Scheuermann's kyphosis, also known as Scheuermann's disease, juvenile kyphosis, or juvenile discogenic disease, is a hyperkyphosis in which there is a wedge-shaped deformation of three or more adjacent vertebrae by ≥ 5 degrees.
The thoracic spine is most often affected, but the thoracolumbar and lumbar spine are no exception. The photo shows a 22-year-old man with severe Scheuermann's disease (before surgery).
Scheuermann's disease
- Most often, the disease is diagnosed at the age of 12-17 years. The reason for visiting a doctor is usually the concern of parents who are worried about their child’s poor posture or hunched back.
- Pain in the area of hyperkyphosis may also be a reason for examination.
- Scheuermann's disease is the most common cause of kyphotic spinal deformity in adolescents.
There are two forms of Scheuermann's kyphosis:
- Thoracic, when the apex of the deformity is located at the level of the Th7-Th9 vertebrae.
- Thoracolumbar form, in which the apex is located between the Th10–Th12 vertebrae. It is highly likely that this form will progress during puberty.
Clinically Relevant Anatomy
Curves of the spine
The adult spine has a natural S-shape. The cervical and lumbar regions are curved forward; these curves are called lordosis. The thoracic and sacral sections are curved backward; these curves are called kyphosis. According to the Scoliosis Research Society, the normal kyphotic angle in the thoracic spine is 20-40 degrees. If the magnitude of the kyphotic curve is greater or less than the specified value, then in this case we speak of spinal deformity.
Friends, the seminar “Scoliosis: types, causes, treatment” will take place very soon. Find out more...
With Scheuermann's disease, structural deformation of the vertebral bodies and the spine as a whole occurs. With this disease, the kyphotic angle in the thoracic region is about 45-75 degrees. In addition, wedge-shaped deformation of three or more adjacent vertebrae occurs by 5 degrees or more. The wedge-shaped vertebral bodies determine the nature of hyperkyphosis, which is observed in Scheuermann's disease. Hyperkyphosis can be compensated for by lumbar or cervical hyperlordosis.
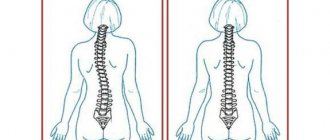
Symptoms
A normal spine appears straight when viewed from behind. However, a spine affected by kyphosis indicates an anterior curvature of the spinal bones (vertebrae) in the upper back, giving a person an abnormally rounded or “humpbacked” appearance. This anomaly manifests itself at an early age and is more common in children aged 12 years. In this case, the curve can be fifty degrees or more. This leads to problems such as:
- Frequent shortness of breath due to compression of the respiratory organs.
- Poor mobility of the ribs.
- Development of heart diseases.
- Liver dysfunction and urinary incontinence.
And these are just some of the problems that arise from a curved spine.
Etiology
There is still no clear and generally accepted opinion on the etiology of Scheuermann's kyphosis.
- It is assumed that heredity plays a role, but the mechanism of transmission of the disease is not yet known.
- The theory connecting the disease with impaired mineralization and ossification of the vertebral plate during the growth of a teenager has gained some popularity. As a result of these disorders, the vertebral bodies begin to grow disproportionately and become wedge-shaped, which in turn leads to the appearance of kyphosis. This theory is confirmed by the results of histological studies.
- Other theories include mechanical, metabolic, and endocrinological causes, but the actual cause is still unclear.
Classification of curvature
There are seven types of kyphotic posture, differing from each other both due to the development and severity of deviations.
Types of kyphotic posture:
- Embryonic – develops in the womb due to abnormalities of the neural tube. The pathology can only be corrected through surgery.
- Congenital – a consequence of birth injuries, as a result of improper behavior of a woman, the use of obstetric forceps or a vacuum aspirator. If the deviation from the norm is no more than 30%, conservative correction is possible. For more severe deviations from the norm, surgical intervention will be required.
- Mycobacterial - deformation develops as a result of infectious damage to the vertebrae by harmful bacteria. It can be treated primarily through surgery.
- Hereditary - kyphotic posture appears as a result of a dominant trait of inheritance.
