September 24, 2019
18490
0
3.5 out of 5
Spondylodesis is a surgical procedure that is a type of arthrodesis. The purpose of the operation is to immobilize one or more spinal motion segments. This is achieved through the installation of special structures that reliably fix the vertebrae to be fused together. As a result, over time they firmly grow together, which completely eliminates the possibility of movement and the development of painful sensations against this background.
The need for spinal fusion arises in many spinal pathologies that are not amenable to conservative treatment. Therefore, it is usually combined with other surgical interventions. Spine surgeons at SL Clinic will help you get rid of spinal problems and perform spinal fusion. We have already managed to help many hundreds of patients with various diagnoses, and we will help you return to a full, active life without pain.
Indications for spinal fusion
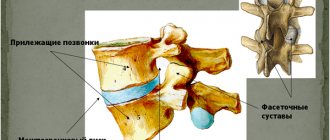
The need to eliminate the mobility of the vertebral motion segment arises with spondylolisthesis, instability of the vertebrae, which is accompanied by severe pain. The vertebral motion segment of the spine is called its structural and functional unit, which consists of two adjacent vertebrae, a disc located between them, as well as a facet joint and their ligaments.
The causes of vertebral instability most often lie in severe osteochondrosis, in which the intervertebral discs are severely destroyed and completely lose their functionality. As a result, a large number of patients additionally develop not only intervertebral hernias, but also arthrosis of the facet joints, compression of the spinal cord and its nerve roots.
Each of these conditions is accompanied by severe pain, which in almost half of the cases cannot be treated with conservative methods. Therefore, in such cases, patients are prescribed surgical intervention appropriate to the situation, followed by spinal fusion. It could be:
- facetectomy, indicated for severe spondyloarthrosis;
- decompression of the dural sac, necessary for compression of the spinal cord;
- meningoradiculolysis, used for the formation of adhesions in the area of the spinal roots.
Most often, patients undergo removal of intervertebral hernias and installation of special cages in place of the resected intervertebral discs. Only such an integrated approach ensures complete elimination of pain syndrome and reliable prevention of their occurrence in connection with damage to the same spinal motion segment in the future.
Indications for spinal fusion after releasing compressed nerves and removing severely damaged intervertebral discs are:
- displacement of the vertebrae (spondylolisthesis);
- arthrosis of the facet (arc-shaped) joints;
- cicatricial adhesive epiduritis;
- congenital or acquired instability of the spine;
- severe kyphosis, scoliosis grade 3–4;
- osteochondrosis, accompanied by discogenic pain;
- regularly recurrent radicular syndrome due to various reasons;
- herniated discs leading to compression of nerves or the spinal canal;
- neoplasms in the spine of any origin;
- spinal canal stenosis;
- compression fractures of the spine that occur due to osteoporosis;
- cracks, fractures and other spinal injuries.
In each individual case, the spinal surgeon strictly individually selects the type of intervention performed and develops a step-by-step plan for the operation. To do this, he requires laboratory results, MRI, CT or X-rays.
When developing tactics for surgical treatment, existing concomitant diseases and the financial situation of the patient must be taken into account. At SL Clinic you can undergo a comprehensive diagnosis of the spine and receive help from leading neurosurgeons who regularly perform decompression and stabilization operations with high success rates. The cost of all types of operations and diagnostic methods is given in the price list.
Postoperative recovery
Surgery on the cervical spine is complex and requires careful implementation of a number of measures:
- After surgery, complete regeneration will take several months. To limit neck movement and provide support, a neck brace is often recommended after surgery. Limiting neck movement promotes effective fusion of the vertebrae. It is important that the patient rests.
- Patients are advised to resume slow walking as soon as possible after surgery. It is necessary to gradually increase the duration of walking, and if the patient has difficulty walking in the first few days after surgery, then it is better to avoid walking. Before starting walking, you should consult with your doctor. It is advisable to walk 10-15 minutes a day.
- Avoid lifting heavy loads, bending, performing overhead work with arms, and sudden or forceful turns of the neck. Do not carry out any activities that put stress on the neck muscles. Driving is also not allowed after surgery. The patient needs to join exercise therapy classes 3-4 months after surgery. But physical exercise is possible only after the bones have fused properly.
