Laser vaporization of the intervertebral disc is an outdated type of nucleoplasty procedure , which has ceased to be used within our neurosurgical department with the advent of cold plasma and other types of nucleoplasty technologies. This type of treatment was widespread in the 90s and many clinics purchased expensive equipment for it, which they are still forced to use. In Europe, this type of treatment is prohibited due to the disadvantages described below.
The essence of the nucleoplasty procedure and its varieties
Nucleoplasty is the general name for operations to treat intervertebral herniation, during which the nucleus pulposus of the intervertebral disc is affected in order to change it. The word nucleoplasticity comes from two words: nucleo (nucleus) and plastic (change).
The essence of the nucleoplasty procedure is that an electrode (or a needle, a light guide, etc.) is inserted into the core of the intervertebral disc using a puncture method (through a 2-3 mm puncture) under the control of intraoperative X-rays, through which pulses of cold plasma (either an electromagnetic field or mechanical action is performed, etc.). The impact on the nucleus pulposus of the disc leads to its evaporation, as a result of which the pressure of the disc on the fibrous ring decreases. Due to the decrease in pressure, the bulging of the fibrous ring into the lumen of the spinal disc decreases and it stops putting pressure on the nerve root, resulting in a rapid reduction in pain.
There are several types of nucleoplasty technologies:
- Cold plasma nucleoplasty (coblation) - exposure to a beam of cold plasma (the most popular technology);
- Radiofrequency ablation - exposure to an electromagnetic field;
- Hydroplasty - exposure to pressure of saline solution;
- Interventional discotomy - mechanical action (newest technology);
- Laser vaporization (laser treatment) - laser exposure (this technology is outdated and is not used in our country).
Nonspecific spondylitis as a complication after laser vaporization of the intervertebral disc
Introduction.
The prevalence of low back pain is so high that 80% of all people will experience acute back pain at least once in their lifetime [2, 3, 4, 5, 6, 7]. The most common causes of chronic lumbar pain and radicular pain are intervertebral disc herniation, spinal canal stenosis, intervertebral disc degeneration without herniation and spinal cord syndrome, which lead to significant economic, social and medical costs [1].
Magnetic resonance imaging allows you to identify various pathological changes in the spine and assess the degree of deformation of the spinal canal. Prescription of bed rest, muscle relaxants, non-steroidal anti-inflammatory drugs, B vitamins, anticholinesterase drugs, and sometimes glucocorticosteroids, as well as physiotherapeutic procedures, relieve ischiolumbalgia in most cases. Persistent pain in the lower back and lower extremities is relieved by epidural and paravertebral injections of glucocorticosteroids. Failure of conservative therapy is an indication for surgical intervention.
The development of surgery for degenerative diseases of the spine is moving along the path of developing minimally invasive treatment methods to reduce the trauma of the operation and reduce complications [8, 9, 10, 11].
One of the minimally invasive methods for treating herniated intervertebral discs is the method of percutaneous laser vaporization. The laser energy is transferred to the nucleus pulposus through the fiber. The fiber is placed through a fine needle through a posterolateral percutaneous approach under local anesthesia. Absorption of laser energy leads to vaporization of water inside the nucleus pulposus and a change in the structure of its proteins, which leads to a decrease in volume and a decrease in intradiscal pressure and, as a consequence, to decompression of the compressed nerve root. The first laser disc decompression operation was performed in Europe by Choy and colleagues in 1986.
To date, sufficient experience has been accumulated in the use of laser decompression of intervertebral discs, and the literature describes cases of aseptic and infected discitis after this procedure. We wanted to report a case from our practice of the development of spondylitis of two adjacent vertebrae after laser vaporization of the VL4-5 intervertebral disc.
Case from practice
Patient A.B. 50 years old, applied to the Republican Scientific and Practical Medical Center F&P with complaints of sharp pain in the lumbar spine, pain spreading to the lower extremities, increased pain when moving, limitation of movements.
