The elbow joint belongs to the group of complex ones, since it combines three joints of three different bones: the radius, ulna and humerus. This is why the anatomy of the human elbow joint is incredibly complex, because it must be considered in the context of three different joints united by one articular capsule.
All kinds of diseases, developmental disorders and injuries can also affect one of the areas of the elbow or all at once - it depends on the severity and location of the pathology. In order to consistently understand this issue, you should study in detail each component of the elbow, its features and structure - only in this way can you understand the basic anatomy of this most important joint of the upper limb.
Elbow joint: anatomy and bone functions
The human elbow is formed by three bones of different volume and density - the ulna, radius (their proximal part) and the humerus (respectively, the distal part).
Brachial bone
This bone is a clear example of the dense and incredibly strong tubular bones of the human body, the shape of which smoothly transitions from perfectly round at the top to triangular at the bottom. Such features allow the distal end to ideally articulate with the bones of the forearm, the medial end to adjoin the ulna, and the lateral end, respectively, to the radius. At the same time, the medial surface has a smoother structure, and the lateral surface is spherical, which largely explains the physiology and characteristics of the trajectory of the elbow.
The surface of the humerus is covered with pits and depressions of various shapes and sizes, thanks to which a tight interaction of the elements of the elbow joint is formed. So, for example, above the medial surface there are small holes into which, when bent, the processes of the ulna - the coronoid and ulna - fall. These processes seem to fix the elbow in the grooves, supporting the joint capsule and protecting it from injury. In the medial and lateral epicondyles, which are quite easy to palpate at the distal end of the bone, there are attachment points for muscle fibers and ligamentous apparatus. And the spiral groove serves as the location of the radial nerve, which innervates the tissues of the upper limb.
Elbow bone
The triangular ulna bone is more voluminous and powerful than the radial bone. At the upper end it has a significant thickening with a trochlear notch, to which the humerus tightly adjoins, as if enveloping it. The lateral edge, accordingly, is adjacent to the radius.
The surface of the ulna is also heterogeneous, and for good reason. On the anterior and posterior surfaces of the trochlear notch there are two processes that limit the mobility of the elbow and ensure the normal physiology of the joint - the coronoid and ulnar. Following them is a special tuberosity, which is necessary for a stronger attachment of the brachial muscle. And below, at the distal end, there is a head with another process - the medial styloid, thanks to which the articulation of the ulna and radius bones is partially supported.
If desired, the anatomy of the ulna can be examined not only in pictures, but also on your own hand - this bone can be easily and painlessly felt under the skin along its entire length, starting with the dense muscular skeleton in its upper part and ending with the tendon bursa in the lower part. A certain anatomical structure, coupled with an adequate amount of muscle and fatty tissue of the arm, allows us to even see the head of the bone, which normally protrudes slightly on the inner back surface. All this greatly facilitates the identification of injuries and structural anomalies of the upper limb - with the proper skill of the physician, a correct diagnosis can be made even before an x-ray, which is required to clarify the clinical picture rather than for diagnosis.
Radius
The radius bone, together with the ulna, forms the forearm, however, unlike the latter, it is less durable and has a thickened lower rather than upper section. This structure allows you to achieve balance in the structure of the forearm and elbow joint. The small diameter and vulnerability of this bone requires special protection from the body, therefore, as a rule, it is surrounded throughout its entire length by well-developed muscle fibers, securely fixed in the pits and tuberosities. All this allows not only to prevent the occurrence of injuries and damage, but also to develop mobility, slightly expanding the capabilities of the normal physiology of the elbow joint.
Development of bone structure
The ulna is one of those elements that are formed in the womb and are present to a person from birth. In the first weeks of life, it is a long bony shaft, and only by 4 years of age does the hyaline cartilage at the distal end begin to ossify, forming the distal epiphysis. This happens in the wrist area.
Thin hyaline cartilage remains between the new formation and the diaphysis, gradually develops and prevents fusion of the epiphysis and diaphysis. By the age of 10 years, the proximal end has completely ossified and the proximal epiphysis has formed.
During puberty, the bones fuse to form a single ulna.
