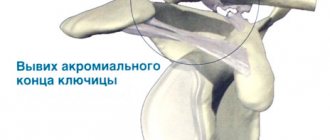
Collarbone - This is a curved S-shaped bone, consisting of a body and having two ends with articular surfaces - acromial (external) and sternum (internal). Together with the scapula, it forms the girdle of the upper limbs. The clavicle is the only bone that connects the trunk (axial skeleton) to the upper limb. Due to the fact that the clavicle is involved in the formation of two joints (sternoclavicular and acromioclavicular), dislocations occur in two types: the sternal end of the clavicle and the acromial end of the clavicle. Dislocations of the acromial end most often occur; dislocations of the sternal end of the clavicle are much less common. Dislocation of the scapular (acromial) end can be complete or incomplete (depending on which ligament is torn). Dislocation of the sternal end is divided into suprasternal, presternal and retrosternal (depending on the trajectory of the clavicle displacement).
Clavicle dislocation
- Anatomy of the clavicle
- Classification
- Dislocation of the outer (acromial) end of the clavicle
- Dislocation of the internal (sternal) end of the clavicle
- Symptoms of types of dislocations
- Prosternal type of dislocation
- Suprasternal type of dislocation
- Substernal type of dislocation
- Photo of a dislocated collarbone
- First aid for acromial dislocation
- Treatment of clavicle dislocations
- Conservative treatment
- Surgery
- Rehabilitation
Content
Anatomy of the clavicle
The clavicle is a not very large arcuate tubular bone. It is united on one side with the sternum, and on the other with the acromial end of the scapula. The main injuries to this area are a fracture or dislocation of the collarbone.
Since it contains 2 ends, in this case, dislocation of the acromial end of the clavicle is also distinguished as dislocation of the sternal end of the clavicle. Injuries to the acromial end are more common. We will analyze all the symptoms and causes of injury, without exception, as well as all possible ways to solve the problem.
A dislocated collarbone is a fairly common injury. As a percentage, the number of cases of clavicle dislocation is 5% of the total number of injuries of this kind. In this case, one should strictly distinguish between dislocation of the acromial (external) and sternal (internal) ends.
For a general understanding of the collarbone, we invite you to watch a video that describes in detail the composition of the shoulder joint.
Classification
If up to 3 days have passed since the dislocation of the sternal or acromial end of the clavicle, such a dislocation is considered fresh, from 3 days to 3 weeks - stale, more than 3-4 weeks - old.
Depending on the location and degree of damage in traumatology and orthopedics, the following are distinguished:
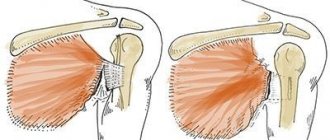
- Complete dislocation of the acromial end of the clavicle - damage to the coracoclavicular ligament, capsule and ligaments of the acromioclavicular joint.
- Incomplete dislocation in the acromioclavicular joint - the acromioclavicular ligament is torn, the coracoclavicular ligament remains intact.
- Complete dislocation of the sternal end of the clavicle - the integrity of the sternoclavicular and costoclavicular ligaments is disrupted.
- Incomplete dislocation of the sternoclavicular joint - the sternoclavicular ligaments are damaged, the costoclavicular ligament remains intact.
Dislocation of the outer (acromial) end of the clavicle
The outer, acromial end of the clavicle is connected to the acromial process of the scapula by two ligaments. Depending on whether one or both of them is damaged, subluxation or complete dislocation of the clavicle is diagnosed, respectively.
Symptoms of external dislocation of the end of the clavicle
The main symptoms of a dislocation of the outer end of the clavicle are:
- pain in the area of the junction of the collarbone and scapula.
- pain when trying to move your arm or shoulder.
Important!
It is worth noting that the latter aspect often leads to the fact that, out of ignorance, patients often confuse a dislocated clavicle with a dislocated shoulder joint.
However, distinguishing one injury from another is quite simple, knowing the following symptoms:
- When the clavicle is dislocated, there is swelling and deformation caused by the protrusion of the outer end of the bone (it protrudes upward and slightly back). Swelling rarely occurs in cases of shoulder dislocation.
- A dislocation of the shoulder joint is accompanied by a feeling that the shoulder is out of place, and any attempt to move the limb is accompanied by a sharp attack of pain. If the collarbone is dislocated, the pain is moderately limiting.
Causes
Articulation rupture can occur in the following cases:
- Injury during sports activities, for example, among goalkeepers of hockey or football teams, who often fall on their shoulder while catching the ball or trying to hit the puck.