- The length of time it takes for the bones to completely fuse (fuse) varies from patient to patient. It also largely depends on what method was used to surgically fuse the bones. If the surgeon used the patient's own bone or instrumentation for surgical fusion, then the bones will fuse quite quickly, in about 3-4 months. But, if a bone graft from a donor is used, then it takes a longer time for the bones to fuse (within 6-9 months). Recovery time will be further prolonged if the patient is overly physically active, performs work with the arms above the head, and holds the neck arbitrarily in any direction. Every day the patient experiences less discomfort. The time required for the patient to return to normal activities will also vary. Some may take 3-6 months, while some may take a year to fully heal.
- If the patient notices any signs of infection, swelling, redness or thickening at the site of surgery or incision, then he must see his doctor. To treat severe pain after surgery, your doctor may prescribe narcotic pain medications. Gradually, as the pain decreases, the doctor moves on to conventional analgesics. Certain pain medications and nonsteroidal anti-inflammatory drugs (NSAIDs), such as aspirin, naproxen, ibuprofen, and COX-2 inhibitors, should be avoided for several months after surgery.
- Follow-up scheduled appointments with the attending surgeon are absolutely necessary to evaluate the recovery process and verify the reliability of the surgical implants or artificial disc. If there is persistent pain, the doctor may prescribe certain diagnostic tests, such as MSCT or MRI, EMG (ENMG). It is also important that the patient takes the medications prescribed by the doctor in a timely manner.
- Smoking is a big enemy on the road to recovery. Smoking should not be resumed after surgery because nicotine disrupts or interferes with the bone healing process, which is necessary for successful fusion. Smoking also increases the risk of complications after surgery.
- Diet is another important aspect of recovery. The patient must eat a healthy and nutritious diet to allow muscle and bone tissue to recover. It is necessary to include animal proteins in the diet, as they contain all the essential amino acids, while vegetarian sources do not contain some amino acids. A balanced diet helps in healing and recovery.
- Family members and loved ones should provide support to the patient so that he/she can get rid of emotional stress. The patient experiences a lot of stress during the surgery and hence good care and support from the family members after the surgery will be of great help in mitigating the stress.
Types of spinal fusion
Decompression and stabilization operations can be performed through an anterior or posterior approach. But more often, preference is given to the posterior one, since performing the anterior approach is more technically difficult and is accompanied by significant injury to soft tissues, which entails the risk of severe bleeding and a high likelihood of complications.
In the posterior type, the surgeon is able to perform manipulations on the spine, cutting the skin, fascia and pushing the deep back muscles to the sides. This allows for less tissue trauma, therefore less likely to lead to undesirable consequences and ensures an easier and faster rehabilitation period. Spinal fusion through the posterior approach in the vast majority of cases became possible thanks to the creation of titanium cages, which contain bone chips. These are special implants installed instead of removed intervertebral discs. They replaced bone or artificial implants and significantly increased the safety and effectiveness of surgical intervention.
If it is still impossible to perform the operation via a posterior approach, an anterior approach is chosen. It involves making an incision on the front surface of the neck, and if it is necessary to perform surgery on the lumbar region, the surgeon creates access to the spine through the abdominal cavity. This is mainly practiced when:
- comminuted fractures of the spine;
- scoliosis;
- a number of degenerative-dystrophic diseases.
There are also differences in the methods of fixation of the vertebrae during spinal fusion. When choosing the anterior method, the neurosurgeon stabilizes the vertebral bodies. If the posterior fixation technique is chosen, the surgeon works with the spinous and transverse processes of the vertebrae.
But according to studies, interbody fusion is especially effective. Since the vertebral bodies are much better supplied with blood, have a larger number of cellular elements and have a high potential for the formation of new bone tissue, objects implanted between them take root much better than those installed between the processes of the vertebrae. With this method of fixation, successful spinal fusion can be achieved in 96% of cases. Otherwise, the vertebrae may not fuse, which will lead to continued back pain and serious consequences in the future.
