The clavicle is a supporting support for the shoulder girdle, ensuring the function of the upper limb and its position. It is vulnerable to damage because it performs a special function, is located under the skin and has an unusual geometry.
Clavicle fractures are the most common injury among adults and account for 5% of the total number of fractures. The incidence is 29 cases per year per 100,000 population with a mean age of 33 years and a male to female ratio of 2.6:1. In men, the peak occurs between the ages of 13 and 20 years.
The main mechanism of injury is a fall during sports.
Fractures of the middle third of the clavicle are the most common and occur in 69-81% of cases, while injuries to the distal third occur in 16-28%.
Clinical examination
The evaluation of patients should take into account the mechanism of injury and possible associated injuries. When assessing a patient with high-energy trauma, the ATLS protocol should be followed. In case of open fractures, fractures of the middle third, concomitant fractures of the scapula, it is necessary to use additional imaging methods to exclude concomitant damage to the chest organs.
Patient complaints
The main complaint of patients with all clavicle fractures is pain in the shoulder joint , however, to obtain a complete picture it is necessary to examine the cervical spine, chest and evaluate the neurological status to exclude possible combined injuries.
Clinical examination
The examination should begin with an examination of the shoulder areas on both sides. A displaced fracture is characterized by the presence of a typical deformity with protrusion of the medial fragment as a result of the action of the weight of the limb and traction of the sternocleidomastoid muscle.
Shortening of a broken clavicle is manifested by a decrease in the width of the shoulder girdle as a result of protraction of the scapula. During examination, it is necessary to evaluate the condition of the skin, since in case of open fractures or significant skin tension, surgical treatment is indicated. With a direct fall on the shoulder, there are abrasions, which are often located in the projection of the deltoid muscle and acromion process.
Palpation should examine the sternoclavicular joint, subcutaneous surface of the clavicle, acromioclavicular joint, acromial process and spine of the scapula. Detection of specific areas of tenderness determines the need for imaging techniques.
Due to the pain syndrome, there is a restriction of movement, however, with an isolated fracture of the clavicle, passive internal and external rotation is possible. The presence of full passive rotational movements indicates the absence of dislocation in the shoulder joint. The proximity of the brachial plexus and the vessels of the subclavian region requires an assessment of the neurovascular status (examination of the pulse and sensory-motor characteristics of the limb distal to the site of injury).
Visualization
Minimal x-ray examination
should include a direct view with full coverage of the clavicle and acromioclavicular joint. Additional radiography with a radiator tilted 20° radially helps assess clavicle displacement and shortening.
If damage to the shoulder joint is suspected, radiography should be performed in direct and axial projection.
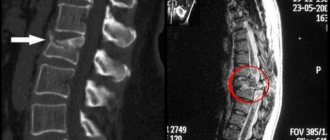
Performing a CT
with reconstruction gives a complete picture of the configuration of the fracture, displacement and shortening
of the clavicle .
Classification
There are several classifications of clavicle fractures . A more practical and constructive classification was proposed by Robinson. This Edinburgh system considers the displacement and comminuted nature of fractures as key features of therapeutic and prognostic significance, as well as inter-rater reliability.
Type I – Medial 1/5 (fracture medial to the first rib)
- IA: no offset
- IA1: extra-articular
- IA2: intra-articular
- IB: offset
- IV1: extra-articular
- IV2: intra-articular
Type II – Moderate 3/5 (Damage to the central 3/5 of the clavicle)
- IIA: without disruption of the cortical layer
- IIA1: no offset
- IIA2: angulation
- IIB: with offset
- IIВ1: simple
- IIВ2: splintered/segmented
Type III – Lateral 1/3 (Injury to the lateral part of the clavicle)
- IIIA: without disruption of the cortical layer
- IIIA1: extra-articular
- IIIA2: intra-articular
- IIIB: offset
- IIIВ1: extra-articular
- IIIB2: intra-articular
All types are further subdivided depending on the displacement, where subtype A is fractures with a displacement of less than 100%, subtype B is more than 100%. Groups are also distinguished depending on the splintered nature of the damage and the relationship of the fracture line to the structure of the joints.
