A comminuted fracture is one of the complex types of injuries in which bone fragmentation occurs with the formation of three or more fragments. Damage to bone tissue can occur as a result of longitudinal or transverse force applied to the bone during falls, car accidents, sports, industrial and domestic accidents. Such a fracture is considered a dangerous injury and therefore requires immediate first aid and hospitalization.
Photo 1. Comminuted fractures often require not only a cast, but also surgery. Source: Flickr (Kaitlyn Hodnicki)
What is a comminuted fracture
Violation of the integrity of the bone with the formation of several fragments can occur in any part of the body. This type of injury is divided by location into fractures of the skull, spine, lower and upper extremities.
Long tubular bones are most often susceptible to such fractures:
- ulna;
- shoulder;
- femoral;
- radial;
- tibial
These bones often suffer from fractures with the formation of fragments as a result of the application of great force - a blow from a hard object, a fall while supporting an arm or leg, or rotation (for example, in a work-related injury involving a working mechanism).
Comminuted skull fractures occur when the head is hit with a hard object or a heavy object falls on top of the head .
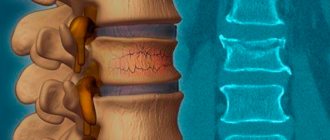
Compression fractures of the spine with the formation of splinters are often diagnosed in the cervical spine as a result of non-compliance with safety precautions. Often, fractures of the cervical spine and severe traumatic brain injuries occur while relaxing in unfamiliar open waters when diving upside down and subsequently colliding with underwater objects (snags, stones).
Causes of injury
A compression-comminuted fracture of the lumbar spine is not so easy to obtain. This form of injury occurs when too much pressure is placed on the body and the spinal column seems to compress. Under the influence of forces, the vertebrae cannot withstand and crack. The stronger the impact, the higher the likelihood that one or more fragments will break off.
Much less often, injuries are diagnosed due to strong twisting or a direct blow to the area of future injury.
Most often, people involved in extreme sports, acrobatics, and skydiving suffer from a comminuted fracture. You can get damaged by getting into a car accident.
Differences and danger of comminuted fractures
The main difference between comminuted fractures is significant damage to the bone, in which fragments can be displaced. This is the main danger of such an injury - fragments with significant mobility tear soft tissues , main blood vessels , nerves , tendons and skin .
If the injury leads to displacement of a fragment close to a large artery, then the presence of a bone fragment poses a threat to the life of the victim due to blood loss .
Note! Displaced comminuted fractures of the skull are fraught with damage to the lining of the brain and serious complications in the form of neurological disorders, coma and vegetative state, and brain death.
Comminuted fractures of the lower extremities
The most common fractures are comminuted fractures of the femur and tibia. In the first case, special skeletal traction is most often used for treatment, under which the patient must remain for at least 2 months. But if this fracture has displacements that require surgical intervention, skeletal traction is prescribed to the patient only after a successful operation to shift the bone fragments and fasten them together.
Skeletal traction using a kettlebell counterweight
A tibia fracture can be mild, and then the bone fragments can be put together without surgery, after which a cast is applied, which the patient wears for 1-1.5 months. If the fracture has a complex shape and the lower leg is severely deformed, surgical intervention cannot be avoided. Surgeons set the tibia and fix the broken bone pieces with screws and a plate. And only then the patient is put in plaster.
- Open fracture of the tibia
Kinds
There are comminuted fractures: closed and open, extra-articular and intra-articular, with displacement of fragments and without displacement.
Closed comminuted fracture
With this type of injury, soft tissue and skin remain intact, although internal bleeding due to damage to blood vessels by bone fragments. A sign of a closed fracture with hidden bleeding is the formation of a hematoma and severe swelling of the limb.
Open comminuted fracture
An open fracture is diagnosed when a separated bone fragment, having shifted significantly, tears muscles, tendons and skin , coming out. If soft tissue is damaged, severe bleeding occurs.
With and without displacement of fragments
If a significant force is applied to the bone, the latter can split into several fragments. If the force of impact is combined with a change in direction, the fragments can move relative to the bone. Displacement of fragments can occur if the injured limb is not immobilized in a timely manner or if the recommendations of the traumatologist are not followed.
Significant mobility of the fragments complicates the treatment of the fracture , making it difficult to reposition - restore the correct position of fragments of crushed bone.
