A transcondylar fracture of the humerus is recorded in victims quite rarely, but is recognized as a serious injury. It is formed when falling forward onto outstretched arms. Damage to the humerus most often occurs in childhood, which is associated with immaturity of the bones. In our article we will describe what a transcondylar fracture is, how it manifests itself, and how it is treated.
What is a transcondylar fracture of the humerus?
A transcondylar fracture of the humerus is an injury in which the humerus is damaged in the area of the condyles. They are called spherical thickenings at the ulnar end of the humerus. The fracture runs along their surface and its plane is located above the epiphysis (the expanded part of the bone) or passes through it. The fault line often runs in the transverse direction. Damage to the humerus belongs to the group of intra-articular injuries in which the function of the elbow joint is impaired. Due to the structural features, the fracture is more common in the right limb.
Causes and characteristics of trauma in adults and children
Damage to the humerus occurs when hyperextension or strong flexion occurs. The main cause of transcondylar fractures in children and adults is a fall on an outstretched arm or hand. This type of injury is considered an extension injury. In the flexion subtype of the transcondylar fracture, the person lands on the elbow with the limb bent. This subtype of injury is much less common. The main predisposing factor for this type is considered to be rarefaction and thinning of the bone tissue in the condyle area. The altered tissue is easily damaged by falls or impacts in the elbow area. The separation of bone fragments occurs under the influence of muscle force.
The reasons leading to bone loss are as follows:
- osteoporosis;
- long-term sluggish inflammatory processes in the bone;
- arthrosis of the elbow joint;
- malnutrition of bone structures;
- hormonal changes;
- diabetes.
Transcondylar fractures of the humerus in children occur due to the structural characteristics and immaturity of the bone tissue. They lead to low bone strength in this area of the shoulder. High mobility and increased susceptibility to injury predispose children to transcondylar injuries. They run, jump and fall more often than adults. For preschoolers and schoolchildren, a transcondylar fracture is considered typical.
Causes of fracture
In the case of children, the reasons for the occurrence of injury are clear - activity, bone flexibility and lack of fear due to future injury. Adults who try to avoid danger are also not immune to such damage. Belonging to a risk group increases the likelihood of a fracture in the presence of traumatic factors. What risk groups exist:
- Elderly age;
- People with bad habits (smoking, alcohol, drug addiction);
- Overweight people (large body weight increases the load during tramming);
- People with metabolic disorders and chronic diseases.
The cause of injury in both children and adults is careless falls either on the hand or on the forearm in the area of the elbow joint.
Attention! The peculiarity of the injury in a child is that it affects both the left and right hands. However, in adults, the right limb is injured statistically more often than the left. This is due to the fact that the right hand is often dominant and when a person falls, it is with it that he tries to arrest the fall.
Classification
There are transcondylar injuries with displacement and without displacement.
With offset
This type of injury to the humerus is most common in childhood. It occurs more often than a fracture without displacement. The muscles attached to the process necessarily stretch the fragments in different directions. A transcondylar fracture of the humerus with displacement in children occurs when they fall from their own height onto a slightly bent arm at the elbow joint or a fully straightened limb. In this case, the peripheral fragment (it is located on the outer surface of the bone) moves backward and upward, and the central one is displaced downward. For this type of injury to the humerus, rotational (rotational) displacement of bone fragments is typical; this happens in 40% of all cases of these injuries.
This migration of fragments is realized in three ways:
- When you fall on the forward shoulder and the forearm turned inward, the muscles that rotate the humerus outward tighten. In this case, the central fragment moves inward, the peripheral (located closer to the outer surface of the bone) fragment is pulled outward under the action of muscle traction.
- If you fall on your hand with your forearm turned outward and your shoulder turned inward, it will be different. The peripheral fragment is pulled inward and, and the central fragment is rotated outward. This occurs due to the contraction of the muscles that rotate the shoulder inward.
- When falling on the hand and simultaneously keeping the forearm in the middle position, rotational displacement does not occur. In this case, lateral displacement of the fragments outward or inward is possible. Circular displacements in the longitudinal and transverse plane of the humerus are possible.