From his medical history he considers himself sick for 8 months. The disease began with pain in the lumbar spine. He was treated conservatively with a diagnosis of Osteochondrosis of the lumbar spine. Herniated intervertebral disc VL4-5 measuring 6 mm. Secondary spinal stenosis, radicular syndrome, took NSAIDs, physiotherapy, epidural blockade with glucorticoids, without effect. General blood test from accompanying documents: Hb-117 g/l; eryth-3.5; Color ref.-0.9; leukocytes-5.5; Pal.poison -1; Seg.poison-60; Eoz.-4; lymph.-34; Mon.-5; ESR-5 mm/h. After 3 weeks of ineffective therapy, laser vaporization of the VL4-5 intervertebral disc was performed under local anesthesia; in the postoperative period, cefazolin 1.0 IM 2 times a day was prescribed for 10 days. After the intervention, clinical improvement was noted. However, after 2 months, the patient began to experience pain in the lumbar spine, an increase in body temperature to 38 degrees, the patient was given a course of antibiotic therapy: broad-spectrum antibiotics and NSAIDs for 20 days, the temperature returned to normal and the patient was discharged for rehabilitation treatment. After 2 months, the patient comes to us with the above complaints.
The patient grew up in satisfactory social conditions. Married, has three children. There are no hereditary diseases. Denies the presence of chronic diseases. There are no medications taken on a regular basis. Denies contact with a tuberculosis patient. 1 BCG scar 5 mm. He did not suffer from infectious diseases and was not in contact with them, did not receive blood or blood products, and did not go to the dentist. No allergies to medications or food products were noted. Works as a mechanic.
The general condition of the patient is relatively satisfactory. Consciousness is clear and adequate. The pupils are equal in size, the reaction to light is preserved. From the side of the cranial nerves without pathology. There are no meningeal symptoms. The skin and visible mucous membranes are clean. Peripheral lymph nodes are not enlarged. Subcutaneous fat is moderately expressed. The chest is of asthenic type. Breathing through the nose 20 per minute. Percussion pulmonary sound over the entire surface of the lungs. The lung boundaries are within normal limits. Auscultation reveals vesicular breathing in both lungs. Heart sounds are rhythmic and muffled. A/D – 120/80 mmHg, pulse – 88 beats. in 1 min., satisfactory filling and tension. The tongue is moist and clean. The abdomen is soft and painless. The liver and spleen are not palpable, stool is regular. Pasternatsky's symptom is negative on both sides. Diuresis is regular and free.
Local status. The patient cannot move independently due to pain in the lumbar spine. The limb axes are correct. Active and passive movements in the joints are free. The spine is straight, the lumbar lordosis is smoothed, the paravertebral muscles are reflexively tense. Lasègue's sign is positive on both sides at 30 degrees. Wasserman's sign is positive on both sides. With deep palpation, there is a sharp pain in the projection of the VL4-5 vertebrae, the pain spreads to the lower extremities, more to the left. Parasthesia is noted in the proximal parts of the lower extremities. Skin sensitivity, peripheral pulsation and muscle strength are preserved.
Upon admission, general blood test hemoglobin was 140 g/l; red blood cells - 3.8 × 1012; color index - 0.9; leukocytes - 5.0 × 109; stab - 1; segmented - 59; eosinophils - 4; lymphocytes - 32; monocytes - 4; ESR - 17 mm/h. General urine analysis: color - yellow; transparency - slightly turbid; reaction - acidic; no protein; epithelial cells - 0-1 in the field of view; leukocytes - 2-3 per field of view; red blood cells - 0-1 in the field of view, salts - oxalates. Biochemical analysis: AST-0.36 mmol/l; ALT - 0.50 mmol/l, total bilirubin - 10.5 mmol/l; urea – 5.7; creatinine-78 µmol/l; blood sugar – 6.2 mmol/l. Coagulogram: hematocrit - 50%; thrombotest - VI; prothrombin index - 84%; fibrinogen - 4.25; recalcification – 1'55''; clot retraction - 53%; fibrinogen activity - 15%. Diaskintest is negative. ECG: sinus rhythm 88 per minute, horizontal EOS, dystrophic changes in the ventricular myocardium. Ultrasound of the abdominal cavity and retroperitoneal space without echopathology.