Extra- and intra-articular fractures
With intra-articular injuries , the bone fracture line completely or partially passes through the joint cavity, which leads to injury to the cartilage tissue and rupture of the joint capsule. Extra-articular fractures are limited to the distal parts of the tubular bones, without affecting the articular capsule.
Additional complications
The above type of injury can be complicated by dislocation (for example, of a limb) or subluxation. Also, along with a broken bone, there may be a problem of sprained ligaments or even rupture.
The fragments can cause severe damage inside soft tissue. If a person is moved or ambulates independently, fragments of the broken bone can sever the nerve processes and continue to move within the soft tissue, resulting in additional tears, cuts, etc.
Surgeons can also place sutures on damaged nerves or use special plastic surgery to restore them. But there are situations when damaged nerves cannot be restored and the patient remains disabled, for example, acquiring a limp for life.
Causes
Like other types of bone tissue trauma, comminuted fractures can be traumatic and pathological . The first are caused by external influence of kinetic energy exceeding the tensile strength of the bone: during road accidents, accidents, sports injuries.
Pathological bone fractures are associated with changes in the structure of bone tissue under the influence of internal negative factors. For example, osteoporosis—increased bone fragility—usually causes hip fractures in older people.
Note! Tuberculosis, osteomyelitis, malignant tumors and other diseases can reduce the strength of bone tissue and increase the risk of fracture. With demineralization of bone tissue, fractures occur even with relatively small loads on the limb.
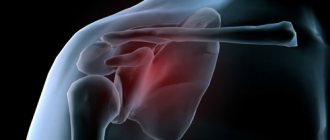
Periarticular fractures
For periarticular injuries in the area of the shoulder joint, combinations of fractures of the surgical neck of the humerus, the neck and processes (acromial and coracoid) of the scapula, and the acromial end of the clavicle are characteristic.
The mechanism of formation of these injuries is associated with indirect trauma (falling on the shoulder). It can be represented in two ways: 1) the occurrence of fractures of the processes and neck of the scapula due to direct pressure from the head of the humerus, the surgical neck of which breaks after them; 2) the occurrence of a fracture of the acromial end of the clavicle and a fracture of the humeral neck from the general direct action of force on the shoulder girdle. Surgery is required only for fracture-dislocation of the humeral head and fracture of the coracoid process. Treatment with plaster splints on an abduction splint gives good results. Consolidation of concomitant fractures of the scapula and clavicle was noted within 4 to 6 weeks. Against the background of a fracture of the surgical neck of the humerus, clinical symptoms of damage to adjacent bones almost do not appear.
Signs of a comminuted fracture
Diagnosis of a comminuted fracture is possible based on external signs, as well as x-rays and computed tomography of the damaged bone. External signs of a comminuted fracture:
- forced unnatural position of the arm/leg;
- severe bleeding and an open wound (with an open fracture);
- crepitus (crunching in the area of the fracture);
- deformation and/or pathological mobility of the limb;
- denervation or severe pain ;
- swelling of the injured limb;
- hematoma in the area of injury.
Comminuted fractures of tubular bones lead to significant limitation of mobility when trying to move the injured limb. If the bones of the pelvis, hip or leg are fractured, the victim cannot walk, stand or sit.
How to recognize a fracture
An accurate determination of the nature and severity of the fracture is possible after an X-ray examination. However, there are signs of a fracture that everyone should know in order not to aggravate the damage to bone and soft tissue and to alleviate the condition of the victim. Let's list them.
- Pain that occurs immediately after the fracture and subsides somewhat at rest. With the slightest movement or palpation it intensifies.
- Impaired musculoskeletal function of the bone.
- Deformation of the damaged organ : unnatural position, curvature of the axis of the limb, reduction in its length, edema.
- A crackling, crunching sound (crepitation) when palpated due to the friction of the edges of the fragments against each other.
- Presence of hematoma , subcutaneous hemorrhage.
First aid
If a comminuted fracture occurs, especially an open one, it is necessary to urgently provide first aid to the victim.
Note! In case of an open fracture, it is prohibited to independently move, reduce or remove bone fragments. Only a doctor can do this!
If you suspect a closed comminuted fracture, you must:
- firmly fix the limb , ensuring its absolute immobility;
- in case of an open fracture with bleeding, apply a splint or tight bandage above the area of injury;
- apply cold to the damaged area;
- in case of severe pain, give the victim a painkiller .