Displaced clavicle fracture
The cause of a clavicle fracture is the excess of mechanical force over the strength of the bone. This can happen to people with epilepsy. If their bones are weakened and the convulsive muscle contractions during an attack are very strong, then a fracture occurs. But most often such serious damage is caused by injury. Injuries are inevitable when playing contact sports: football, hockey, boxing and others, as well as cycling and motorsports. There are many victims after a traffic accident. Newborns can also be injured when passing through the birth canal.
Types of clavicular fractures: outer, middle and inner third of the clavicle. The thinnest and most curved part of this bone is the middle. That is why midline fractures make up the lion's share of the total number of clavicle injuries.
There are many classifications of fractures. They differ in the main characteristics taken as a basis. According to one of them, fractures may be accompanied by displacement of fragments or not. Parts of the collarbone move without separation or in width, length, or at an angle. Displacement always complicates the treatment process and can have unpleasant consequences.
Symptoms of a displaced clavicle fracture:
- shoulder pain;
- swelling;
- cyanosis or pallor of the skin;
- bleeding (external and internal);
- deformation of the contours of the shoulder (lowered and protruding forward, the injured arm “sags”, seems longer);
- the hand does not obey well, the fingers are inactive;
- nerve damage;
- numbness of the hand;
- bone fragments overlap each other;
- “sagging” of the scapula, it protrudes more;
- violation of the integrity of the pleural dome in closed fractures.
The site of injury quickly swells because... The bone fragments are quite sharp and easily rupture adjacent blood vessels. This is the reason for the appearance of hematomas. Displacement of fragments increases pain.
The patient holds the forearm and elbow of the injured limb with his healthy hand and presses it to the body. The hand moves with difficulty, because The collarbone is the support for the bones of the upper limb. Movement in the shoulder joint is limited due to pain. When palpating the fracture site, pathological mobility and crepitus of the fragments can be determined.
There are complete or classic (with a rupture of the periosteum at the site of injury) and incomplete fractures. The displacement can be of several degrees:
- complete, in which the fragments are not held by the periosteum;
- incomplete - the bone structures are displaced, but continue to be held by the periosteum.
In case of a displaced fracture, only a rigid bandage is applied. More elastic tires are contraindicated. Before the procedure of applying a plaster, the patient must be given an anesthetic, because the sore shoulder must be fixed in the correct position. Without anesthesia, the muscles are “protected”; involuntarily, reflexively, they retract – contract.
A displaced clavicle fracture is more difficult to cure, but there are cases when it is accompanied by dislocation and damage to nearby bones. The process of treating an open fracture will also be complex and difficult. Displacement usually requires surgery. Fragments that have shifted into an unnatural position pose a threat to the adjacent neurovascular bundles and skin.
Kinds
Clavicle fractures are divided into:
- simple;
As a result of pain, the patient unconsciously tilts the body towards the fracture (along with the body, the head also tilts). The shoulder blade leans back. In most cases, such damage is accompanied by displacement of fragments. From a scientific point of view, this is explained by the shape of the collarbone, which, with the help of muscles, ensures the connection of the ends of the broken parts and attaches them to each other.The main diagnostic method is a hardware examination, which is a regular x-ray in one projection (direct shot). In situations where it is not possible to detect all the debris, an additional CT scan (computed tomography) is performed.
Clavicle fracture in children
Fractures without displacement of fragments are typical for children. With proper treatment, they grow together in 8-10 days. Approximately 1-2 weeks after the fracture, children can already freely raise their arm.
In babies, the collarbone usually breaks in a greenstick fashion. This is a so-called incomplete fracture, when a complete rupture of the bone does not occur, because The “fragments” are still held together by the periosteum or periosteum. So, in nature it is very difficult to quickly break a young twig. It is so filled with juice, and its bark is so strong and elastic, that it is impossible to do it right away without cutting tools.
The periosteum is a film of connective tissue covering the bone. Thanks to its ability to regenerate, thickening of the bones occurs, as well as the formation of callus at the site of fractures. The nutrient openings of the periosteum supply the bone with blood, and it is to it that tendons and ligaments are attached. The strength of the periosteum in children prevents the displacement of parts of the collarbone, and, therefore, helps reduce pain.