Sections forming the elbow joint
Since the elbow is a complex joint and consists of three bones connected in pairs to each other, in anatomy it is customary to distinguish three interconnected sections of this joint, surrounded by one articular capsule:
- Shoulder-ulnar joint
. It is formed by the trochlear structure of the humerus and the notch of the ulna, which normally connect and fit tightly together like puzzle pieces. It allows you to move your forearm, bending and extending your arm. - Humeral joint
. This articulation is formed at the point of contact of the articular fossa of the radial and condylar heads of the humerus. In shape it is classified as spherical, however, the features of the anatomical structure allow movements not in three, but only in two projections (flexion - extension plus rotation), since the third is limited by the presence of the adjacent ulna and a strong ligamentous apparatus. - Proximal radioulnar joint
. The cylindrical articulation of the radius and ulna bones supports the capabilities of the elbow, ensuring mobility of the arm along the longitudinal axis, that is, its rotation.
Blood supply and innervation of the adjacent area
Complete nutrition of the elbow joint is provided by the powerful blood network that surrounds it. Arterial blood enters the muscle fibers adjacent to the articular surface from the superior and inferior collateral ulnar arteries, as well as the recurrent, median and radial arteries. Having enriched the cells and tissues with oxygen and nutrients necessary to maintain physiological functions, it is sent through the veins of the same name to the venous basins of the upper extremities - the brachial, ulnar and radial. The lymph flow of the elbow joint passes in a similar way, moving through the lymphatic vessels to the elbow lymph nodes.
The innervation of the capsule that unites the sections of the elbow joint is carried out by the largest nerve fibers of the arm - the branches of the ulnar, radial and median nerves. This explains the high sensitivity of the tissues adjacent to the elbow and the particular pain of the resulting injuries.
Read also[edit | edit code]
- Elbow and forearm
- Elbow joint in children (anatomy)
- Sports elbow injuries - treatment
- Elbow ligament damage
- Lateral epicondylitis - treatment
- Medial epicondylitis - treatment
- Pain in the back of the elbow joint
- Compressive neuropathy of the radial nerve
- Cubital tunnel syndrome
- Hyperextension in the elbow joint
- Taping the elbow joint
- Diseases and injuries of the elbow joint during sports
- Tendopathies of the elbow joint in athletes
- Elbow instability
- Osteochondritis dissecans of the head of the humeral condyle
- Traction apophysitis
- Deforming arthrosis of the elbow joint
Muscles and ligaments of the elbow joint
The structural features and enormous functionality of the upper limbs are largely possible due to the anatomy of the human elbow joint. It is this joint that maintains mobility and ensures full activity of the upper limb, so the muscular-ligamentous apparatus of the elbow simply cannot have a simple structure. Let's consider each of these elements in order to understand the relationship between the anatomical structure and physiological capabilities of the elbow joint.
Muscular apparatus
Greater strength, physical capabilities and flexibility of the arm are provided largely due to the muscles acting on the elbow joint. Since the movements allowed in the elbow affect two planes - flexion/extension and pronation/supination - all muscle fibers can be divided into 3 significant groups:
1. Elbow flexor muscles
Such a movement is possible due to the contraction of muscle fibers, which, as it were, tighten the forearm, reducing the angle formed by it and the shoulder. The most powerful flexor of the upper limb is the biceps, located parallel to the humerus. In addition, this largest muscle is able to partially participate in supination of the forearm and rotation of the palm.
Additional muscles that flex the arm are the brachialis and brachioradialis. They (although they are considered auxiliary) in case of injury to the biceps are able to compensate for lost functions by performing full range of arm movements.
2. Extensors of the upper limb
Antagonist flexor muscles perform the exact opposite function, increasing the angle between the free end of the forearm and the shoulder of the upper limb. These include the triceps (triceps) and olecranon muscles, as well as the tensor fascia of the forearm. The triceps, like the biceps, is parallel to the humerus, but is located not anteriorly, but posteriorly, from the olecranon to the scapula. Together with the ulnar muscle fibers, it contracts and causes extension of the forearm in the elbow joint until the olecranon process fixes the humerus (the maximum allowable physiological extension of the arm).
3. Rotator muscles
This group is responsible for arm rotation - pronation and supination. The pronators that rotate the forearm in and out at the elbow joint include the pronator teres and quadratus muscles, as well as partly the brachioradialis muscle. And the second group - the instep muscles, which perform movements with the forearm from the inside - combines the instep muscle, the brachioradialis muscle and the biceps.