As soon as possible, the patient is hospitalized in the traumatology or surgery department.
Rehabilitation after injury
In order for recovery after a comminuted fracture of the L1 vertebra or other area to be successful, you need to carefully follow the recommendations of an orthopedic traumatologist
and don't overload your body.
In the first six months, doctors require you to wear a corset, and also prescribe a complex of exercise therapy, individually selected for the patient. Serious activity is excluded - there is a danger of injury to the nerve roots by the displaced vertebra.
The further course of rehabilitation depends on what happens in the first months. A long recovery may be required with a gradual return of mobility to the limbs - some patients learn to walk again. In the later stages, massage, acupuncture and other similar physiotherapy techniques are prescribed.
Complications and consequences
A comminuted fracture has serious negative health consequences. The main danger is the displacement of bone fragments with damage to blood vessels, tendons and nerves . This can lead to the following violations:
- denervation (loss of sensation) of a limb due to nerve damage;
- limited mobility of an arm or leg due to a tendon injury;
- infection of soft and bone tissues during an open fracture;
- impaired blood supply to the extremities due to damage to a large vessel.
Proper and timely medical care will minimize the likelihood of complications from comminuted fractures.
What might be the consequences?
Comminuted fractures of any bone are dangerous. People who have sustained such an injury require immediate and appropriate medical care. The fragments can tear soft tissues and lead to severe blood loss. If a person is not given first aid on time, he may even die from severe blood loss.
Fragments of broken bones can rupture blood vessels and nerve processes. It is not always possible to restore them. And then the person will most likely remain disabled. Due to nerve rupture, paralysis of individual parts of the body is also possible.
Features of treatment of comminuted fractures
Treatment of comminuted fractures can be conservative or surgical, depending on the type and severity of the injury and its location. Damage to the bone with the formation of fragments without displacement allows the surgeon or traumatologist to perform a closed reposition of the fragments - restoring their anatomically correct position without surgical intervention. After repositioning the fragments, an X-ray of the bone in the area of the fracture is taken and a plaster cast is applied.
In case of open comminuted fractures, the wound is sanitation with the removal of severely damaged and non-viable bone fragments. In severe cases, surgical treatment of fractures is indicated - osteosynthesis using metal knitting needles, pins, plates, three-blade nails and other devices. If nerves and blood vessels are damaged, the surgeon restores the integrity of the vascular walls and nerve bundles.
Injury to the shoulder girdle and arms
The upper body is most often injured.
The most common fractures of the shoulder girdle and arms include the following:
- broken collarbone;
- broken humerus;
- fracture of the forearm bones;
- broken olecranon.
A clavicle fracture is usually closed and can only be complicated by a large number of fragments. If the number of the latter is significant and their location threatens to violate the integrity of blood vessels and arteries, then surgeons perform surgical intervention, during which the fragments are assembled into a single whole using special plates, as well as screws and knitting needles. Next, Delbe rings and Smirnov-Vanshtein bandages are applied. In cases where the shard displacement is minimal, closed shard matching is used. In this case, the patient is placed under anesthesia.
Fixing the hand in a stationary state
In cases where the humerus, forearm bones or olecranon are broken, surgery is usually necessary. If there is no such need, and the X-ray results indicate that it is possible to make a closed comparison of bone fragments, then doctors always choose this option. And after the necessary manipulations, the injured bone is securely fixed until it heals.
But if the fracture is complicated and requires immediate intervention by surgeons, then the integrity of the bones is restored to the patient using surgical devices: knitting needles, metal plates, bolts, pins and screws during surgery.
Preventive measures
Complex cases of comminuted fractures of tubular bones lead to changes in the length of the lower limb. This deformation can lead to disastrous consequences for human health - curvature of the spine, gait disturbance, and diseases of internal organs.
Photo 2. Rehabilitation should take place under the supervision of a specialist. Source: Flickr (Exogen).
To maintain normal leg length, special devices are used that require a long course of rehabilitation.
Most cases of comminuted fractures require qualified assistance from a surgeon, traumatologist, neurologist and orthopedist. Specialists must assess the severity of damage to bones, tissues, nerves and blood vessels, and choose the right treatment tactics.
To avoid complications and recover quickly, you need to follow the doctor’s recommendations - stay in bed , wear plaster casts and other fixing devices, engage in exercise therapy and undergo physiotherapy courses .