Causes of clavicle fracture:
- falling onto a shoulder or arm from a height;
- strong mechanical impact on the clavicular area, for example, a blow during a fight or in a car accident;
- birth injury;
- muscle cramps (for example, in epileptics);
- Osteosarcoma is a malignant bone tumor.
Skeletal injuries during childbirth are not uncommon. They relate to mechanical forms of birth injuries. In newborns, a clavicle fracture is caused by injuries during childbirth. In early childhood, the cause may be an unfortunate fall while playing, playing sports, or riding a bicycle or skating. Most often, fractures occur in children and the elderly. In children, the bones are not yet strong enough, and in older people they are fragile due to calcium deficiency.
Symptoms of types of dislocations
At the same time, there are symptoms characteristic of each individual type of dislocation.
Prosternal type of dislocation
Thus, the first, prosternal type of dislocation is the most common and is easily determined by the protrusion of the inner end of the clavicle forward.
Suprasternal type of dislocation
In the case of a suprasternal dislocation, the collarbone protrudes forward and upward.
Substernal type of dislocation
For the third type of dislocation, according to its name, there is a retraction of the inner end of the clavicle. Retrosternal dislocation of the inner end of the clavicle is considered to be the most dangerous, since in this case there is a serious risk of damage to important anatomical structures.
Also helping to avoid confusion is the fact that in the event of a fracture, in addition to swelling and deformation, there is limited mobility of the shoulder, bruising and rupture of soft tissues from fragments of the broken bone. In addition, displacement during a fracture, unlike a dislocation, usually occurs forward and downward. However, an x-ray should be taken to rule out the presence of a bone fracture.
Attention!
In people who are obese, the outward signs of a dislocated collarbone may be less noticeable.
Consequences of a clavicle fracture
The consequences may be as follows:
- loss of hand functionality during the rehabilitation period;
- damage by sharp bone fragments to nearby vessels and nerves, as well as the dome of the pleura and skin;
- serious blood loss;
- plexitis - inflammation of the nerve plexuses;
- muscle paralysis;
- secondary displacements, for example, due to muscle contractions or incorrectly applied bandages;
- formation of false joints;
- scoliosis - lateral curvature of the spinal column - with improper fusion of fragments of the clavicle;
- nonunion;
- infection if the area around the wound with an open fracture is not treated with antiseptics;
- osteomyelitis - purulent-necrotic inflammation of the bone and adjacent soft tissues caused by pathogenic microorganisms;
- suppuration of a postoperative wound;
- arthrosis, accompanied by joint stiffness;
- limitation of hand movements;
- cosmetic defect due to improper bone fusion.
A complication in the form of flaccid muscle paralysis occurs with obstetric trauma. This happens with very large newborns and with foot presentation. If secondary displacement is left unattended, the bones will heal crookedly. This will certainly subsequently affect the ability to control the hand and its strength. In addition, when displaced, nerve endings are affected, which causes pain.
Causes of clavicle nonunion:
- comminuted fracture;
- inadequate metal fixation;
- excessive separation of the periosteum during surgery.
In case of nonunion or malunion of the clavicle, repositioning of the fragments and surgery is possible. To identify complications in adjacent soft tissues, in rare cases, computer or magnetic resonance imaging studies are prescribed.
Complications after a clavicle fracture are extremely rare. The severity of possible consequences is determined by the severity of the disease and the level of treatment.
Rehabilitation
Regardless of what methods were used in the treatment of clavicle dislocation, rehabilitation is an important and necessary link in therapy. With its help, the healing process of muscles and ligaments is accelerated, the motor activity of the limb is restored, the collarbone is strengthened, which serves to prevent relapses.
After 3 months after the injury, the doctor prescribes special physical exercises, with the help of which the collarbone and arm acquire their previous shape and function. If you start doing exercises ahead of schedule, there is a possibility of recurrence of the injury, the treatment of which will take more effort and time.