Classification of injury
The complexity of a transcondylar fracture determines the need for its detailed classification in order to select treatment as effectively as possible and speed up recovery. The main primary categories for classification are the following distinctive general features:
- Nature of injury: open and closed fractures.
- Formation of fragments: with and without displacement.
The rest of the article presents specific categories for transcondylar fractures.
Traumatic injury to the proximal part
It is quite difficult to obtain this type of injury, because it is characterized as injury to the upper part of the humerus at the junction with the upper girdle through traumatic impact in the area of the hand or forearm. This category, in turn, also has two subtypes:
- Abduction is formed as a result of a traumatic effect on an elongated limb with abduction to the side. The fragments are displaced according to the following mechanism: the central fragment moves in the center, rushing upward. Therefore, an angle of more than 90 degrees is formed between the bone structures.
- Adduction - its occurrence is similar to the previous case, but differs in that the hand is not moved to the side. The mechanism of displacement of fragments changes as follows: the bone fragment rushes towards the center and to the side. Therefore, the risk of developing an open injury is high.
Diaphyseal fractures of the humeral region
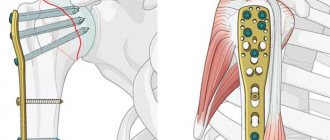
These types of injuries make up a larger percentage of other types of injuries. Damage to the diaphysis occurs due to the same traumatic factors - a fall on the forearm in the area of the elbow joint. At the same time, “scrolling” of the bone occurs, so most often a spiral-shaped bone fracture line or an oblique line is observed. The first option is fraught with the formation of many fragments. This means that there is a high probability that a specialist will choose surgical reposition of fragments using pins and screws.
Attention! Transcondylar fractures rarely occur without the formation of bone fragments. Such cases are more often observed in people with reduced muscle tone and poorly developed muscles.
Injury to the distal epiphysis
Dangerous injuries that increase the risk of consequences after rehabilitation. There is an internal detailed classification of fractures of the distal epiphysis. The primary categories are external and internal injuries affecting joint structures. External joint injuries include:
- Flexion is characterized by the fact that the bone is damaged in the following directions - from top to bottom and from the back surface to the outside. With such fractures, intense damage to muscle structures, large blood vessels and nerve fibers is observed. Therefore, the symptoms of such an injury are heavy bleeding and impaired sensitivity (its complete absence or occasional loss).
- Extensor is characterized by the opposite direction of mechanical action - from bottom to top and from the front surface to the back.
Intra-articular are divided into:
- Transepicondylar tears are the most common in the presented classification and are visualized in the form of the letters T or Y on an x-ray.
- Lesions of the lateral epicondyle and the head of the humerus are characterized by minimal trauma to the articular surface and the absence of fragments.
- Injuries to the medial epicondyle.
- Complex injuries, characterized by a combination of two or more of the injury options described by you.
Symptoms of a transcondylar fracture
Manifestations of this injury occur immediately after a fall or blow. The pain is so severe that the victim may lose consciousness.
A little later, other symptoms appear:
- Pain in the elbow area increases significantly even with slight pressure on the skin above the condyles.
- When you fall, you hear the crunch of a breaking bone.
- In the elbow area there is severe swelling of the subcutaneous tissue, the limb swells. The hand in this place becomes hot to the touch. The skin in this area turns red. Then the skin turns blue and a hematoma forms.
- The anatomical configuration of the elbow area changes. An unnatural position of the forearm is noted. It is inconsistent with the position of the shoulder.
- With an extensor fracture, a visible shortening of the limb is observed, and with a flexion fracture, the arm appears elongated.
- Active movements in the elbow joint are severely limited and painful. With passive movements, the crunching of fragments is heard.
With an open injury, a gaping wound is visible; bone fragments may peek out from it.
IMPORTANT Often, a transcondylar fracture of the humerus is accompanied by severe bleeding, since the area is well supplied with blood and large vessels pass through here.