Posterior Fusion Surgery
Spine surgery can be performed on any part of the spine, from the neck to the tail. In this case, an incision is made at the back of the spine and the bones are fixed in place in various ways to heal. This operation is performed in several different ways.
Posterolateral groove fusion
In this case, spine surgery is performed from the back through a seven to 12 cm long intermediate incision. A bone graft is taken from the pelvis and placed in and out of the back of the spine. This area has many arteries, and the nutrients needed for the transplant are supplied through the blood.
Part of the vertebrae in this area acts as a muscle connection. In order for the graft to be firmly anchored, these muscles are lifted and placed on the graft to provide the necessary pressure and tension to the bone graft.
Posterior lumbar interbody fusion (PLIF)
Unlike the previous method in PLIF, fusion is performed directly in the disc space by placing allograft bone fusion or synthetic materials (PEEK or titanium). When this surgical procedure is performed from the back, it is called (PLIF).
To do this, they make an incision between seven and 15 cm in the back of the waist and remove the psoas muscles from the left and right parts of the vertebra. The allograft structure within the metal shelves is then inserted into the intervertebral space. With the support of this allograft, the vertebral bone grows and fusion occurs.
Transforaminal lumbar interbody fusion (TLIF)
TLIF surgery is performed through the back of the spine. In this method, a fusion spacer is first placed between the vertebrae, and then pedicle screws and rods are used to increase the fusion speed and immobility of the vertebrae. The bone graft used in this surgery is also taken from the patient's pelvic bone. Of course, alternative options can be used.
Spinal fusion of the cervical spine
In case of pronounced degenerative-dystrophic changes in the vertebrae of the cervical spine, posterior cervicospondylodesis using transpedicular fixation is most often performed. If it is necessary to stabilize in one position, 1, 2 or more spinal motion segments may be subject to stabilization. But this method requires a high level of professionalism from the neurosurgeon, as it carries a risk of damage to nerve fibers and blood vessels.
If a high probability of developing such complications is detected at the stage of preoperative preparation, preference is given to installing metal structures to fix the posterior supporting complex of the spinal motion segment. They allow you to connect the processes of the vertebrae, which leads to spinal fusion.
Spinal fusion can also be performed through an anterolateral approach. Indications for its implementation are serious injuries to the cervical spine. In such cases, the method of vertebral fixation is selected for each patient individually based on MRI results. Interbody cervicospondylodesis associated with the installation of an anterior fixation plate is highly effective in the surgical treatment of cervical spine fractures.
As a result of surgical intervention, in most cases it is possible to achieve complete elimination of pain, which allows patients to return to daily activities. In some cases, minor discomfort may occasionally occur that does not affect a person’s ability to work.
How much does the operation cost?
In Moscow, the minimum cost of spinal fusion is 50,000 rubles. In this case, a person must additionally pay for consumables, metal implants, hospital stay and rehabilitation. In total, treatment in Moscow can cost a patient 100,000 rubles.
Nowadays, many residents of the Russian Federation go to Germany and Israel for surgery. There the operation costs between 10-12 thousand euros. Unfortunately, in German and Israeli clinics, patients are discharged within a few days after surgery. As a result, patients do not receive the necessary rehabilitation or undergo it at home. Naturally, all this slows down recovery.
If you want to undergo surgery abroad and receive full rehabilitation, pay attention to the Czech Republic. Treatment there costs much less than in other European countries. For spinal fusion, a stay in the clinic and high-quality recovery in the Czech Republic, you will pay only 7-8 thousand euros.
Spinal fusion of the lumbar spine
In the vast majority of cases, operations on the lumbar spine are performed via a posterior approach with the choice of an interbody method of fixation of the vertebrae. Intervention through the anterior approach is carried out exclusively in complex clinical cases and in case of comminuted fractures.
There are several ways to perform lumbar interbody fusion:
- anterior (ALIF);
- rear(PLIF);
- transforaminal(TLIF).
To ensure that the immobilization of the spinal motion segment is as reliable as possible, the operation is often supplemented with transpedicular fixation. In this case, special metal structures are installed, which further strengthen the fastening of the vertebral bodies.