- Myotonic – formed with a pronounced myotic syndrome, accompanied by impaired contraction and relaxation of muscles.
- Angular - not a round, but a peculiar angular shape is formed on the spine.
- Compression-kyphotic posture appears against the background of injuries, fractures and damage to the spine.
In elderly people, senial curvature of the spine is diagnosed, caused by impaired blood supply to the bones, weakness of muscles and ligaments, and lack of calcium.
Features/Clinical manifestations
X-ray in lateral projection
According to Sorenson, Scheuermann's kyphosis is characterized by the following criteria:
- Three or more adjacent vertebrae have a wedge deformity of ≥ 5 degrees.
- There are no congenital pathologies of the spine, as well as infectious diseases and injuries.
A teenager with Scheuermann's kyphosis will experience:
- Cosmetic defect/postural deformity.
- Subacute chest pain is likely, usually without a specific trigger. The pain increases with activity and decreases with rest.
- Most often, the deformity is detected in early and middle adolescence. It is usually noticed either by the child himself or his parents, or it is detected during school medical examinations.
- Physical examination reveals a rough, hyperkyphotic curve with pronounced curvature.
- Hyperkyphosis does not disappear either during extension or in the supine or abdominal position, which only confirms the high degree of rigidity of this deformity.
- Cervical or lumbar hyperlordosis, scoliosis, and tension in the hamstrings may also be detected. Although neurological disorders are rare in Scheuermann's disease, a thorough neurological examination of the patient is recommended.
- Muscle stiffness and fatigue may occur, especially at the end of the day.
- Reduced flexibility of the torso.
- In severe cases, heart and lung function may be impaired or severe neurological symptoms may occur. These symptoms are extremely rare.
Patients may also complain of pain that prevents them from exercising, working, or doing daily activities. The disease can also cause discomfort due to its aesthetic component.
During the examination, it is possible to detect skin pigmentation in the area of greatest curvature due to friction against the backs of chairs. The natural history of the disease remains an open question, with many conflicting reports regarding the severity of pain and physical disability.
Causes of poor posture
The causes are congenital and acquired.
Congenital changes occur due to abnormalities in intrauterine development or injury to the fetus during childbirth. These are wedge-shaped vertebrae, connective tissue dysplasia, dislocation of the atlas (1st cervical vertebra), myotonic syndromes (torticollis and the like). Congenital abnormalities account for no more than 10% of all lesions. The vast majority of causes of poor posture are acquired. The predisposing factor is asthenic constitution. Postural deformities are provoked by factors such as low physical activity, a heavy briefcase (especially in combination with the habit of carrying it in one hand), insufficient lighting in the classroom, which is why the child’s body is in a non-physiological position for a long time.
Some actions of parents who want the child to sit down or walk ahead of the time prescribed by nature also do not contribute to the formation of correct posture. The desire to “teach” a child whose spine is not yet mature to sit or walk does not end well.
The spine suffers from severe systemic diseases: polio, tuberculosis, flat feet, consequences of injuries, shortening of one leg. Poor vision and hearing (myopia, strabismus, hearing loss) interfere with the formation of correct posture, when the child is forced to approach the source of sound or image, holding his back in a forced position almost constantly. Incorrect posture also occurs in children with underweight or excess body weight, when muscles do not have the opportunity to develop normally.
Diagnostics
A thorough history, physical examination, and lateral and anteroposterior radiographs are necessary to evaluate Scheuermann's kyphosis. Lateral radiographs are required for diagnosis. Diagnostic criteria are:
- Severe hyperkyphosis of more than 40 degrees.
- Anterior wedge deformation of the vertebral body of 5 degrees or more (in three or more adjacent vertebrae).
Radiographs also reveal:
- Irregular shape of the supporting areas of the vertebral bodies.
- Schmorl's hernia.
- Reduced height of the intervertebral space.
- Scoliosis.
- Spondylolysis / Spondylolisthesis.
- Disc herniation.
MRI is not normally required, but may be needed to assess anatomical changes and to prepare for surgery. There is no need to do a CT scan. There is also no need for laboratory tests or histological studies.
When is surgery needed?