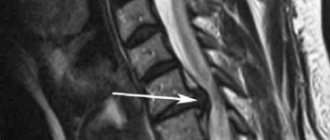
On MRI, the signal in VL4-5 bodies is heterogeneously reduced. The interbody gap is narrowed. The articular surfaces are uneven with urination, with marginal osteophytes. The soft tissues around are infiltrated, thickened, and there are no abscesses. The spinal canal is narrowed. Due to protrusion of the discs of VL4-5, VL5-S1 vertebrae. Increased signal from the bodies of the remaining lumbar vertebrae.
On the chest x-ray: pulmonary fields without infiltrative shadows. The roots of the lungs are structural. The sinuses are free. The diaphragm domes are of normal shape. Heart shadow without features.
The patient was prescribed NSAIDs, anti-inflammatory, decongestant and detoxification treatment: Diclofenac sodium 75 mg IM 1 time per day No. 7; NaCl 0.9% - 200.0 + CaCl 10% - 10.0 IV once a day No. 10; Glucose 5% - 200.0+ Vit C 6.0 IV 1 time per day No. 10; furosemide 1.0 IM 1 time per day No. 10, Vitamin B6 1.0 IM 1 time per day No. 10. Levofloxacin at a dose of 750 mg daily No. 20.
In the dynamics of a general blood test, hemoglobin is 140 g/l; red blood cells – 4.0 × 1012; color index - 0.9; leukocytes - 5.6 × 109; ESR-15 mm/h, the rest of the analysis without features. On dynamic MRI after 3 weeks, the infiltration decreased, but persisted, the pathological signal from the VL4-5 bodies persisted. Clinically, there is sharp pain when moving in the lumbar spine with pain spreading to the lower extremities, spinal instability.
The patient underwent necrectomy VL4-5, with opening of the spinal canal, spinal fusion with a titanium mesh cage from the left anterolateral approach. During the operation, the following is noted: instability of the VL4-5 segment, destruction and sequestration of bone tissue. The histological conclusion of the surgical material is nonspecific spondylitis.
In the postoperative period, broad-spectrum antibiotics were prescribed for 10 days to prevent the development of a secondary infection. The postoperative wound has healed initially.
The patient was activated in a brace 3 weeks after surgery and was discharged home in satisfactory condition.
The final diagnosis was made: Osteochondrosis of the lumbar spine. Intervertebral disc herniation VL4-5. Secondary spinal canal stenosis, radicular syndrome. SPO laser vaporization of intervertebral disc VL4-5. Os.: spondylitis of VL4-5 vertebrae of a nonspecific nature.
| Rice. 1. MRI before laser vaporization of intervertebral disc VL4-5 |
| Rice. 2. MRI on admission |
| Rice. 3. MRI after 20 days of Levofloxacin therapy |
Discussion
In percutaneous laser decompression of the intervertebral disc, laser energy is used to reduce intradiscal pressure by vaporizing the small nucleus pulposus, which reduces the pressure between the nucleus pulposus and the annulus fibrosus, thus leading to retraction of the hernial protrusion and freeing the nerve root.
Vijay S. et al, 2013 reports that in vitro, an increase in intradiscal volume of 1 ml leads to an increase in intradiscal pressure of 312 kPa or 2340 mmHg. On the other hand, a decrease in intradiscal pressure leads to a significant decrease in intradiscal pressure, which, according to the principle of negative pressure, directs the hernial protrusion to the center of the intervertebral disc, decompression of the nerve root and relief from radicular pain. In addition, vaporization of water leads to denaturation of the nucleus pulposus protein, which prevents the subsequent accumulation of water [12].
Percutaneous intervertebral disc decompression is not believed to cause serious complications, other than the fact that recent studies indicate minimal risk if the procedure is performed by an experienced surgeon. Potential complications include: infection, bleeding, nerve damage, increased pain, recurrent hernia, paralysis, idiosyncrasy, anaphylactic shock, and death. Nerve root damage may occur during insertion of the cannula. An experienced surgeon performs the procedure under real-time imaging control and with the patient fully conscious to ensure that this complication does not occur. Damage to blood vessels may occur if an artery or vein contacts the device, especially if thermal energy is used, resulting in necrosis of the vessel wall. Care must also be taken not to bury the device in the anterior portion of the annulus fibrosus.
