What is arthrosis of the 2nd degree, general information
Answering the question - what is arthrosis of the 2nd degree, we can answer that it is a degenerative-dystrophic disease, accompanied by the gradual destruction of cartilage tissue with subsequent deformation of the joints.
The pathology occurs in a chronic form and is accompanied by the appearance of pain of varying strength. Without timely treatment, arthrosis can lead to limb immobility, causing the patient to become disabled. What is arthrosis
Women are more likely to suffer from osteoarthritis, as they are more susceptible to varicose veins and obesity. A typical picture of arthrosis is that a woman over 40 years old, overweight and leading a sedentary lifestyle may have arthrosis of the knee or hip joint. Unilateral damage to the right knee is more common than to the left. If a degenerative-dystrophic process is observed in several joints at the same time, this indicates a more unfavorable course of the disease.
In older age, the disease is associated with natural wear and tear of the joints. If arthrosis develops before the age of 40, it is preceded by injuries, hypothermia and overload. In the preclinical stage of the disease, pathological changes in the joint tissue are first observed, against the background of which deterioration develops. Over time, the recovery processes deteriorate, which leads to the predominance of destruction of articular tissue over restoration. Next, true arthrosis appears, leading to complete erasure of cartilage.
The mechanism of arthrosis development is associated not only with impaired blood circulation and metabolic processes, but also with the proliferation of osteophytes. The essence of the disease is the gradual replacement of thinned cartilage tissue with bone pathological growths, which contribute to the occurrence of limited mobility. When the cartilage is completely worn away, osteophytes grow large and replace it. This leads to a state of complete immobility.
Pathogenesis
The pathogenesis of osteoarthritis (OA) is based on pathological changes in the molecular structure of hyaline cartilage, in which processes of remodeling (synthesis/degradation) of the basis of cartilaginous tissue, the extracellular matrix . A key role in this process is played by highly differentiated cells of cartilage tissue - chondrocytes , which begin to produce low-molecular proteins of the interstitial cartilage tissue (matrix), which reduces the shock-absorbing properties of the knee joint cartilage.
of proteoglycans in the surrounding cartilage matrix and react negatively to their changes. It is known that the state of cartilage tissue is determined by the balance of anabolic/catabolic processes. At the same time, the speed/intensity of catabolic processes increases under the influence of cytokines (interleukin-1, tumor necrosis factor-α), metalloproteinases (stromelysin, collagenase), cyclooxygenase-2 , which are produced by chondrocytes, cells of the subchondral bone and synovial membrane. Also in the process of restoration of cartilage tissue, a significant role is played by the reparative activity of chondrocytes, which is based on insulin-like/transforming growth factors and morphogenetically altered cartilage/bone proteins.
As a result of the increase in degenerative processes, the cartilage loosens/softens, cracks appear, and the articular surfaces of the bone, due to the destruction of cartilage tissue, begin to experience an unevenly distributed increased mechanical load. This contributes to the appearance of a zone of dynamic overload in the subchondral bone, which causes redistribution disturbances of microcirculation, the development of subchondral osteosclerosis , changes in the curvature of joint surfaces, and the formation of osteophytes (marginal osteochondral growths).
A significant role in the pathogenesis is played by synovitis , characterized by moderately expressed exudative/proliferative reactions in the form of hyperplasia and mononuclear infiltration of the synovial membrane, most manifested in places of attachment to cartilage with subsequent transition to lipomatosis / sclerosis . Exudative-proliferative reactions in the synovial membrane and subchondral bone occur against the background of a disorder of regional microcirculation and hemodynamics with the gradual development of tissue hypoxia . osteophytosis appear in the subchondral bone , and the structure of the changes becomes irreversible. The pathogenesis of OA is schematically presented below.
Reasons for the development of deforming arthrosis
In what cases does arthrosis of the knee joint develop most often:
- Previous injuries. Typically, arthrosis develops after severe dislocations, fractures, bruises and damage to the meniscus, if we are talking about the knee joint. Most often, gonarthrosis occurs before the age of 40 and is associated with injuries. A fracture is a high risk of developing arthrosis in the future, since the limb has to be fixed in a stationary position for a long time. For this reason, circulatory disorders develop, which ultimately leads to degenerative-dystrophic complications. If the patient also underwent surgery to remove the menisci, then in 90% of cases, over time this will lead to deformational arthrosis of the knee joint.