First aid for a broken collarbone
If a clavicle fracture is suspected, the limb should be immobilized as soon as possible to prevent possible movement of bone fragments. Pre-hospital stage, i.e. transportation of the patient must be carried out competently. A set of first aid measures will help to avoid complications: damage to veins, lungs and/or nerves. Unprofessional intervention can irreversibly worsen the situation.
To alleviate the patient's condition, analgesics are administered orally or intramuscularly. A small cushion is placed under the armpit. The arm is bent at the elbow and tied to the body from the shoulder to the hand. The forearm should be parallel to the floor. The brush is threaded into a bandage attached to the neck.
If there is no material suitable for a neck band at hand, then the edge of the clothing is folded up and secured: T-shirts, shirts. It is important that the forearm is completely secured with the bandage. This is the part of the arm from the elbow to the wrist. This type of bandage is called a scarf or headscarf. If the tape is not wide enough, the hand will be too mobile. This can lead to displacement of the fragments.
Why is complete immobilization of an arm with a broken collarbone necessary? When it is completely immobilized, the patient relaxes the muscles, the bone fragments put less pressure on the nerves and the pain subsides a little.
If you only have a scarf, a belt, or just a cloth tourniquet at hand, proceed as follows. It is thrown over the shoulders, and the resulting loops are connected with something between the shoulder blades. It is important that your shoulders are pulled back. In essence, you get soft Delbe ring straps. The main requirements for the design are rigidity and reliability. The fracture site can be numbed by applying ice.
It is forbidden:
- trying to straighten a “dislocation” on your own without an accurate diagnosis;
- transport the patient standing or lying down, only sitting or semi-sitting;
- lean forward;
- pull him by the arms;
- fully straighten the injured limb;
- secure the upper limb with a cord, rope or belt that is too thin.
During transportation, it is better for the patient to lean back a little, this will prevent the fragments from moving. Knowledge of a first aid course can be useful to anyone in life. Ideally, everyone should have the basic necessary knowledge and a set of emergency medical measures.
Physiotherapy
Any rehabilitation is impossible without physiotherapeutic procedures. In addition to therapeutic exercises, patients may be prescribed:
Treatment of a clavicle fracture
The success of the therapeutic course depends on many factors: the severity of the pathology, the extent of damage, the professionalism of doctors and the age of the patient. In severe cases, surgery is required.
X-rays help diagnose a fracture. It is usually carried out in two projections: lateral and direct. The first is necessary to clarify the position of the fragments relative to each other. The traumatologist chooses conservative or surgical treatment depending on the specific case. It is possible to compare bone fragments without surgery using reposition. This is a medical procedure performed under local anesthesia. This procedure avoids improper fusion of parts of the clavicle bone.
After hospitalization, the arm is immobilized for 3-8 weeks. To do this, the patient is given a special fixing bandage. The pain is relieved by a course of analgesics.
The therapeutic course includes:
- anesthetics;
- antibiotics for infection of an open fracture or postoperative sutures;
- general strengthening, immunostimulating agents;
- vitamins;
- calcium preparations to strengthen bone tissue;
- physiotherapy: electrophoresis, magnetotherapy, ultrasound, laser therapy, UHF therapy (ultra high frequency);
- physical therapy, massage and warm salt baths at the final stage of treatment.
Children are usually not given a plaster cast, but are treated only with Delbe rings or a Deso bandage. Among folk remedies, we can recommend comfrey. This plant was actively used in ancient times to treat wounds and fractures. Comfrey has a very powerful healing effect. It is better to purchase ointments and balms based on it in pharmacies, because this forest grass is poisonous. There you can also buy goldenrod herb (common goldenrod), which has very useful properties for treating fractures.
You can take advantage of the anti-inflammatory and pain-relieving properties of ivy bud (catnip). This plant should also be used with caution.
It is advisable to eat foods rich in calcium:
- nuts;
- sesame;
- rose hip;
- milk;
- soy;
- fish;
- bread;
- bran;
- cottage cheese;
- greenery;
- persimmon;
- beans;
- cabbage
It’s easy to prepare your own vitamin mixture from honey, walnuts, two lemons and a glass of dried apricots and raisins. Dried fruits are pre-soaked in boiling water. The lemons are squeezed out and the seeds are removed. Everything is minced with a meat grinder or crushed with a powerful blender and mixed with honey. Take this vitamin mixture one teaspoon three times a day after meals. This is an unusually useful composition; it is good to use both during periods of epidemics of acute respiratory viral infection and during pregnancy.