It is important to understand that all methods of conservative treatment have a short-term effect and are used primarily to eliminate pain and stiffness in the affected segment of the spine. The only way to restore normal posture in patients with grade 3-4 kyphosis is an operation called osteosynthesis. This type of treatment involves the installation of fixing metal structures (plates) for the purpose of long-term elimination of mobility of certain bone structures. If the operation is performed correctly and the patient continues to comply with the prescribed regimen, remission can last quite a long time - up to 7-10 years.
Before and after surgery
Performance evaluation criteria
Distance between the wall and the back of the head (Occiput to Wall Distance).
Patients can fill out the following questionnaires themselves. The collected data can be used both before treatment and after surgery.
- Scoliosis Research Society Instrument (SRSI): This questionnaire provides information on activity level, pain, etc.
- Back pain and disability scales: Visual Analogue Scale (VAS), Quebec Back Pain Disability Scale (QBPDS), Roland-Morris Disability Questionnaire, Oswestry Disability Index (ODI) and SF-36
Stages
There are four stages of kyphotic posture:
- By visual examination, only a specialist can determine kyphosis at the initial stage. There is a slight bulge and impaired muscle tone. The patient himself does not feel any discomfort and lives a normal life.
- Signs of a “round back” become noticeable, the head tilts slightly forward, and the shoulders drop slightly. The deviation from the norm ranges from 30% to 50%, but to make a final diagnosis it is necessary to undergo an X-ray examination.
- A constant stoop appears, which not only spoils the appearance, but can also affect the functioning of the internal organs. Patients with kyphosis often complain of difficulty urinating, problems with defecation, and shortness of breath during prolonged physical activity. The curvature is 60% or more; even with a straight back, the curvature cannot be hidden.
- The most severe form of kyphosis, accompanied by the formation of a pronounced hump. The patient experiences severe pain in the spine, is often limited in movement, and is not physically active.
Survey
- The main distinguishing feature of patients with Scheuermann's disease is thoracic kyphosis.
- Often, along with kyphosis, the patient is found to have cervical or lumbar hyperlordosis.
- Cervical lordosis can be increased with head protraction. The shoulders are mostly directed forward.
- These disorders may be accompanied by mild or moderate scoliosis.
Patients with Scheuermann's disease usually have well-developed muscles, in contrast to patients with postural kyphosis.
The examination consists of:
- Posture Assessment: Body position is assessed from the front, back and side.
- Neurological screening: in rare cases, compression of the spinal cord along the posterior surface of the vertebral bodies may occur at the site of greatest curvature. This may result in symptoms of impending paraplegia with clonus and hyperreflexia.
- Adam's forward-bend test: Scheuermann's kyphosis may be accompanied by scoliosis.
- Muscle Shortening Test: In Scheuermann's disease, the following muscles may be stiff: the pectoralis major, hamstrings, suboccipitals, and hip flexors. Contractures in the shoulder and hip joints are possible.
- Range of motion in the joints of the lower extremities and spine.
- Muscle Strength Test: The strength of the abdominal, core, trunk extensors, and gluteal muscles should be tested.
How to recognize the problem?
Symptoms manifest differently for everyone. Below are the most common:
- Difference in shoulder height.
- The head is tilted forward compared to the rest of the body.
- Differences in the height and position of the shoulder blades.
- The upper back goes up significantly when the child leans forward.
- Tight muscles in the back of the thigh (hamstring).
It is worth considering that the symptoms may turn out to be other back problems. For example, it is the result of injury or infection. It is best to consult a specialist to make a diagnosis.
Treatment
Conservative treatment
Stretching, lifestyle modification, NSAIDs, +\- physical therapy.
Indications:
- Asymptomatic course of the disease, kyphotic angle less than 60 degrees.
Application:
- Most patients fall into this category.
- Patients generally cope well with rehabilitation tasks. Long-term or significant complications usually do not occur.
Corset therapy
Indications
- Kyphosis 60-80 degrees, +/- presence of symptoms.
Application:
- Wearing a corset is recommended for a period of 12-24 months.
- The following types of corsets are recommended: Milwaukee corset, Kyphologic corset, Boston corset for the thoracolumbosacral region.
- Most effective for children whose skeleton has not yet fully formed.