- Injury in contact sports, for example, sumo, judo, boxing and others.
- Falling on an outstretched upper limb, for example, during icy conditions.
- An overly active lifestyle that leads to falls, for example, roller skating, skiing, and so on.
Dislocation of the internal (sternal) end of the clavicle
Unlike the external one, dislocation of the internal, sternal end of the clavicle is quite difficult to confuse with anything else. This is explained by the specific articulation of the bone with the chest.
Depending on the nature of the injury, there are different types of dislocations:
- Prosternal
- Suprasternal
- Retrosternal
All of them are characterized by pain in the area where the collarbone connects to the sternum:
- Pain when breathing deeply
- Deformation and swelling of soft tissues
- Noticeable shortening of the shoulder girdle on the injured side
Important!
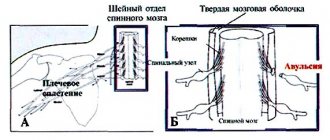
If the dislocated bone touches the vessels, which is most often observed with a retrosternal dislocation, specific external manifestations will be noted (for example, a change in the color of the skin).
Arthrosis
Arthrosis of the acromioclavicular joint is diagnosed less frequently than shoulder arthrosis. The causes of the pathology are:
- Frequent loads on the shoulder - professional activities, sports.
- Injuries.
- Inflammatory processes in the joint cavity and in soft periarticular tissues.
- Physiological reasons – aging of the body.
- Endocrine disorders.
- Deterioration of joint nutrition, stagnation, slowdown of metabolic processes, circulatory disorders.
When articular cartilage is destroyed, the following processes develop:
- Compaction of subchondral bone tissue.
- The appearance of microcavities that merge with each other, resulting in the formation of bone growths - osteophytes.
- Dead cartilage fragments and osteophytes, irritating the synovial membrane, provoke an inflammatory process, that is, synovitis occurs.
- The joint becomes deformed and its edges can protrude significantly through the skin.
Symptoms of types of dislocations
At the same time, there are symptoms characteristic of each individual type of dislocation.
Prosternal type of dislocation
Thus, the first, prosternal type of dislocation is the most common and is easily determined by the protrusion of the inner end of the clavicle forward.
Suprasternal type of dislocation
In the case of a suprasternal dislocation, the collarbone protrudes forward and upward.
Substernal type of dislocation
For the third type of dislocation, according to its name, there is a retraction of the inner end of the clavicle. Retrosternal dislocation of the inner end of the clavicle is considered to be the most dangerous, since in this case there is a serious risk of damage to important anatomical structures.
Also helping to avoid confusion is the fact that in the event of a fracture, in addition to swelling and deformation, there is limited mobility of the shoulder, bruising and rupture of soft tissues from fragments of the broken bone. In addition, displacement during a fracture, unlike a dislocation, usually occurs forward and downward. However, an x-ray should be taken to rule out the presence of a bone fracture.
Attention!
In people who are obese, the outward signs of a dislocated collarbone may be less noticeable.
Osteolysis
Osteolysis of the acromial end of the clavicle is a rare pathology that is accompanied by resorption of bone tissue. For what reasons this phenomenon occurs, scientists have not yet figured out. Only the connection between the pathology and autoimmunization of bone tissue is known. This disease is characterized by the absence of pain symptoms. The clinical manifestation of the disease is poor healing of bones during fractures. As for radiography, osteoporosis is noticeable in the pictures - loss of bone tissue.
First aid for acromial dislocation
When providing first aid to a victim who has suffered a dislocation of the collarbone, first of all, one should ensure fixation and calmness of the injured limb. This can be done using a bandage or a rag scarf. The arm is suspended in a bent state, and a small soft cushion is placed in the armpit.
Since the injury is very painful, it is permissible to apply a cold compress to the painful area. Ice should be wrapped in cloth to prevent the skin from freezing. This kind of compress can be applied for no more than a quarter of an hour with an interval of thirty minutes between procedures.
It is important to know!
Attempting to straighten a dislocation on your own is strictly prohibited, since inexperienced actions can lead to negative consequences. Also, until the ambulance arrives, you should not give the patient strong painkillers, which can change the clinical picture.
Treatment of clavicle dislocations
Therapy for clavicle dislocation is carried out both by conservative methods and by surgical intervention.