So, the main method of treating a clavicle fracture is fixation. After healing of the damaged bone, a rehabilitation period is necessary. In addition to a set of physical therapy exercises, the attending physician recommends swimming, warm baths with sea salt and massage.
Applying a bandage for a clavicle fracture
Bandages for matching and holding fragments of a broken collarbone vary in the degree of fixation. The toughest is the classic plaster cast, which is applied over the shoulder and chest. This bandage reliably protects against displacement of fragments, allowing you to monitor the fracture area. Shoulder fixation with plaster is contraindicated for people over 50 years of age, because then a complication develops in the form of arthrosis. Manipulations with a sore collarbone are very painful, so local anesthesia is required.
Conservative treatment involves applying one of the following types of dressings:
- eight-shaped with fixation of the shoulder girdle - such as Delbe, Borchgeriving, Ombredan and others;
- according to Smirnov-Weinstein;
- according to Kaplan;
- according to Voronkevich;
- Deso;
- Seira;
- Titova oval;
- two Kramer tires;
- on a wedge-shaped pillow;
- Chizhin frames;
- Kuzminsky tires.
The technique for applying these dressings is basically the same. The patient is seated on a chair. It should rest firmly on the back. The dressing is done by two people. One person from behind spreads the patient’s shoulder girdles with his hands so that the inner edges of the shoulder blades are as close as possible to the spinal column. He must keep the shoulders in an open position at all times during the dressing. The second doctor simultaneously slowly and carefully presses with his thumbs on the top of the angle formed by the fragments of the clavicle. After this, the arm is fixed with a soft or plaster bandage. Plaster is used mainly after operations.
If within three hours after the procedure the patient’s hands do not begin to go numb, swelling does not develop, and there are no other unpleasant symptoms, the bandage is applied correctly. Otherwise, it is weakened a little. Of the above types of dressings, preference is given to those sold ready-made.
The Deso bandage is made as follows: the arm is bandaged to the body, while the shoulder is pulled back, and small pillows are placed on the armpit and forearm. When applying a Smirnov-Weinstein plaster cast, one strip is thrown over the forearm of the injured arm and healthy upper arm, and the second is over the sternum and shoulder.
Sometimes this type of bandage is used. The sternum is bandaged obliquely over the healthy shoulder, and the opposite shoulder joint is raised with a built-in crutch. This device is often used for complex clavicle fractures. This bandage is removed after about 3 weeks.
For the first 4 days after fixing the collarbone, the doctor conducts mandatory daily examinations. A control X-ray is taken a week later. Immediately after removing the cast, an x-ray should also be taken to identify secondary displacement, malunion, or complete nonunion of the clavicle.
Delbe rings for clavicle fracture
Soft Delbe ring straps are placed on the area between the patient’s neck and shoulders, pulled tightly and tied between the shoulder blades. Initially, this bandage was made using cotton wool and gauze. Modern headbands are much more convenient and practical. They can even be washed. They are sold ready-made and are perfectly adjustable. The application of such rings gives the patient a minimum of discomfort.
The figure-of-eight bandage gets its name because the bandages cross between the shoulder blades in a figure-eight shape. To make such a bandage, a thick cotton pad is attached to the patient between the shoulder blades brought together to the spine. Flat rollers are placed on the shoulders and armpits and bandaged as tightly as possible. After applying the bandage, be sure to check the correct position of the fragments using x-rays.
The Delbe shoulder fixator is produced by both domestic and foreign companies. It is made of very durable and yet soft material. It is also breathable and has several levels of belt tension. To select rings of the right size, you need to know the patient's chest circumference.
Functions of Delbe ring straps:
- securing the shoulders in a spread position;
- fixation of the acromial clavicular joint;
- unloading of the clavicle ligaments;
- holding fragments in the desired position.
Traumatologists prefer Delbe rings because of their ease of use and ease of adjustment of the degree of traction.