- Increased stress on joints. Sports activities should be strictly dosed in terms of lifting weights. Lifting heavy weights, frequent injuries and sprains in the legs is a recipe for deterioration. Often, due to chronic overtraining, an athlete accumulates microtraumas. At first, small injuries are practically not felt, but over time they can develop into fractures and serious damage. Separately, we should consider the moment of starting sports after 40 years. At this age, there is already a slowdown in the natural recovery processes in the body, so dosing loads should be approached more carefully. Movements should be smooth so as not to cause damage. Also, in old age, joints are in worse condition than at a young age.
- Obesity, overweight. There is no direct connection between a person’s body weight and arthrosis, but there is a relationship in terms of the load placed on the joint. Severe obesity, along with a weak muscle corset, contributes to increased pressure on the meniscus, which over time leads to injuries and gonarthrosis. The highest risk is a combination of varicose veins and obesity. In this case, poor blood circulation is observed, so the occurrence of arthrosis in such a situation is associated with the rapid development of articular pathology.
- The presence of weak ligaments and tendons. This phenomenon is more often observed in individuals with a congenital tendency to hypermobility. An example is that a person has good flexibility since childhood; he does the splits without preparation or bends strongly in the lumbar region. Excessively developed flexibility often leads to the development of microtraumas and arthrosis. The situation is often complicated by the fact that a person does not feel pain during microtrauma, and therefore does not notice the appearance of pathology.
- Presence of concomitant diseases. Many other joint pathologies, including autoimmune rheumatological diseases, can provoke the occurrence of arthrosis. For example, a long-term aggressive course of rheumatoid arthritis often leads to arthrosis. Since the inflammatory process in autoimmune diseases is difficult to suppress, and even with constant use of disease-modifying drugs, exacerbations often occur, chronic inflammation leads to arthrosis. Knee and hip joints are often affected.
- Violation of metabolic processes. Various pathological conditions, endocrine disorders and increased bone tissue resorption can lead to problems with the musculoskeletal system, which causes many complications, including arthrosis.
- Stressful conditions. Nervous and physical exhaustion often leads to a weakening of the body’s defenses, which partially affects the development of pathology and can contribute to the occurrence of arthrosis.
Symptoms of deforming arthrosis
Symptoms in the presence of this disease are not specific and in the initial stages may seem vague. If arthrosis is in the first stage of development, then slight pulling sensations or stiffness can be confused with signs of overload. As the pathology progresses with the subsequent growth of osteophytes, the discomfort intensifies. At first, pain is felt only during periods of physical activity, but as the clinical picture worsens, discomfort begins to bother you even during periods of rest.
Symptoms are directly related to the stage of development of the disease. At the initial stage, discomfort rarely occurs. If discomfort occurs, it is associated with fatigue during prolonged walking or running. They are often periodic in nature and immediately subside during the rest period. The crunch occurs rarely and is not accompanied by discomfort. A person can calmly go about his daily activities for years, because arthrosis develops very slowly.
What symptoms occur with arthrosis?
Vivid symptoms that force you to go to the hospital more often appear with the development of stage 2 of deforming arthrosis of the knee joint. The patient begins to feel severe pain, which worsens during periods of exercise and subsides slightly during rest. A characteristic symptom of the disease, in addition to constant crunching, is the occurrence of night or morning stiffness in the area of the affected knee. After waking up, a person needs some time to eliminate the stiffness in the knee, otherwise it will not bend normally. If you do exercise therapy, the stiffness will go away. During exacerbations, the joint may swell and become red. Pain is effectively relieved by the use of NSAIDs.
With further development of the pathology, the pain becomes severe and constant. The patient experiences discomfort even during periods of complete rest. Typically, this condition indicates complete neglect of the disease, which requires urgent treatment to the hospital. If the stage of development of the pathology is late, then the knee stops hurting, but can no longer bend or straighten, since the cartilage has completely worn out, and instead of them a large number of osteophytes have grown, which do not allow normal movement. External signs of deformation are also detected at a late stage of the disease.
Folk remedies
After the main treatment, orthopedists allow the use of folk remedies. They are used to eliminate mild pain and morning stiffness.
Burdock root
Large young burdock root is peeled and crushed. A tablespoon of plant material is placed in a ceramic teapot and poured with a glass of boiling water. After an hour, filter, take 70 ml (about a third of a glass) 3 times a day after meals.
