Ignatieva MD”. The spine will stop hurting if you wear a special bandage or corset that relieves stress from the muscles and holds the spinal column in a physiological position.
The lower the load on the spinal column, the less your back will hurt . Once you normalize your weight, the pain will go away if there are no organic changes. A nutritionist will help you create the right diet.