Symptoms and diagnosis of injury
With a transcondylar fracture of the humerus, a small patient may experience the following symptoms:
- sharp pain in the elbow joint with its intensification upon palpation of the condyles;
- characteristic crepitation (crunching) of bone fragments;
- swelling of tissues in the affected area;
- hyperemia and cyanosis of the skin;
- with a closed fracture with displacement, a hematoma appears due to damage to the blood vessels; with an open fracture, the bones come out;
- passive movements in the elbow joint are limited;
- the hand below the forearm takes an unnatural position;
- Depending on the nature of the damage, the limb may appear longer or shorter than the healthy one.
After the victim is injured, swelling quickly increases - this complicates diagnosis. It is difficult for the doctor to palpate bone fragments
The traumatologist palpates and checks passive movements with great care to prevent displacement of bone fragments. If there is a suspicion of a fracture, the patient is sent for an x-ray
In addition to x-rays, the patient may be referred for consultation to a neurosurgeon if there is a risk of compression of the ulnar, median or radial nerve. The assistance of a vascular surgeon may also be required, although vascular ruptures from such fractures are rare in children.
In addition to standard diagnostic methods, the little patient will have to undergo a number of examinations:
- ECG;
- general blood and urine analysis;
- coagulogram;
- analysis of biochemical parameters.
Transcondylar fracture of the humerus in children
Bone tissue in children has a structure and metabolism that differs from that of an adult. The bone in the area of the humeral condyles has a sparse structure and lower strength. It is more vulnerable to damage to the humerus. The formation of transcondylar fractures in childhood is facilitated by a deficiency of protein, vitamins and microelements in the diet. At the same time, children are more mobile than adults. They are more likely to fall on their hands and get hit with their elbows on hard objects during games, running and fighting.
This type of injury to the humerus is quite common in the pediatric population. It accounts for up to 15% of all injuries in this age group. A transcondylar fracture in this location occurs much more often in childhood. It occurs especially often in boys between the ages of six and ten years. In children, closed-type injuries with displaced fragments are more common. They arise due to the effect of muscle traction on fragments.
IMPORTANT It is more difficult to diagnose a transcondylar fracture in children, since due to increased blood supply, swelling increases faster and a hematoma forms in the elbow joint. This makes it more difficult to palpate the fragments.
Diagnostics
A transcondylar fracture is identified by a surgeon or traumatologist. He finds out what is bothering the patient now and asks about the circumstances under which the injury occurred. The doctor then examines the affected area. Determines the volume of possible passive and active movements during rotation in the elbow joint, as well as flexion and extension. The doctor assesses the presence of deformity in the elbow area. He must ensure that there is no damage to blood vessels and nerves.
First aid
Before transporting the victim to the emergency room, first aid must be provided to the required extent. This is necessary so as not to worsen the damage to the humerus on the road. Before starting activities, you need to call an ambulance.
Before her arrival, you need to do the following:
- When there is a suspicion that the victim has broken the humerus, it is necessary to carefully immobilize the arm, avoiding aggravation of the injury to the humerus. You need to make a support bandage from scrap materials or use a ready-made splint. It is applied, immobilizing the entire arm (shoulder, elbow, wrist joint) at once. Before this, a soft cloth folded in several layers is placed under the elbow joint area. Then you should securely tape the limb to the body.
- If a wound is found in the damaged area, it should be washed and treated with antiseptics.
- When it is impossible to bend the arm at the elbow, the patient is placed in a supine position. Then it is fixed to the body. The joint should not be bent with significant force.
- You need to check your pulse regularly. If it becomes weak, the bandage is carefully removed from the arm for a while. It is straightened to restore blood circulation. Then, when it is restored, the arm is fixed again.
- After these measures, you should take the victim to the emergency room yourself if an ambulance cannot arrive. We need to hand the patient over to the doctors when she arrives.
IMPORTANT Painkillers should be given to the victim before transfer to medical workers only as a last resort. Otherwise, the clinical picture will be unclear. This will complicate the diagnosis.