Rehabilitation period
Most often, comminuted fractures require surgical intervention, and accordingly, the recovery period after such treatment will be more difficult and lengthy. If an operation was carried out to collect the fragments into a single whole, and surgeons used special fasteners to fasten them, then the patient is prescribed painkillers throughout the entire recovery period. They are intended to relieve pain that may occur in the patient’s body not only from the injury itself, but also due to the presence of foreign objects (plates, knitting needles) in the body.
When the X-ray results show that the patient is ready for the next stage of the recovery period (the formation of a bone growth should begin on the damaged bone), the plaster cast will be removed or the skeletal traction will be removed, after which regular visits to physiotherapeutic procedures, in particular electrophoresis, will be prescribed. The latter promotes accelerated healing of bone tissue.
On average, the period of complete recovery after receiving comminuted fractures can range from 1 to 2 years.
After the above type of bone damage, you should not rush too much when trying to fully load the injured area. Loads should be minimal and the return to normal functioning (for example, a broken leg) should be gradual, so as not to aggravate the situation and avoid a re-fracture.
Introduction
Epi- and metaepiphyseal fractures of the bones of the knee joint are considered severe injuries to the musculoskeletal system due to significant impairment of limb function and represent a serious problem in traumatology and orthopedics today. In recent years, there has been an increase in the number of victims with intra- and periarticular fractures of the bones of the knee joint, most of which are comminuted, which is explained both by an increase in the number of high-energy injuries in road traffic accidents and catatraumas, and by an increase in the number of patients suffering from concomitant osteoporosis [1, 3 ]. The aging of the population, senile and postmenopausal osteoporosis cause a sharp increase in the number of victims with injuries to the distal femur and proximal tibia in old age [1]. The development of hypostatic pneumonia, bedsores, the inability to stay in skeletal traction for a long time, and concomitant somatic diseases force traumatologists to abandon conservative treatment methods and more often operate on patients in order to quickly mobilize them [7, 8, 10]. Complex comminuted intra- and periarticular fractures of the bones of the knee joint against the background of concomitant osteoporosis create a certain problem in choosing the most effective method of surgical treatment [4]. The use of immersion osteosynthesis is accompanied by the need to use a massive fixator, to carry out a significant surgical approach for adequate reposition of bone fragments, which causes trauma to the soft tissue surrounding the fracture during the operation, is accompanied by blood loss, further impairs the blood supply to the fracture zone, and causes disruption of venous and lymphatic outflow from the area damage and as a result leads to delayed consolidation, fracture nonunion, formation of a false joint, development of osteitis and osteomyelitis [5, 9, 11].
Currently, peri- and intra-articular fractures of the bones of the knee joint require surgical treatment in order to restore the damaged articular surface and the normal axis of the limb. Based on our experience in treating these types of injuries, the most preferable method is transosseous osteosynthesis using rod and wire-rod devices of an original design. This method allows for low-traumatic osteosynthesis without immobilization of the damaged joint; the operation takes much less time and is accompanied by a significantly smaller number of purulent-infectious complications.
The purpose of this study was to analyze the results of treatment of intra- and periarticular fractures of the knee joint bones in patients who underwent transosseous osteosynthesis with devices designed by A.I. Gorodnichenko.
Material and methods
Since 1997, the Clinic of Traumatology and Orthopedics has operated on 105 patients with intra- and periarticular fractures of the knee joint bones. There were 42 patients with fractures of the distal femur and 63 patients with fractures of the proximal tibia. It should be noted that out of 105 victims, 22 (21%) had multiple and combined injuries, among which the leading place was occupied by traumatic brain injury - 13 (59.1%). 11 (50%) victims had fractures of other segments (except the knee joint). In 9 patients, transosseous osteosynthesis was performed on both sides, therefore, in 105 patients, 114 surgical interventions were performed using rod and wire-rod devices designed by A.I. Gorodnichenko.