Anterior interbody fusion
The ALIF technique allows for extremely convenient access to intervertebral discs and vertebral bodies. Thanks to this, the neurosurgeon is able to freely remove the disc, eliminate pathological compression of the nerve roots and spinal canal, and install a cage. If necessary, the surgeon installs additional fixing structures.
When using the ALIF technique, it is possible to bypass the nerve bundles, which eliminates the possibility of their damage and the development of related complications. But it presupposes the need to move blood vessels, which can provoke bleeding.
Posterior interbody fusion
The PLIF method involves removing processes from both sides of the vertebra. This is followed by a radical discectomy. Cages are placed on both sides of the vertebra.
Sometimes they are replaced with expanding implants. Since they are smaller, the neurosurgeon only needs to perform a medial bilateral facetectomy (removal of the facet joints) and remove only the nucleus pulposus of the disc. These implants are equipped with screws. They are unscrewed with a special key, thanks to which the cages are firmly fixed in a given position.
A huge advantage of the technique is the ability to perform circular spinal fusion during one operation. But its implementation carries the risk of damaging the nerves, since the surgeon must push them back to gain access to the interbody space. The main danger of this is the development of paresis, paralysis and disruption of the intestines and urinary organs, which can lead to urinary and fecal incontinence.
Transforaminal spinal fusion
The TLIF technique is recognized as the least traumatic. It involves removing the intervertebral disc and performing spinal fusion on the side of the most severe stenosis.
Transforaminal spinal fusion allows you to preserve the integrity of the posterior supporting structures of the spine and fulfill the entire planned volume even in the presence of significant scar changes.
Possible risks and consequences of the operation
Fortunately, complications with spinal fusion surgery are extremely rare. But, like any other operation, this surgical intervention can cause postoperative complications:
- Bleeding.
- Hematomas.
- Infection of the wound surface.
- Thrombosis.
- Allergic reaction to medications.
- Partial fusion or non-fusion of the bones of the spine.
- Damage to the nerve roots, which, in turn, will lead to severe pain, paralysis, tingling, and numbness in parts of the body.
- Impaired bowel and bladder functions.
Factors that significantly increase the risk of postoperative complications are the patient’s smoking, obesity and unbalanced diet, the presence of other diseases, and the patient’s age.
Contraindications
Spinal fusion cannot be performed if:
- severe diseases of the cardiovascular system;
- recent stroke or heart attack;
- acute infectious diseases;
- exacerbation of chronic diseases;
- formation of fistulas of unknown origin;
- blood clotting disorders;
- varicose veins.
Traditionally, surgical treatment is indicated only for patients aged 12 to 60 years. In other cases, the possibility of surgical intervention is considered by a group of specialists.
Combined Fusion Surgery
Anterior/posterior fusion, or combined fusion surgery, is a procedure in which spinal surgery is performed from the front and back.
Some spine surgeons perform fusion surgery as a combination of anterior and posterior surgery to further stabilize the spine. Studies have shown that surgery on both sides of the lumbar spine increases the rate of fusion. With this method, an incision is made on both the side of the body and the back.
Features of rehabilitation
Spinal fusion is not a simple surgical procedure. The patient spends the first day after it in the intensive care ward under constant medical supervision. If during this time there are no signs of complications developing, positive dynamics are observed, he is transferred to a regular ward and allowed to get up and move independently for short distances.
Discharge from the hospital is carried out at different times, which is determined by the type of operations performed and the extent of spinal fusion performed. The patient receives detailed instructions on the rules of behavior during the rehabilitation period, directions to attend physiotherapeutic procedures and exercise therapy classes.
To speed up reparative processes, patients are prescribed individually selected medications, as well as wearing an orthopedic corset.
On average, it takes 2 to 4 months for the body to fully recover. During this entire time, it is prohibited to perform heavy physical work, lift weights, or sit for long periods of time.
If all recommendations received are strictly followed, patients return to a full life and do not suffer from limited mobility, especially when performing mono- and bisegmental spinal fusion. Minor difficulties can arise only when several spinal motion segments are fused during bending.