Treatment
A transcondylar fracture must be treated using a set of measures. First, reposition of the fragments is carried out, followed by immobilization. Surgical correction is performed according to indications. Then drug treatment is applied. Physiotherapy, massage, and exercise therapy are used to restore the functions of the affected limb. Transcondylar fractures without displacement are treated on an outpatient basis, complex fractures with displacement in a specialized department of the hospital.
Conservative method
With the conservative method of treatment, reposition of the fragments is carried out, followed by immobilization. Three approaches are used depending on the type of damage to the epicondyles.
They are as follows:
- Patients with a fracture without displacement of fragments or minimal displacement that does not require reduction. The limb is immobilized by applying a splint. The arm is bent and suspended. It is kept in this state for two or three weeks. By the end of the first week, X-ray diagnostics are performed to identify secondary displacement of bone fragments after swelling is removed.
- For patients with significant displacement of bone fragments when the fracture plane is located across the bone, closed manual reduction is used to reduce the fragments. Then the arm is fixed in a bent position by applying a plaster cast. In this case, rotational, angular and lateral displacements are excluded. If they are not eliminated, the sharp end of the fragment may move towards the elbow and injure nearby soft tissues. Assuming fusion of the bone tissue in the event of rotation of the bone fragments, the elbow joint will not bend. Reposition is carried out under anesthesia.
- Patients with complex displacements of fragments, oblique planes of displacement of fragments, bleeding, nerve damage and a history of unsuccessful reduction of bone fragments undergo skeletal traction. They are being treated in hospital. Skeletal traction should slowly level out the displacement. For this, Kirschner wires or Marx staples are used, which are installed at the base of the olecranon. A load weighing two kilograms is suspended from them. Then the weight is gradually increased to five kilograms. Afterwards a splint is applied to the arm. On the third day of traction, X-ray control is performed. The procedure takes two and a half weeks. Afterwards, a splint is applied until the bone tissue defect is completely healed.
Fractures of the medial condyle of the humerus
They are rare in children; the fragment is most often slightly displaced and can be reduced bloodlessly, after which traction is applied on an abduction splint for an early start of gymnastics, fusion occurs by the 12-14th day. In case of large displacement, open reduction is performed through an incision on the anteromedial side of the ulna, the fragment is fixed with a knitting needle and sutures to the periosteum.
Fractures of the medial epicondyle are more often observed in middle-aged and older children. In children under 5 years of age, the diagnosis can only be made based on the clinical picture, since the cartilaginous epicondyle does not give a shadow on an x-ray. This injury occurs as a result of severe abduction of the forearm with hyperextension at the ulna as a result of tension on the medial collateral ligament and the flexor muscles of the forearm. The plane of the fracture often runs along the apophyseal zone, so these fractures have the character of apophyseolysis.
Clinically, swelling, hemorrhage and sharp pain along the inside of the elbow joint and an increase in the physiological valgus position of the elbow are noted. In fresh cases, before swelling appears, you can palpate a movable fragment displaced downward. With the elbow bent, it is easy to move the fragment upward with your finger and press it to the humerus, where it is fixed with a deep plaster splint from the middle of the shoulder to the base of the fingers. If there is a large hematoma, it is first emptied with a syringe.
Avulsion of the medial epicondyle often occurs in combination with subluxation or dislocation in the elbow joint, and if the reduction is inept, the fragment, along with the muscles attached to it, the ligament and the edge of the articular capsule, can become pinched in the joint gap between the trochlea of the humerus and the lunate notch of the ulna. The strangulated fragment blocks the joint, making movements almost impossible; the fragment cannot be felt on the inner surface of the elbow. The diagnosis of a fragment inserted into the joint is confirmed by radiographs.
The treatment method for these complicated fracture-dislocations is as follows:
1. In fresh cases (up to 3 days), under anesthesia, the dislocation or subluxation is resumed, the elbow is strongly valgused, the limb is extended, the hand is retracted to the dorsal radial side (to stretch the muscles attached to the fragment) and the subluxation or dislocation is again set. As a rule, the strangulated fragment slips out of the joint space. After this, the limb is bent at the elbow to a right angle, the fragment is moved upward with a finger and fixed with a plaster splint to the humerus. Immobilization is indicated for 18-21 days.
