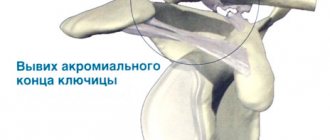
Many users of different ages are interested in how to straighten a shoulder on their own and what is needed for this. It is worth immediately noting that the reduction of dislocations of any type must be performed by a qualified specialist.
As a result of injury, the victim is significantly limited in his usual social life. Ignoring deviations leads to the development of serious complications. Optimization of physical processes in the body will not occur until the problem is eliminated. Pre-medical care plays a huge role.
Types of dislocations
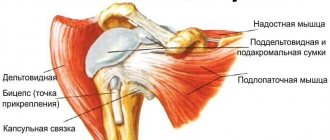
The shoulder joint is the third largest joint in the human skeleton, formed by the scapula and the head of the humerus.
This marvel of nature's engineering gives increased mobility to the most amazing limb on Earth. But precisely because of its mobility, the shoulder is at risk when it comes to dislocations.
Dislocations come in different natures and severity:
- Habitual - a dislocation that recurs periodically due to an anatomical disorder, trauma at birth, or as a result of unskilled reduction of a traumatic dislocation;
- Traumatic dislocation - occurs due to mechanical impact on the joint.
The severity of the injury is determined by:
- Dislocation - when, when the head comes out of the humerus, the ligaments, joint capsule, and often nearby shoulder muscles are damaged;
- Subluxation is a slight separation of the bones of the joint from each other with injury to the ligament system, but without rupture of the soft tissue. The danger of subluxation lies in its apparent safety. Often it can be mistaken simply for a bruise and not seek timely help, which can subsequently negatively affect the health of the joint.
Treatment methods for habitual shoulder dislocation
As a rule, the patient consults a doctor after a long series of dislocations. Often the symptoms are erased or not noticeable. If a person has already undergone treatment, then a complete medical history can be reconstructed from his existing medical record.
Usually the specialist immediately notices:
- muscle atrophy while maintaining the shape of the joint,
- decreased sensitivity,
- restriction in movement due to fear of recurrent pain,
- caution in using your hand.
Only an experienced traumatologist can diagnose the presence of a habitual dislocation. He will examine the patient, collect anamnesis, and conduct the necessary instrumental studies.
To establish the presence of this type of injury, there are usually four main symptoms:
- Weinstein (limited movement in the forearm);
- Babich (muscles are in spasm, which makes passive movements difficult);
- Khitrova (if you pull the upper limb down, a gap appears between the bone and the articular process of the scapula);
- Stepanova (in the lying position the patient is not able to reach the couch on which he lies).
Additional diagnostic methods include radiography, ultrasound, arthroscopy, electromyography, etc. Good results can be achieved using magnetic resonance and computed tomography. They give a clear picture of all the features of bones, muscles, ligaments, as well as the tissues surrounding them. If necessary, arthrography is performed using contrast. It makes it clear which places are most affected as a result of habitual dislocation.
In the presence of this type of injury, therapeutic treatment is usually not effective, so in most cases surgery is recommended.
If the dislocation occurs a small number of times (no more than two), then it is necessary to wear a fixing bandage. To strengthen the joint, massage and therapeutic exercises are performed. The patient is also prescribed analgesics, external anti-inflammatory drugs, diuretics, wound healing agents, chondroprotectors, calcium supplements, etc.
Symptoms
Violation of the shoulder anatomy occurs after a sharp push from an outstretched arm or a strong blow to the back in the joint area. After the characteristic pop with which the bone leaves its place, the victim feels a sharp piercing pain.
Visually diagnosed:
- Deformation;
- Hematomas;
- Depression on the deltoid muscle;
- Immobility of the arm and rapid swelling of the shoulder;
- The injured shoulder is located lower than the healthy one;
- The surface of the palms becomes numb or feels tingling.
About a quarter of dislocations are accompanied by bone fractures. If the blood supply is disrupted, the hand and forearm of the injured arm will become cold and acquire a bluish tint.