The rod apparatus refers to unilateral multiplanar external fixation devices and consists of two support plates with longitudinal slots, in which spacer frames with tightening bolts and rod holders are installed. The plates and spacer frames of the device are made of high-strength radiolucent carbon fiber, used in the defense and aerospace industries, which allows you to control the accuracy of closed reduction in all projections both during surgery and in the postoperative period. In addition, the presence of carbon fiber elements significantly reduces the weight of the structure. The device allows you to insert rods, guided solely by the nature of the fracture and without limiting the surgeon in choosing the plane and angle of insertion of the rod, not only within the width of the device body, but also outside it due to the presence of special external brackets. The rod holders in the device move freely and self-align during the reduction process, without interfering with the elimination of all types of displacement of bone fragments, which is why they were called “floating” [2]. The device provides mutual reduction of bone fragments in 6 degrees of freedom, and after reposition by tightening two nuts on each rod holder, all 6 degrees of freedom are fixed, which ensures strong and stable fixation of bone fragments until complete consolidation of the fracture.
The spoke-rod apparatus consists of a base in the form of a rod apparatus, as well as two remote brackets connected to each other, fixed to the body of the apparatus at one of its ends and forming a semi-ring. At the end of the body and the free end of the semi-ring, there are clamps located in the same plane and made in the form of spoke holders with spoke tensioners, which allow you to adjust the degree of their tension and create counter-lateral compression of bone fragments.
The method is low-traumatic, technically simple, allows surgery on the first day after the patient’s admission to the hospital and does not require lengthy preoperative preparation. We have used a fundamentally new approach to the treatment of knee joint fractures using a rod-based external fixation device. In transosseous osteosynthesis of distal femur fractures, cannulated spongy rods with a special thread were used for insertion into the condyles through small incisions, which minimize the risk of surgery and blood loss. The rod is made hollow to accommodate a knitting needle, has grooves for squeezing out bone chips, a self-tapping threaded part and a thrust collar for compression of bone fragments along the fracture line. The use of this rod-based device is low-traumatic, the operation takes less time than when using submersible osteosynthesis and pin devices, and the risk of damage to the neurovascular trunks is eliminated due to its one-sided location, and the stable fixation created allows patients to begin mobilizing in the early postoperative period. Our experience has shown the simplicity and safety of osteosynthesis with this device, the minimal invasiveness of the operation and the high stability of fixation of bone fragments even in patients with osteoporosis.
Indications for osteosynthesis using external fixation devices designed by A.I. Gorodnichenko were open and closed fractures of the knee joint bones of types 33A2.3, 41A2.3, 33B1.2, 41B1.2, 33C1.2.3 and 41C 1.2.3 according to the AO/ASIF classification [6].
All surgical interventions were performed on an orthopedic table under the control of an electron-optical converter. Reduction of the fracture, as a rule, was performed closed and only in case of comminuted intra-articular fractures of type C3, open reduction was used in order to more accurately restore the congruence of the articular surfaces. The number of inserted rods was determined depending on the nature of the fracture and the presence of concomitant osteoporosis. 3 spongy rods were inserted into the area of the condyles of the femur or tibia, 2 of which were placed at the same level and secured in the same spacer frame. Three cortical rods were inserted into the diaphysis of the femur or tibia. The final reduction was achieved on the operating table, which was greatly facilitated by the presence of the main elements of the apparatus made of radiolucent carbon fiber. To enhance the rigidity of fixation and increase the stability of osteosynthesis, we used the technique of introducing rods at an angle of 30° to the perpendicular to the plane of the bone, which ensures an increase in the rigidity of fixation in the device by 1.7 times under axial load. With the help of instrumental reposition in the postoperative period, it is possible to eliminate minor displacements of bone fragments remaining after manual reposition.
In the postoperative period, additional immobilization was not required. Particular importance was attached to the rehabilitation treatment of patients after surgery. Passive movements in the operated joint were allowed from the first day after surgery, active movements - as the pain decreased - on the 3rd-4th day. To prevent thromboembolism, low molecular weight heparins and elastic bandaging of the lower extremities were used in the pre- and postoperative period. Patients with concomitant osteoporosis received complex treatment using calcium supplements, vitamin D3 and a group of bisphosphonates. Stability of fixation of the rod apparatus designed by A.I. Gorodnichenko, even in patients with osteoporosis, made it possible to develop movements in the operated joint in the coming days after surgery, which prevented the development of hypodynamic complications, contractures and deforming arthrosis.