Purslane grass
A tablespoon of fresh purslane herb (stems and leaves) is poured into a glass of hot water and simmered for 10 minutes. Infuse, wrapped, for 2 hours, filter, take 1-2 tablespoons 3-4 times a day after meals.
Herbal collection
Pour a teaspoon of dried calendula and chamomile flowers into a thermos, add a tablespoon of birch buds. Pour in a liter of boiling water and leave for 3 hours. Cool, filter, take 100 ml before bed.
Stages of development of deforming arthrosis
The disease has 3 main degrees of progression:
- In the initial stages, if there is pain, it is insignificant. There may be excessive accumulation of synovial fluid in the joint cavity, which leads to the formation of Baker cysts. Although at this stage active processes of destruction of cartilage tissue are already taking place, such changes are still invisible on x-rays. This stage is often called pre-radiological. To identify arthrosis at the initial stage, you need to use more highly sensitive diagnostic methods - CT or MRI.
- Arthrosis of the knee of the second degree is characterized by the appearance of a narrowing of the joint space, and significant damage to the cartilage tissue is observed. X-ray photographs already clearly show osteophytes - bone growths that replace cartilage tissue. At this stage, the pain already becomes acute, especially when making sudden movements, so motor activity becomes limited. Patients rarely consult a doctor with the initial symptoms of arthrosis, so at stage 2 the disease is already somewhat advanced. In this case, the patient experiences severe discomfort when performing flexion and extension movements in the knee joint. An experienced specialist at this stage can also distinguish the first signs of deformation in the affected joint.
- The third stage of the disease is terminal. X-rays may show signs of complete thinning of the cartilage in some areas, including the ankle joint. Also, at this stage, the X-ray machine perfectly recognizes large growths - osteophytes, which appear in place of worn-out articular cartilage. There is a deposition of salts in the joint cavity, and free elements are detected. External signs of the disease at this stage are very noticeable, there is a characteristic deformation. Pain syndrome becomes a constant companion of a person, and joints almost completely lose their natural mobility.
Treatment tactics for arthrosis are determined individually. It depends on the stage of the disease, the rate of progression of degeneration and the patient’s individual response to treatment.
Diet
Diet for osteoarthritis of the knee joint
- Efficacy: no data
- Timing: constantly
- Cost of products: 1700-1800 rubles. in Week
With normal body weight, a balanced, nutritious diet is recommended, in accordance with age and energy expenditure. A mandatory requirement is the inclusion in the diet of natural chondroprotective products that promote the process of collagenase/hyaluronan synthesis, slow down negative structural changes in joints and normalize the structure of the cartilage tissue matrix. Products with such properties include: hard cheeses, cartilage, gelatin, chicken/pork legs, red fish and chicken meat, from which it is necessary to prepare jellied fish, jellies, fruit and berry jellies/jelly.
When body weight exceeds the norm, dietary nutrition is aimed at normalizing it. This diet is based on a reduced calorie content of the daily diet in the range of 500-600 kcal, on average to the level of 1800-2000 kcal/day, which ensures a gradual reduction in body weight at the level of 0.5-1.0 kg/week. The limit to 250-300 g is primarily limited to simple carbohydrates and refractory animal fats (up to 60 g). At the same time, the protein content remains within the physiological norm. It is recommended to practice 1-2 fasting days/week: fruit and vegetable, cottage cheese, kefir days.
The diet is limited to sugar, sweets, honey, chocolate, pastries, white bread, fatty meats, mayonnaise, fast food, high-calorie dairy products, waterfowl meat (duck/goose), animal/cooking fats, smoked meats. Any fried foods are not recommended.
Diagnosis of deforming arthrosis of the knee joint, degree 2
The basic method for studying arthrosis is radiography. Using this research method, it is possible to determine the stage of advanced pathology by the degree of narrowing of the interarticular space and the number of overgrown osteophytes. To diagnose the pathology of the knee or hip joint at stage 2, x-rays are suitable, since at this stage characteristic pathological changes in the joints are already visible.