Reduction of dislocation according to Chaklin
The patient is positioned in a horizontal position on his back, and the guide stands behind his head. With one hand you need to take the injured person by the hand, and place the other on his shoulder in the area of the head of the joint. After this, you need to begin to carefully move the head of the humerus to the side.
The presented technique is absolutely not suitable for independent use due to the fact that it is too painful. It is practiced by doctors only after the patient has been given anesthesia. The method is most often used in cases where the dislocation resulted in a simple fracture.
Waiting for the doctor
If it is possible to entrust the reduction of a shoulder dislocation to specialists within 12 hours, then there is no need to attempt this complex procedure; it is better to provide first aid to the victim.
To do this you need:
- Secure the arm, bent motionlessly at a right angle, using a bandage. Any available means can serve as a bandage - scarves, belts, clothes, bedding. The forearm and elbow are conveniently located inside the bandage, the ends of which are secured to the neck so that the forearm is at chest level. This will avoid involuntary movements that can cause severe pain; and undesirable consequences in case of nerve rupture, vascular damage or bone fracture;
- Apply cold to the injured area - ice, frozen food or a damp cloth. By constricting blood vessels, cooling prevents inflammatory processes, reduces bleeding and relieves pain. Ice should be crushed for better adhesion to the surface, poured into a plastic bag and wrapped in a soft, dry cloth so as not to cause harm to the skin. Keep the compress on the sprain for 15-20 minutes per hour;
- Unbearable pain caused by injury and muscle spasm can lead to painful shock, so you should offer the victim a painkiller or muscle relaxant. When choosing a medicine, you should take into account the nature of the injury. In case of open or internal bleeding, determined by bruising and hematomas, Naproxen and Ibuprofen should be discontinued. These drugs provide good pain relief, but thin the blood, increasing bleeding. You should also not mix several medications without knowing their compatibility.
If the circumstances are such that “the rescue of drowning people is the work of the drowning people themselves” and there is nowhere to wait for help, it is not at all out of place to know how to set a shoulder yourself. But such knowledge should be used only in the most emergency situations.
Treatment
At the beginning of the treatment course, it is necessary to decide on the method of repositioning the injured joint. Reposition is carried out under local anesthesia; for this, the patient is injected with pantopon or morphine, after which novocaine is used, which anesthetizes the shoulder joint. Reduction of dislocations can be carried out by a large number of different methods.
The most commonly used methods for reducing a dislocated shoulder are:
- Reduction of shoulder dislocation according to Kocher;
- Reduction of shoulder dislocation according to Dzhanelidze;
- The Hippocrates-Cooper method.
Methods for self-reduction of the shoulder joint
Before you start realigning the joint, you need to numb it well and cool it down, otherwise you risk losing consciousness before completing the procedure.
Circular rotation
Do it while sitting or standing.
- Raise your arm bent at the elbow joint to chest level;
- Without straightening, move it to the side as far as possible;
- From this position, lift up so that your palm is above your head.
Movements should be smooth and non-stop.
Using your knee
- Sit on a horizontal platform;
- Bend your knees and press them to your body;
- Interlace your fingers and place them behind your knees;
- Slowly leaning back and straightening your knees, try to pull the head of the joint into place.
Either an epic hero or a person placed in a hopeless situation can perform such a manipulation. Much more often there are other people around the incident and the opportunity to receive or provide all possible assistance.
The main thing is that this help is competent enough and does not cause even more harm.
Hippocrates-Cooper method
The essence of the action is as follows: the patient takes a horizontal position, the specialist sits near the injured limb. Then, firmly grasping the sore arm and resting his foot on the patient’s axillary area, he begins a gradual stretching. Minor rotations along the axis are permissible for adhesion to the joint.
Reduction of the shoulder joint with an assistant
When you are providing assistance to someone and are not sure of the correctness of your actions, you should contact an emergency service employee by phone to clarify the algorithm of actions. Be sure to obtain the consent of the person you are going to help, warning him that you are not a medical professional and cannot be held responsible for unqualified actions.