According to the literature, the level of complications after laser vaporization of the intervertebral disc is 0.5%. In a study by Choy et al., 1998 [14], in 4 of 518 patients the procedure was complicated by discitis, which was less than 1%. Farrar et al., 1998 [15] reported a case of osteomyelitis in a 50-year-old man after laser decompression of the intervertebral disc for a VL4-5 disc herniation. In a study that followed patients for 3 months after laser vaporization, McMillan et al., 2004 [16], indicated an increase and recurrence of low back pain in 63%. However, it was reported that no cases of infection, nerve damage, or clinically significant bleeding were observed [13].
Conclusion: The use of laser energy and other thermal energy can lead to thermal injury not only of cartilaginous structures, but also of bone structures and feeding vessels, which is manifested by their necrosis and manifests itself clinically months after surgery.
Literature:
- Vasiliev A. Yu., Kaznacheev V. M. “Puncture laser vaporization of degenerated intervertebral discs.” M., 2005.S. 128.
- Boswell MV et al. "Interventional techniques in the management of chronic spinal pain: Evidence-based practice guidelines." Pain Physician 2005; 8:1-47.
- Bressler HB et al. “The prevalence of low back pain in the elderly. A systematic review of the literature". Spine 1999; 24:1813-1819.
- Lawrence RC "Estimates of the prevalence of arthritis and selected musculoskeletal disorders in the United States." Arthritis Rheum 1998; 41:778-799.
- Cassidy JD et al. "The prevalence of low back pain and related disability in Saskatchewan Adults." Spine 1998; 23:1860-1867.
- Walker BF et al. "Low back pain in Australian adults: Prevalence and associated disability." J Manipulative Physiol Ther 2004; 27:238-244.
- Guo HR et al. "Back pain prevalence in US industry and estimates of lost workdays." Am J Public Health 1999; 89:1029–1035.
- Wang JC et al. “The effect of uniform heating on the biomechanical properties of the intervertebral disc in a porcine model.” Spine J 2005; 5:64-70.
- Welch WC et al. "Alternative strategies for lumbar discectomy: Intradiscal electrothermy and nucleoplasty." Neurosurg Focus 2002; 13:E7.
- Helm S et al., “Effectiveness of thermal annular procedures in treating discogenic low back pain.” Pain Physician 2012; 15:E279-E304.
- Magalhaes FN et al. "Ozone therapy as a treatment for low back pain secondary to herniated disc: A systematic review and meta-analysis of randomized controlled trials." Pain Physician 2012; 15:E115-E129.
- Vijay S. et al. “Percutaneous Lumbar Laser Disc Decompression: An Update of Current Evidence” Pain Physician 2013; 16:229-260.
- Vijay S. et al. "Percutaneous Lumbar Laser Disc Decompression: An Update of Current Evidence" Pain Physician. 2006; 9:139-146.
- Choy D.S. "Percutaneous laser disc decompression (PLDD): twelve years' experience with 752 procedures in 518 patients." J Clin Laser Med Surg 1998; 16: 325-331.
- Farrar MJ. "Possible salmonella osteomyelitis of spine following laser disc decompression." Eur Spine J 1998; 7:509-511.
- McMillan MR et al. "Percutaneous laser disc decompression for the treatment of discogenic lumbar pain and sciatica: a preliminary report with 3-month follow-up in a general pain clinic population." Photomed Laser Surg 2004; 22:434-438.
Disadvantages of laser vaporization
With laser vaporization, the core of the disc is exposed to a high-temperature (up to 400°) laser beam, which damages adjacent tissue. That is why in modern neurosurgical centers laser vaporization is replaced by more modern technologies - cold plasma and other types of nucleoplasty. For example, with cold plasma nucleoplasty, the disc core is exposed to a plasma cloud at a temperature of 70°, which makes this procedure more delicate and safe, but no less effective.