Decompressions and fusion
Sometimes the surgeon will perform decompression and fusion. For example, after a discectomy, space appears between the vertebral bodies. This gap is usually filled with a bone graft (from the patient's pelvic bone or from donor bone) or a spacer, which supports the spine and promotes fusion. This type of surgery is called an anterior cervical discectomy and fusion, or ACDF.
Many surgeons use fixation devices (plates with screws) in the anterior surgical approach to perform ACDF or corpectomy. These devices help improve fusion stability.
Spinal fusion at SL Clinic
“SL Clinic” has comfortable reception areas, treatment rooms, wards, modern diagnostic equipment and operating rooms equipped with the latest technology. We are constantly improving and trying to create the best treatment conditions for patients with various spinal diseases.
The cost of spinal fusion starts from 410,000 rubles and depends on: - Spinal diseases (displacement of the vertebrae or narrowing of the spinal canal, etc.) - Implant manufacturer; — Clinic (where the operation will be performed) and the class of the ward. — The number of vertebrae that need to be stabilized. The price includes: — Stay at the clinic before and after surgery; — Implants. — Operation; - Anesthesia; — Observation and consultation during the rehabilitation period. All clinic services and costs are listed in the price list.
Our spinal surgeons have been helping you achieve pain relief and a high quality of life for over 10 years. They regularly master new methods of conservative and surgical treatment, which will allow them to combine experience and modern approaches to treatment.
If you don't have back pain, contact SL Clinic.
Why does the cage shift in the spine?
Most often this happens for two reasons:
- Failure to comply with surgical technology, for example, installing a T-pal without a transpedicular system;
- Gross violation by the patient of the treatment regimen and immobilization regimen - refusal to wear various orthoses after surgery.
Author of the article: neurosurgeon Anton Viktorovich Vorobiev Frame around the text
Why choose us:
- we will offer the most optimal treatment method;
- we have extensive experience in treating major neurosurgical diseases;
- We have polite and attentive staff;
- Get qualified advice on your problem.
What operating techniques does the Gelenk Clinic offer?
Depending on the cause of the pain, surgeons at the Gelenk Clinic in Gundelfingen offer the patient various surgical techniques.
Nucleoplasty
Nucleoplasty is an endoscopic operation designed to treat incomplete intervertebral hernia. If the fibrocartilaginous tissue around the core of the intervertebral disc protrudes and compresses the spinal nerves, nucleoplasty can help cure this disease without the need for open surgery. To do this, the operating surgeon inserts a high-frequency electrode into the damaged intervertebral disc through a special puncture needle. Using an electric probe and the presence of X-ray equipment that allows you to carefully observe the movements of the instruments, the doctor reduces the size of the core of the intervertebral disc until it no longer compresses the spinal nerves. The chances of success with this minimally invasive surgery are very high. Thanks to this operation, almost 80% of patients were able to relieve pain and return to their previous lifestyle.
Intervertebral disc endoprosthetics
A cervical endoprosthesis can replace the original shape of the intervertebral disc.
© Spinal Kinetics For ten years, artificial intervertebral discs have been an effective and widespread treatment method. In addition, this operation is also a promising alternative to the proven spinal fusion, an operation that blocks individual vertebral bodies. Intervertebral disc replacement is also aimed at restoring the natural functions of the intervertebral disc. The goal of this surgery is to relieve or normalize symptoms associated with disc degeneration and herniation, such as chronic back pain and neurological disorders. The endoprosthesis replaces the real intervertebral disc, stabilizes the spine and protects it from subsequent injuries. At the Gelenk Klinik medical center, M6-C type prostheses are used during this operation. Such disc prostheses last a lifetime and do not need to be replaced.
Spinal fusion
A progressive form of wear and tear on the spine often reduces the distance between the vertebrae. Thus, the space between them narrows, which leads to destabilization of the spine and displacement of the vertebral bodies forward, backward or to the side. If conservative treatment methods do not bring the desired result and minimally invasive operations do not help the patient, the technique of immobilizing the painful area is the only solution. The combination of special screws and connecting components ensures immobility of the operated area. Thanks to modern medicine, this operation is performed minimally invasively, through small incisions. It is worth noting that spinal fusion does not provide the patient with complete relief from pain, but only reduces pain in the spine.