At the initial stages of diagnosis, other, more highly sensitive research methods are used, including CT, MRI, ultrasound or arthroscopy. These instrumental diagnostic options are more accurate, but expensive. Ultrasound is an accessible method, but it is not effective for detecting arthrosis in all cases. CT is recommended for early detection of joint degeneration. MRI is best done when there are signs of inflammation. Arthroscopy is the most accurate and expensive way to examine joints, but it is prescribed for advanced cases to identify complex anomalies or is performed before surgery.
If, when identifying signs of arthrosis, inflammation is observed at the site of the lesion, then it is important to differentiate arthritis from internal, autoimmune pathology. In this case, it is necessary to carry out a series of tests to exclude ankylosing spondylitis, rheumatoid arthritis, and psoriatic arthritis.
What tests are usually prescribed to exclude pathological arthritis:
- Antigen HLA-B27.
- Rheumatoid factor.
- ASL-O.
- C-reactive protein and erythrocyte sedimentation rate are nonspecific markers of systemic inflammation.
- Anti MCV.
- A-CCP.
Based on the data obtained, a final diagnosis is made. If some tests go beyond the reference values, it means that the patient has an autoimmune disease that has caused secondary arthrosis over time.
Diagnosis of the disease
Any clinical recommendations for deforming osteoarthritis are prescribed after a thorough examination. Therefore, if you discover its signs, you should see a rheumatologist as soon as possible.
He will prescribe the following diagnostic procedures:
- X-ray diagnostics, thanks to which the degree of narrowing of the joint gap, the size and localization of growths, and features of bone changes will be clearly visible;
- for a more detailed examination - CT and ultrasound of the spine, as well as MRI of the damaged joint;
- puncture of the diseased joint (if necessary);
- endoscopy (arthroscopy) of the damaged knee joint (not mandatory, at the discretion of the specialist).
Treatment of arthrosis 2 degrees
Treatment methods can be divided into 2 types - conservative and radical. Conservative therapy also involves the use of non-drug treatment methods aimed at restoring the functionality of the limb. If the situation is advanced, as with end-stage arthrosis, surgical intervention is prescribed. During surgical treatment, endoprosthetics is performed - this is the replacement of a joint with an artificial implant.
Drug treatment used for grade II arthrosis
Drugs in the treatment of degenerative joint damage can be divided into disease-modifying and symptomatic. Symptomatic treatment is carried out during the period of exacerbation, using short-term medications to eliminate pain and inflammation.
What medications are most effective for exacerbation:
- NSAIDs. Non-steroidal anti-inflammatory drugs have a complex effect, remove inflammation, pain and reduce elevated body temperature. With short-term use, in most cases they do not cause unwanted side effects, so when using them for up to 5-7 days, there are no consequences. If, after the specified time, the exacerbation with the help of NSAIDs is not eliminated, then the treatment tactics need to be changed. Examples of medications are Diclofenac, Airtal, Nimesil, Movalis.
- Corticosteroids. For arthrosis, they are not used systemically, but are prescribed with caution in the form of intra-articular injections to suppress severe inflammation. Often, intra-articular blockades with corticosteroids are not recommended, as they negatively affect the structure of cartilage tissue. Typically, long-acting drugs are used to suppress inflammation for a long time if it is chronic. More often, injections of Diprospan or Kenalog are prescribed. Less commonly, Dexamethasone or Hydrocortisone.
- Muscle relaxants. They do not affect the joint, but relax rigid muscles that tense in response to inflammation, which in turn increases pain in the affected area. It is possible to treat osteoarthritis with the help of muscle relaxants by increasing the effectiveness of NSAIDs, because these medications potentiate the effect on each other. In case of defarthrosis during the period of exacerbation, it is necessary to relax the muscles so that the inflammation does not increase even more. The average duration of taking relaxing drugs is two to three weeks. Examples of products are Baclofen, Mydocalm, Sirdalud.
- Chondroprotectors. With long-term use of these drugs, a therapeutic effect often appears. These medications help relieve pain. Many medical studies confirm the presence of improvements when taking this group of medications, but their use does not lead to quick results. To evaluate the result in terms of reducing discomfort in ligaments and joints, it is necessary to take chondroprotectors for six months or more. These drugs will not help with severe pain, but they effectively support the functions of joints and bones, and improve well-being in the presence of chronic discomfort. An example of substances is Dona, Chondroguard, Teraflex.