Surgery for a clavicle fracture
In cases where conservative treatment is powerless, surgery is performed. Many traumatologists and surgeons consider surgery the best method of treatment for a clavicle fracture. Metal structures are actively used. After the fracture has healed, they are removed. This usually occurs after a few months, although the plates may not be removed until after a year.
Surgical treatment involves performing one of the following types of surgery under general anesthesia:
- bone osteosynthesis with plates (including compression);
- intraosseous osteosynthesis with knitting needles or a stainless steel rod (for example, a pin, rod or nail of the Bogdanov type, tie bolts);
- with external fixation devices.
To secure the metal structures, channels are drilled into the bone. Types of plates for clavicle osteosynthesis:
- reconstructive;
- S-shaped;
- hook-shaped;
- with locking screws.
Two types of intraosseous osteosynthesis are performed:
- according to Klyuchevsky, if the central fragment is short;
- according to Spizhariom-Kupcher, if there is a small peripheral fragment.
To secure fragments, pins are also used: lockable or non-lockable. The former have additional fixation with screws. Channels are drilled into the bone into which pins are inserted. Inside these rods there are special holes for screws necessary for fixing the metal structure. Non-locking pins come in smooth and threaded types. The latter fix the bone more strongly (Rockwood pin).
Many doctors prefer to perform surgery for a clavicle fracture. It allows you to remove the fragments and firmly fasten the separated parts of the bone. After the operation, the rehabilitation period is slightly longer. But it is possible to avoid many unpleasant complications.
On topic: 12 folk methods for home treatment
Diagnostic methods
At an appointment with a traumatologist, the doctor initially asks under what circumstances this injury occurred, how much time has passed since it was received, and what symptoms are bothering you. Then he begins a procedure called “palpation”. These manipulations allow the doctor to understand the nature of the injury and check whether there is displacement of the fragments during the fracture. But with this diagnostic method it is impossible to make an accurate diagnosis, and therefore, the doctor sends the patient for radiography in two projections. After the specialist examines your images, he makes an accurate diagnosis and prescribes the most appropriate treatment for you.
Recovery period
Rehabilitation is absolutely necessary, because... Due to prolonged immobilization, the arm muscles partially atrophy. Exercises should be started as soon as possible. The load and type of activity is determined by the attending physician. Typically, the recovery course lasts from three to seven weeks.
The rehabilitation period can be divided into 3 stages:
- during immobilization, perform passive exercises;
- after the growth of callus and removal of the fixing bandage, use gymnastic sticks and expand the range of exercises;
- introduction of strength loads using expanders, dumbbells, clubs, exercise machines.
For a speedy recovery after a fracture, physiotherapeutic procedures are continued, hydrotherapy and massage are used. An integrated approach guarantees high rehabilitation results. Thanks to electrophoresis, magnetic therapy, ultrasound, laser therapy and UHF, blood flows more strongly to the damaged area. Sufficient blood supply promotes rapid tissue repair.
How to develop a collarbone after a fracture?
Exercises after conservative treatment and surgery are slightly different. But in both cases they become more complex step by step.
A set of exercises for the postoperative period:
- breathing and general tonic exercises;
- light active-passive rocking in the shoulder joint (arm on a bandage);
- alternate tension and relaxation of the muscles of the shoulder and shoulder girdle;
- active movements in the elbow and wrist joints, as well as in the fingers and hand;
- pronation-supination (inward-outward rotation) of the forearm;
- shrugs;
- general strengthening exercises for all parts of the body;
- dosed walking and running;
- training hand speed and strength endurance;
- sports-assist exercises;
- exercises to restore coordination of movements;
- sports training.
First, the exercises are performed with outside help for several minutes. Then they are repeated more often and longer. From smooth and slow movements they move to jerks. In order to quickly develop a collarbone after a fracture, you need persistence and patience.
Anatomical features
The collarbone, humerus and scapula make up the shoulder girdle. The acromioclavicular joint is a low-moving joint that connects the collarbone and scapula.
The joint is supported by bone formations that secure the joint with strong ligamentous tissue. The articular ends are surrounded by a closed capsule, which is filled with synovial fluid.