Conservative treatment
The specificity of the procedure is that straightening the protruding end of the collarbone is not a difficult task. It is much more difficult to fix and keep it in the correct position. In traumatology, incomplete acromial dislocation is usually treated conservatively. The displacement of the bone is eliminated by moving the shoulder back and at the same time pressing on the protruding end of the clavicle. Then the acromioclavicular joint is immobilized for a period of 2-3 weeks. Subsequently, physical therapy and physiotherapy are prescribed: electrophoresis, magnetic therapy, ozokerite therapy.
When the sternal end is dislocated, reduction is carried out without much difficulty, but it is not always possible to keep the collarbone in place. The assistant pulls the patient's shoulders back, while the traumatologist corrects the position of the collarbone by moving it out from behind the sternum or applying pressure. There is a special conservative treatment method in which, after reduction, a figure-of-eight plaster cast is applied. The patient is prescribed exercise therapy and physiotherapy.
Treatment for dislocation of the outer end of the clavicle is carried out using invasive and non-invasive techniques. In most cases, one of the conservative treatment options is sufficient. But if at the end of treatment there is no result, or it is unsatisfactory, the doctor may suggest surgical intervention.
Surgery
With complete acromial dislocations, articulation plastic surgery is often indicated, since the unrestrained acromial end of the clavicle is very easy to put in place, but due to the anatomical structure of this area, it is almost impossible to keep it in the correct position. During the operation, the orthopedic traumatologist realigns the collarbone and secures it with Mylar tape or silk thread. Some surgical techniques use additional fixation with a pin.
For fresh substernal dislocations of the clavicle, in most cases surgical treatment methods are also used. Lavsanoplasty is used to restore ligaments. Usually the operation is performed as planned a few days after treatment. In case of retrosternal injuries, especially those accompanied by breathing problems, intervention is performed on an emergency basis. Old dislocations of both ends of the clavicle can only be eliminated with the help of surgery, the indications for which can be considered as pain and movement disorders, as well as a cosmetic defect.
Fracture
Fracture of the acromial end of the clavicle is often observed in children, active young people and athletes. The main reason is a fall on the shoulder joint or an outstretched arm. With a direct shoulder impact, fractures are observed much less frequently.
A broken collarbone has the following clinical picture:
- The person automatically supports the upper limb.
- The shoulder is displaced downward and forward.
- Severe pain that prevents you from raising your arm.
- Swelling.
- Hemorrhage.
- Crunching when trying to raise your arm.
It must be said that a visual examination alone cannot provide accurate information about the damage, so the patient is sent for an x-ray. An x-ray may show an acromial fracture of the clavicle, a classic fracture, or a displaced fracture. All this influences the choice of therapy.
Treatment again can be of two types. The conservative method consists of eliminating the displacement (if any) and immobilizing the joint until the bone has completely healed. Often this treatment option does not lead to a positive effect - the shoulder girdle can become shortened and deformed. In addition, a long period of healing of a broken collarbone significantly worsens the patient’s quality of life. In this case, it is preferable to perform surgical intervention - osteosynthesis. The essence of the operation is the elimination of debris and fixation of the bone with a metal plate. Sometimes the plate is removed after a few months, but most often it is left in place for life.
Rehabilitation
Regardless of what methods were used in the treatment of clavicle dislocation, rehabilitation is an important and necessary link in therapy. With its help, the healing process of muscles and ligaments is accelerated, the motor activity of the limb is restored, the collarbone is strengthened, which serves to prevent relapses.
After 3 months after the injury, the doctor prescribes special physical exercises, with the help of which the collarbone and arm acquire their previous shape and function. If you start doing exercises ahead of schedule, there is a possibility of recurrence of the injury, the treatment of which will take more effort and time.
Clinical picture
The main problem with shoulder subluxation is instability of the glenohumeral joint. The anatomy of this joint allows for a large range of motion, which is accompanied by a loss of stability. A study conducted by Basmajian determined that the supraspinatus muscle and also the posterior fibers of the deltoid muscle play a key role in preventing humeral subluxation. Chaco and Wolf also confirmed in their study that the supraspinatus muscle is very important in preventing inferior subluxation of the humerus. Shoulder subluxation occurs during abduction and external rotation.
Other studies indicate that the most important ligamentous structure for maintaining proper alignment of the humerus and also for preventing shoulder subluxation is the inferior glenohumeral ligament. This ligament is most important in external rotation and abduction during the throwing movement.
Shoulder subluxation can lead to soft tissue damage because traction can occur due to gravitational forces and a weak shoulder provides poor protection. This is usually quite painful and may be accompanied by partial numbness in the shoulder, arm and hand.