- Hyaluronic acid injections. This drug is injected into the joint. Such manipulations are performed in special institutions under close medical supervision. When performing an injection, control is carried out through an ultrasound machine or x-ray so that the needle does not touch the surface of the bones. This medication serves as a synovial fluid replacement that helps temporarily improve range of motion when bending your legs or arms. Such medications are administered 1-2 times a year into each joint.
- Vitamins, minerals. One of the ways to correct the condition of deforming osteoarthritis is to correct the patient’s diet with the help of nutritional supplements. Not all patients can afford a diet that is maximally rich in minerals and varied, so it is necessary to enrich the menu with nutritional supplements. This approach to therapy is based on the fact that when osteophytes grow, calcium is actively consumed from the bones. If the patient has polyarthrosis (more than 3 joints are affected), secondary osteoporosis may occur against the background of ankylosis. To prevent this condition, calcium and cholecalciferol preparations should be prescribed. The duration of the appointment is determined by the doctor based on laboratory tests. Examples - Calcemin Advance, Aquadetrim, Detrimax.
For external use, ointments and gels with NSAIDs and muscle relaxants are prescribed. If there are no signs of inflammation, it is permissible to use warming agents that improve mobility in the joint.
How to treat using non-drug methods
Non-drug therapy is based on the use of physiotherapeutic correction methods, the use of massage techniques and regular exercises that develop joints. It is worth understanding that during the period of active exacerbation these treatment methods are prohibited. Non-drug correction is supportive, effectively helping a patient with osteoarthritis during remission. There are several effective recovery methods to consider.
What physiotherapeutic procedures help fight chronic inflammation:
- Electrophoresis. The method is based on the effect of a weak electric current on the affected tissue. Additionally, NSAIDs, hormones or vitamins are prescribed in the form of injection solutions, but they are not used parenterally, but are applied to the skin, after which the device is connected. In this method, medications enter transdermally and affect the focus of chronic inflammation. As a result, the patient feels better after several sessions. The advantage of the method is quick results without side effects on the entire body. Using electrophoresis, it is possible to remove chronic pain, inflammation and swelling.
- Magnetic therapy. The essence of the method is similar to electrophoresis, but with one difference - medications are administered through the skin using a weak magnetic field. This method also helps relieve chronic inflammation and pain. After several sessions of magnetic therapy, the patient begins to feel much better, stiffness and chronic discomfort disappear.
- Shock wave therapy. Using this method of therapy, it is possible to adjust the rate of development of osteoarthritis, slowing down its progression. Hardware radiation effectively affects the chronic source of inflammation and destroys bone growths - osteophytes. It is recommended to undergo several sessions to experience a significant effect from this procedure.
Massage techniques are also effective. When there are no longer signs of inflammation, it is recommended to gently massage the limb, which will help mechanically relax the rigid muscle tissue. As a result, the muscles become softer and more pliable, which leads to significant improvements in the patient's condition.
How to relieve pain from arthrosis
One of the key points of recovery is exercise therapy. Physical therapy effectively helps to develop a manually constrained joint. It is recommended to select a set of exercises individually with a rehabilitation therapist. After the specialist shows the correct execution of the exercises, and the patient learns to do them independently without mistakes, you can carry out physical education at home. The key to treatment with gymnastics is patience.
To achieve the effect, you need to carry out physical therapy daily, at least once a day. This point is especially relevant for people leading a sedentary lifestyle. Exercise therapy allows you to work out your muscles and helps strengthen them. Strong muscles relieve stress from the affected joint, after which the patient feels better. If the patient does not perform the exercises every day, but from time to time, then such treatment is ineffective.
To avoid exacerbations, it is important to adhere to a gentle lifestyle. The patient must normalize his diet and life schedule. If the patient works in difficult labor conditions, he needs to change his professional activity. It is important to wear orthopedic shoes with anatomical insoles, sleep on a hard mattress and avoid physical inactivity.
Operative method
For grade 2 deforming osteoarthritis of the hip joint, operations are performed quite rarely. Indications include persistent pain and rapid progression of the pathology.
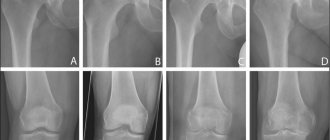
On the right is the head of the femur at stage 3, on the left is healthy.
Arthroplasty is usually used - excision of osteophytes (bone growths), reconstruction of the femur, acetabulum. Endoprosthetics, or replacement of a joint with an artificial implant, is also possible.