2. If the fracture is 4 to 10 days old, bloodless removal of the fragment is almost impossible. In these cases, during visual X-ray inspection, a single-toothed sharp hook is inserted through the skin of the anterior inner surface of the elbow, the fragment or the ligament and muscles attached to it are hooked, and when the elbow is valgused, they are pulled inward. After removing the hook, the limb is bent at the elbow to a right angle, the fragment is placed with a finger and pressed against the humerus with a plaster splint.
3. After 10-12 days, extracting the fragment with a hook is not always successful, and surgical intervention is required: an incision along the anterior internal surface of the elbow joint, removal of the embedded fragment, suturing it to the humerus by the periosteum or with a knitting needle (and sometimes complete removal with suturing of those attached to him muscles and ligaments to the humerus) and suturing the torn joint capsule, plaster for 18-21 days.
In all cases, if the fragment is displaced by more than 0.5 cm, its careful reduction is necessary, otherwise a slight flexion contracture and valgus deformity will remain for a long time.
The information presented in this article is intended for informational purposes only and cannot replace professional advice and qualified medical care. If you have the slightest suspicion that your child has one of the injuries described above, be sure to consult a doctor!
Rehabilitation
The process of rehabilitation of a transcondylar fracture in children and adults begins in the hospital. The main goal of all measures is to fully restore motor functions of the upper limb and prevent post-traumatic complications.
The following rehabilitation methods are carried out:
- Physiotherapeutic procedures improve blood circulation in tissues and relieve swelling. For this purpose, electrophoresis of drugs, magnetic therapy, weak electric currents and paraffin application are used.
- When exercising, a dosed load should be used. It is gradually increased after the formation of callus. To expand motor range, the use of violent movements is unacceptable. A set of exercises is individually developed by a rehabilitation specialist, taking into account the patient’s condition. Classes are conducted under the supervision of an instructor.
- Massage of a broken limb begins only after the formation of a callus. This procedure improves blood circulation, increases muscle tone, and increases the elasticity of tendons. At least ten sessions are carried out.
The patient must adhere to a special diet during the period of bone fusion. It is necessary to increase the content of protein components and foods rich in calcium, vitamin D and B vitamins in the diet.
About rehabilitation
If the bones have fused completely, the recovery period begins. Rehabilitation includes undergoing physical therapy and performing a complex of physical therapy. The duration of the recovery period is 1-2 months. Return to full working capacity occurs in 3-4.5 months.
Rehabilitation is based on physiotherapy procedures:
- Electrophoresis;
- Ural Federal District;
- Ultrasound treatment.
To restore the motor function of the shoulder, a course of physical therapy is carried out
Exercises are performed carefully, without sudden movements, as this can be dangerous for the fused bones. You cannot strain your shoulder during physical exercise; if pain occurs, procedures are temporarily suspended
Humerus fractures are injuries that must be treated immediately. Trauma poses a particular danger in a child during the period of intensive bone tissue growth. Even if signs of a fracture do not appear immediately, after a fall or blow it is necessary to seek medical help in order to make a correct diagnosis and prevent complications.
Possible complications
The main negative consequence is considered to be limitation of motor functions of the upper limb in the elbow joint.
Complications of this injury also include:
- preservation of severe pain syndrome;
- formation of a false joint;
- incorrect splicing;
- internal soft tissue pressure ulcers;
- distant necrosis of fragments;
- development of arthrogenic contracture;
- neurological disorders due to damage to nerve trunks;
- post-traumatic arthrosis in the elbow joint.
Complications of transcondylar fractures in children mainly manifest themselves in the form of various neurological disorders; the function of the radial nerve is most often affected.
IMPORTANT Complications arise as a result of late consultation with a doctor and neglect of his recommendations.