If you need help, you should try to persuade the person nearby to help. There are not so many people who have ever set someone’s hand and, most likely, this proposal will not arouse much enthusiasm. We need to calm the person down, take full responsibility and lead the process.
The victim should be laid on his back, his foot resting against the armpit of the injured arm, and the arm itself should be gradually pulled towards you with increasing effort. Holding the scapula with your foot and extending your arm at an angle of 60-90 degrees, you should feel how the head of the humerus, rounding the scapula, rises to its natural position.
After the shoulder is set, you need to feel the pulse on the injured arm and compare it with the pulse of the healthy arm. Slowness or complete absence of the pulse indicates a violation of blood flow, which without urgent medical attention can lead to the loss of a limb.
If the procedure is successful, a bandage must be applied to fix the unstable joint and transport the patient to the nearest medical facility. In case of failure, the same. You just need to get to the hospital even faster, before hardening of the soft tissues leads to mandatory surgery.
The doctor, after taking an x-ray to make sure there are no fractures, will perform a closed reduction of the shoulder joint. In this case, strong relaxants and anesthetics will be used, up to general anesthesia if necessary.
For those who suffer from a habitual form of dislocation, open surgery is recommended to restore proper functionality of the joint. Such an operation will allow us to identify and eliminate the internal causes of regular dislocations in order to get rid of them forever and experience a new quality of life.
Dzhanelidze method
I give the patient an intramuscular injection of an anesthetic drug. The victim is placed on the table so that the limb hangs down and the edge of the table rests on the axillary area. Next, the traumatologist acts on the forearm and simultaneously performs a full rotation of the affected arm around its axis. Thus, the hand independently comes to the correct position. Reduction does not take much time, and the patient recovers faster.
Restoring a joint after a dislocation
Successful return of the joint to its original place is not the end, but only the beginning of long-term rehabilitation, which can take from three months to six months. After 2-4 weeks of drug therapy, the patient is prescribed:
- Physiotherapy,
- Massages,
- Therapeutic gymnastics,
- Swimming and other procedures,
Promoting a speedy recovery, as well as aimed at the overall development and strengthening of the anatomy of the joint to avoid relapses in the future. Statistics show that after a traumatic dislocation of the shoulder joint, the risk of developing a habitual dislocation increases significantly, so it is necessary to conscientiously follow all medical recommendations.
The recovery process is regulated by the doctor based on the individual condition of the patient. Basically, the reduced and treated shoulder is completely restored, allowing normal movement of the arm.
Therapeutic measures and rehabilitation
After the joint is set, the patient’s limb is fixed with a splint, which needs to be worn for about one and a half months. At the same time, the patient is prescribed anti-inflammatory drugs that relieve swelling, pain, and also resolve the hematoma.
Before removing the plaster, a control x-ray is taken. After making sure that the joint is normal, the doctor removes the plaster and prescribes rehabilitation procedures for the patient. These include:
- physiotherapy;
- massage;
- physiotherapy;
- hydrotherapy;
- electrical stimulation, etc.
When a patient is discharged for outpatient treatment, the doctor gives recommendations, following which you can quickly return motor functionality to the limbs.
conclusions
- Never try to correct a dislocated shoulder yourself unless it is due to emergency circumstances;
- If the situation forces you to make such a decision, perform the procedure as quickly as possible in the first 5-15 minutes after the injury;
- When you are afraid of the consequences, think about what will happen if the dislocation is not corrected. By comparing the risks, it is easier to choose a less dangerous option.
The worst case scenario is when alcohol as a painkiller was taken not by the victim, but by the person providing assistance, and after the procedure no one went to the doctors.
General information
Before adjusting a dislocated shoulder, you need to become familiar with its anatomical features and causes of injury. Provoking factors are often:
- strikes at a specific point;
- falling from a certain height;
- industrial cases;
- uncontrollable seizures;
- pathological abnormalities (arthrosis, tuberculosis);
- car accidents.
Relatively, locations are divided into: anterior (frontal), posterior (dorsal) and medial.