Elbow ligaments
The general joint capsule surrounding the elbow is not strong enough to hold all the large bones of the upper limb in a single joint, especially on the inside. High loads on the arms during physical work and sports training would invariably lead to damage to the elbow if it were not for the strong ligamentous apparatus that reliably holds the elbow and ensures its limited mobility. It includes the following fibers:
- The radial collateral ligament connects the epicondyle of the humerus and the head of the radius, then splits into two bundles and, enveloping the head in a kind of ring, is attached to the radial notch of the ulna. During life, the upper part of this ring gradually intertwines with the tendons responsible for extension, partially fulfilling their function and preventing overstretching; and the deep fibers form a single structure with the annular ligament.
- The ulnar collateral ligament extends from the medial epicondyle of the humerus to the trochlear notch of the ulna. Together with the radial collateral ligament, this ligament limits the mobility of the elbow, preventing lateral movements.
- The annular ligament is a kind of “sealing ring” that covers the articular circumference of the head of the radius, additionally fixing it at the ulna.
- The quadrate ligament connects the ulna bone to the radial neck, reliably fixing them to each other and preventing divergence or hyperextension.
Speaking about the ligamentous apparatus of the human elbow joint, it is impossible not to mention the interosseous membrane - a special structure that, although anatomically, does not belong to the ligaments, but performs a single function with them, fixing the bones of the forearm in the sections of the joint. It fills the small gap formed by the surfaces of the radius and ulna bones and forms a strong radioulnar syndesmosis. The tightly woven fibers of this membrane have special openings through which the vessels and nerves of the elbow pass, and the edges serve as attachment points for some muscle fibers.
Treatment
Treatment tactics include repositioning the fragments and fixing the arm for the period necessary for fusion. If the fracture is open, primary surgical treatment of the wound is required.
Depending on the characteristics of the damage, tactics can be conservative or operative.
Conservative treatment
If there is no displacement, conservative therapy is carried out. A fixing plaster bandage is applied to the forearm. For simple displaced fractures, closed reduction is sometimes possible.
It usually takes 4-5 weeks of immobilization to restore the integrity of the arm. During the process, control radiographic studies are carried out.
Rice. 4 Radiographs show a displaced fracture of the distal metaepiphysis of the radius; a – direct projection, b – lateral.
Fig.5 a, b. Radiographs of the wrist joint after closed manual reduction: the displacement has been eliminated, the position of the fragments is satisfactory.
Surgery
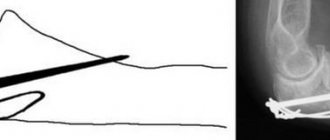
If the displacement is significant and unstable, or there are small fragments, then reposition is carried out surgically, and fixation is provided by metal structures: screws, plates. If the fragments can be combined without surgical access, then percutaneous fixation with knitting needles is used.
Rice. 6 a. fracture of the beam in a typical place with displacement; b. condition after osteosynthesis of the radius with a plate and screws.
Physiology of the human elbow joint
The normal physiology of the human elbow joint implies fairly extensive mobility: even without special training, the bones of the forearm and shoulder can rotate 90°, bend up to 150° and extend another 10° in the opposite direction (that is, as if beyond the elbow). Moreover, these degrees are not the limit - with certain skill and careful training, the mobility of the elbow joint can be increased several times, clearly demonstrating the almost limitless capabilities of the human body.
It should be borne in mind that such functionality requires special attention when loading the elbow joint. Although it belongs to the group of hanging ones and does not formally serve as a support, the size and number of loads does not decrease from this. This is particularly due to physical work, weight lifting, sports training and other activities that involve the upper extremities. As a result, any careless movement performed without proper preparation and warming up of the ligamentous-muscular system can be fraught with a painful elbow injury that requires long-term treatment. Therefore, you should take care of your own body and regularly strengthen it with gradually increasing loads as part of physical exercises - only in this way can you develop your elbow joints, making your arms truly strong, resilient and flexible.
Causes
The injury usually occurs when falling on an outstretched arm. If a person stumbles or falls into ice, then the probability of damage to the beam is very high. This injury often occurs in childhood or in people who play sports, which is associated with high mobility and a high incidence of falls. It may also occur in the event of an accident or at work.
In older people, the cause of the damage is osteoporosis. Even a minor impact causes a fracture.