Results and discussion
Consolidation of fractures was achieved in all cases. No secondary displacement of fragments was observed in the apparatus. The average fixation period was 13.9 weeks. Full weight bearing on the operated leg was allowed after 4-6 weeks for a periarticular fracture and after 12 weeks for an intra-articular fracture. Patients were discharged from the hospital on the 10-12th day after surgery. The device was dismantled on an outpatient basis or patients were hospitalized in the hospital for one day. Of the complications, in 5 cases there was inflammation of the soft tissues around the rods, which did not require repeated insertion of the rods, which was managed by the use of ultraviolet irradiation and local administration of antibiotic solutions. In our opinion, the complication that arose was associated with excess fat in obese patients, all of whom suffered from concomitant diabetes mellitus.
To illustrate the results obtained, we present a clinical observation.
Patient D.,
53 years old, was admitted to the hospital with complaints of pain in the right shin and right knee joint 2 hours after injury as a result of a road traffic accident. Transported by ambulance, the fracture was temporarily fixed with a ladder splint. On examination, swelling of the right knee joint and upper third of the leg, pain on palpation and a positive symptom of ballotation of the right patella are noted. After a clinical and radiological examination, a diagnosis was made: closed intra-articular transintercondylar fracture of the right tibia with displacement of fragments, type 41C1 (Fig. 1, I).
Figure 1. Radiographs of patient D. in frontal (a) and lateral (b) projections.
I - intra-articular transcondylar fracture of the right tibia with displacement of fragments, type 41C1. No vascular or neurological disorders were detected in the distal parts of the right lower limb. Upon admission, the fracture site was anesthetized, 60 ml of blood mixed with fat was obtained during puncture of the right knee joint, and external immobilization of the limb was performed with a plaster cast.
The next day, under anesthesia, an operation was performed: closed reduction and transosseous osteosynthesis of the right tibia using a rod apparatus designed by A.I. Gorodnichenko. Three spongy rods were inserted into the condyles of the tibia and three cortical rods into the diaphyseal part through skin and soft tissue incisions along the anterior inner surface of the right leg up to 8 mm long. After fixing the proximal rods in the device under the control of an electron-optical converter, closed reduction was performed using removable handles, followed by stabilization of the distal rods (Fig. 1, II).
Figure 1. Radiographs of patient D. in frontal (a) and lateral (b) projections. II - after osteosynthesis of the right tibia with a rod apparatus designed by A.I. Gorodnichenko. The skin around the rods is sutured with single sutures.
The postoperative course was without complications; regular dressings were performed with treatment of the skin around the rods with antiseptic solutions and changing of aseptic dressings. The sutures around the rods were removed 12 days after surgery, and the patient was discharged for outpatient treatment with recommendations for further rehabilitation treatment. After consolidation of the fracture, the device was dismantled 100 days later (Fig. 1, III).
Figure 1. Radiographs of patient D. in frontal (a) and lateral (b) projections. III - after consolidation of the fracture and dismantling of the device after 100 days. Movements in the right knee joint before dismantling the device from 0 to 140° (Fig. 2).
Figure 2. Appearance of patient D. before dismantling the device.
Conclusion
Our results of treatment of intra- and periarticular fractures of the knee joint bones using rod and pin-rod devices designed by A.I. Gorodnichenko allow us to speak about their high efficiency - the creation of stable osteosynthesis, which allows preserving the function of the damaged joint throughout the entire period of treatment, and the complete restoration of the patients’ ability to work. Complex treatment of patients in the older age group with concomitant osteoporosis should include the use of calcium, vitamin D3 and a group of bisphosphonates, which helps not only to increase the stability of osteosynthesis, but also to prevent the occurrence of new fractures of other locations. Due to the design features of external fixation devices and the simplicity of the surgical technique, this method is the method of choice in the treatment of intra- and periarticular fractures of the knee joint and can be recommended for widespread use in trauma hospitals.
Thus, treatment of intra- and periarticular fractures of the knee joint using A.I. Gorodnichenko, due to low trauma and short operation time, as well as high efficiency (creation of stable osteosynthesis), is the method of choice, especially in patients with concomitant osteoporosis.
Closed, atraumatic and reliable fixation of bone fragments allows patients to be mobilized earlier, improve their quality of life, reduce the duration of hospital treatment and minimize the possibility of hypodynamic complications, which, together with the repeated use of all components and parts of the device, is of great economic importance.
The method makes it possible not only to begin early restorative treatment of victims, maintaining the active motor function of the damaged joint from the first day after surgery and throughout the entire period of treatment, but also to improve the functional results of treatment for intra- and periarticular fractures of the knee joint.