- Typically, braces do not reduce the arch, but rather inhibit its progression.
Surgical treatment
Spinal fusion, which typically involves an anterior incision and arthrodesis.
Indications:
- Kyphotic curve greater than 75 degrees, causing severe deformity.
- Kyphotic curve greater than 75 degrees, pain.
- Neurological disorders/spinal cord compression.
- Severe pain that cannot be treated.
Application:
- Most patients note an improvement in symptoms, as well as correction of kyphotic deformity.
- Operative and postoperative complications must be taken into account.
Prevention of poor posture
The best prevention is an age-appropriate sleeping place with an orthopedic mattress and pillow, clothes and shoes with stable soles, wearing a backpack instead of a briefcase, and sufficient lighting of the study area.
The child must be consulted by an ophthalmologist and an ENT doctor, and the identified violations must be corrected.
Children with incorrect posture should be observed by a pediatric orthopedist, whose recommendations should be strictly followed. Sufficient physical activity, sports, and games with physical activity are required.
Specialists at the SM-Doctor clinic will conduct a preventive examination of a child of any age and advise on all the necessary measures to correct posture. The center uses innovative diagnostic and treatment methods. Contact the best specialists who know how to make your child’s posture perfectly straight!
Physical therapy
Non-surgical treatment
For a child or adolescent with the initial stage of the disease, it is enough to undergo an examination by a physical therapist, who will assess the condition of the kyphotic arch. The patient should also be counseled about body position and types of activities that are beneficial to him. This can be limited to until the patient’s kyphosis begins to worsen or the pain intensifies.
- In some children, the disease regresses over time without leaving pathological kyphosis or creating long-term problems.
- Others may permanently have a slight thoracic kyphosis, which, however, will not prevent them from functioning normally and will not cause pain or other problems.
Your doctor may recommend brace therapy along with exercises.
- The corset is most effective during the period when the child’s skeleton is not fully formed, which usually occurs by the age of 14.
- Ideally, a corset should be started at puberty and worn for two years. After the final maturation of the skeleton, the corset may not be worn.
- Most doctors prescribe the Milwaukee corset, which is made of molded plastic. It corresponds to the size of the waist and serves to support the shoulders and gradually straighten the chest arch. The corset has two soft straight plates aligned along the spine. The pressure from these plates straightens the spine. A corset will not eliminate a kyphotic arch if the spine is fully formed. In addition, the corset is useless for severe curvatures with an angle of more than 75 degrees.
Corset therapy
- Patients under 15 years of age usually wear corsets all day, removing them only when showering.
- The brace should be adjusted regularly to improve the kyphotic deformity.
- When the situation has improved sufficiently, the corset can be worn part-time (8-12 hours a day). So it should be worn until the skeleton is completely formed, which usually happens by the age of 14-15.
- Sometimes wearing a corset also helps adults, despite the fact that their skeleton has long been formed. We are talking about partial correction of kyphosis and pain relief. Corset therapy is also recommended to reduce pain in cases where surgery is not possible.
Physical therapy is recommended in combination with brace therapy
- It appears that exercise enhances the benefits of wearing a brace by strengthening the muscles, which helps align the spine.
- Recommendations from physical therapists regarding maintaining posture and beneficial activities are of great importance.
- Physical therapy is recommended even if the patient no longer wears a brace, as it helps manage any pain and teaches how to maintain proper body posture. In addition, physical therapy helps identify and treat any muscle imbalances that may be placing mechanical stress on the spine.
Doctors may prescribe anti-inflammatory drugs to relieve pain. Younger patients usually take these drugs for a short period of time and combine them with other treatments. Adults who experience persistent pain sometimes need long-term use of anti-inflammatory drugs.
According to Lowe, bracing is almost always successful if the kyphosis angle is between 55 and 80 degrees and if the diagnosis is made before final skeletal maturation.
- Corset therapy has several disadvantages. One of them is that the longer the brace is used, the higher the likelihood of low back pain.
- Compliance among teenagers is usually low.
Other corsets were also tried, in particular soft corsets. However, they have not shown effectiveness: a soft corset is not able to correct gross deformity.
Other Aspects of Physical Therapy
Kyphotic posture can be corrected using the Schroth technique
Examples of exercises using the Schroth method
Patient education includes the following
- Extension based stretching/muscle strengthening program.
- Hamstring stretch.
- Improvement of postural and mechanical components in activities of daily living.
- Optimal use of corset plates.
Working with posture
- Emphasis on stretching the hamstrings and pectoralis major muscles; strengthening and improving the functions of the trunk extensors.
- The exercises will be effective provided that appropriate rigidity has not yet been developed in the thoracic spine and when the sagittal arch is not yet too high (Cobb angle - from 44 to 55 degrees).
- Maintaining posture in standing and sitting positions.
Exercises
- Flexibility exercises - to relieve contractures in the lower extremities (for example, hamstrings).
- Strengthening the core, back extensors.
Sport
- Sports where extension occurs are shown: gymnastics, aerobics, swimming, basketball, cycling and hyperextension exercises.
- Sports involving jumping and excessive functional use of the back are not recommended.
Postoperative physical therapy
Must include breathing exercises, mobilization and muscle strengthening exercises.
Scheuermann's disease in adults
- The approach to treating the disease in adults is different, since the problem of pain comes to the fore, not aesthetics.
- The preferred method of treatment is functional rehabilitation in an outpatient setting. Much less often, the patient is referred for surgery or prescribed to wear a corset.
There is another treatment regimen. Its main principles are described below:
- 1) Elongation and development of the trunk.
- 2) Symmetrical sagittal extension; exercises should be performed on both sides of the body (right and left): Bilateral expansion of the chest in the posteroanterior direction to reduce thoracic hyperkyphosis.
- Bilateral lumbar expansion in an anteroposterior direction to reduce hyperlordosis in the lumbar region.
- Shoulder Traction: Traction increases chest opening and corrects the spine.
- Breathing correction: allows the patient to feel expansion in problem areas. The purpose of breathing exercises is to open the chest in the back to front and lateral directions.
- Muscle activation through increased tension: to achieve the best possible correction results; muscle balance, stabilization and to enhance proprioceptive afferentation. It also helps to build the correct body diagram in the mind.
- This intensive physical therapy combined with wearing a corset (such as SpinoMed) is a successful treatment regimen for Scheuermann's disease in adults.
It should be noted that more clinical studies are needed to evaluate the effectiveness of conservative treatment (especially manual therapy) and various physical exercises. The results need to be compared with the results of wearing a corset, and the effectiveness of these conservative instruments with the simultaneous use of corsets needs to be studied.
How is kyphosis diagnosed in children?
The doctor will be able to make an accurate diagnosis based on the following information: the child's complete health history, physical examination, and the results of certain tests. The healthcare provider will also ask questions about developmental stages, since some types of kyphosis may be associated with other neuromuscular problems.
Only a specialist can make an accurate diagnosis
Your child will also need the following tests:
- X-ray. This test will give a complete understanding of the internal organs, bones and tissues. This way the doctor can measure the angle of curvature of the child’s spine. Treatment is often based on this definition.
- Bone scanning (osteoscintigraphy). This test will help identify any infection or broken bones in your back.
- MRI. This test uses a combination of large magnets, radio frequencies and a computer to create detailed images of organs and structures inside the body. Based on the findings, any other spinal cord and nerve abnormalities will be ruled out.
- CT scan. This test uses X-rays and a computer to take detailed images of the body.
- Blood analysis.
Identifying the true cause of kyphoscoliotic posture at an early stage is important for successful treatment! It is worth considering that as long as the spine can be displaced, it will be much easier to eliminate the disease.
There are 4 degrees of the disease:
- At the first stage, the child does not feel any discomfort. And in a standing position, muscle weakness and slight deviations in physiology are observed.
- The second degree involves a noticeable defect (angle of curvature of about 55 degrees). The x-ray shows noticeable deformities of the vertebrae.
- The third stage is called Hyperkyphosis. With it, the spine has a permanently curved kyphotic appearance and cannot be corrected simply by changing the position of the body.
- At the last stage, the fourth, there is a clear curvature of the body (costal hump). In this case, there is a high probability of surgical intervention.
[node:field_similarlink]