A fracture of the humerus usually occurs when there is a sudden and strong load on one of the three bones of the shoulder. A clavicle fracture is the most common injury of this nature. There are 3 different bones in the shoulder area that can break: the collarbone, the proximal humerus, and the scapula. A fracture of the humerus usually occurs when a sudden force is applied. This happens, for example, in the event of a hard fall, an impact during sports, or an accident (for example, a car accident).
Closed and open fracture of the humerus
Closed fracture
A closed fracture can occur in the upper part of the shoulder. There, the head of the bone, the lesser and greater tuberosity, the surgical and anatomical neck are susceptible to injury.
The symptoms that concern a patient who has received a closed injury to this part are the following:
- Pain in the joint area.
- If the injury is impacted, then the swelling is not too pronounced and grows slowly. The pain intensifies when trying to actively move the limb. Passive movements are not too limited.
- If displacement is observed during a closed fracture, then deformation of the arm is more often visible, and other symptoms, including pain, appear more clearly.
If a closed fracture of the shoulder occurs in the middle section, then most often the cause is a fall or a blow to the shoulder. The injury can be splintered, oblique, transverse or helical. A fracture of this part often entails damage to the nerve bundle, namely the radial nerve. In addition, the brachial arteries and veins are affected.
The main symptoms that indicate a closed fracture of the humeral body include:
- Strong pain.
- Deformation, in the presence of displacement.
- Decreased limb length.
- Crepitation of fragments.
- Swelling and hematoma, which can occupy a wide area, up to the hand.
- Movements are limited mainly in the elbow and shoulder joint.
- If the nerves have been damaged, there is a disturbance in finger movements and sensitivity.
- The hand cannot be kept in a raised state; it hangs limply.
Open fracture
The main features of an open fracture include:
- An open wound will be visible on the surface of the skin. Most often there is bone visible through it.
- There is severe bleeding, which must be stopped by applying a tourniquet. Its location is the upper third of the shoulder.
- The wound site is treated with any available antiseptic, after which a sterile bandage is applied.
- Only after treatment and stopping the bleeding should the hand be immobilized.
Displaced humerus fracture
The following symptoms are typical for a displaced fracture:
- The occurrence of sharp pain that appears when trying to move the arm or when palpating the body of the humerus.
- Swelling, often with severe hematoma.
- Inability to perform active actions to abduct and raise the limb.
- With active palpation, crepitations are heard.
- The deformation is visible even when the bones have not broken through the soft tissue. Especially if the displacement of the fragments is pronounced.
The final diagnosis can be made only after the doctor sees x-rays, which must be taken in two projections. If there is a pronounced displacement of the humeral head, then the prognosis is unfavorable. Since it will experience a nutritional deficiency, this will lead to its death or even resorption. Fractures, the line of which passes through the tuberosities, are also dangerous. Restoring full function of the limb is rare.
When the surgical neck is injured, the displacement occurs in an impacted manner with the formation of a chip. The fragment may move to the side (when the fracture occurs with the shoulder adducted) or to the middle (with the shoulder abducted). In this case, the decisive factor in where it will be directed is played not only by the position of the shoulder when injured, but also by the muscle contraction that occurs reflexively.
It is important not to confuse a displaced fracture with a dislocated shoulder. A distinctive feature of such fractures is the ability to freely move the shoulder (not at the joint), using passive force. There will be no springing effect. These signs are especially relevant for obese people, since a dense fat layer can make it difficult to conduct a full X-ray examination.
Diagnostics
A preliminary diagnosis can be made based on the patient’s complaints, a history of a fall or blow, and examination data. To clarify the diagnosis, identify the nature of the fracture, and the position of bone fragments, an x-ray examination is performed. The picture is taken in several non-standard projections. In difficult situations, computed tomography is necessary.
This study makes it possible to accurately determine the nature of the damage in situations where the fragments on the radiograph are layered on top of each other, and it is technically impossible to perform the study in the desired projection due to limited mobility of the limb.
Non-displaced humerus fracture
If there is no displacement during the fracture of the shoulder bone, then the signs of the fracture may be somewhat blurred:
- Depending on the location of the injury, the person will feel pain in the upper or lower arm. But its intensity is not as pronounced as in a fracture with displacement of fragments. It intensifies when trying to move.
- Swelling may not form immediately, but over several hours. This is due to the fact that the soft tissue around the bone will not be damaged by fragments.
- A hematoma is observed, but it also appears after some time; its size and severity depend on the cause of the fracture.
- The shortening of the limb is not noticeable without special measurements.
- There is no hand deformity.
It is important to provide first aid to the victim correctly so that the fragments do not shift and the injury does not become more serious. More often, non-displaced fractures of the humerus are observed in children, which is due to the structural features of their bone tissue.
Forecast
If you see a doctor promptly, uncomplicated shoulder fractures give a positive prognosis. The function of the limbs is fully restored within 2-3 months after the impact.
The symptoms of a shoulder fracture that appear depend entirely on the severity of the injury and the location of the fracture. Treatment and rehabilitation will also depend on the presence of various kinds of complications, for example, limitation of limb movements, rupture of soft tissues, nerves, blood vessels or arteries, and the presence of infection in the bone. The video in this article will tell you how to recognize a shoulder fracture and how to provide first aid to the victim.
Fracture of the greater tuberosity of the humerus
Fractures of the greater tuberosity of the humerus are not uncommon. If it was damaged in isolation, then the injury occurs according to the avulsion type. Often the separation of the tubercle is accompanied by a dislocation of the shoulder. Due to the fact that the muscles responsible for shoulder abduction and rotation are attached to it, the torn fragment is always displaced due to their tension force.
Signs of avulsion of the greater tubercle are as follows:
- Swelling of the injury site.
- Pain that manifests itself locally above the shoulder joint.
- Impaired mobility of the shoulder joint.
- Due to muscle retraction, external rotation of the shoulder is impaired. This is one of the main symptoms indicating damage to the tubercle.
- If it is absolutely impossible to move your arm, then this is a sign of tendon damage.
After a fracture of the greater tuberosity, there is a danger that movement disorders in the shoulder joint may be severe. This is due to damage to the supraspinatus muscle. Sometimes there is no possibility of full recovery.
Removing pins
The pins are removed from the humerus after 8–9 months. The removal time is determined by the doctor based on radiographic studies. It is not recommended to skip this period, because osteosynthesis devices of the humerus may become overgrown with bone tissue. Leaving the structure inside is fraught with complications. A pin removed in time will not cause any trouble, leaving no scars or holes in the bone. Removing the pin after the recommended period may result in a serious operation.
Modern materials for osteosynthesis are biodegradable. They do not need to be removed; they dissolve inside the bone.
Other types of humerus fracture
Special mention should be made of surgical neck fractures, transcondylar and comminuted fractures. Each of them has certain characteristics. In treating them you need to adhere to certain tactics.
Surgical fracture of the humerus
If the mechanism of injury is indirect, the surgical neck of the shoulder often suffers. Fractures are divided into adduction and abduction, depending on the position of the arm at the time of injury. The first occurs if the limb is adducted, and the second if it is abducted. When the hand is in the middle position, then the distal fragment is inserted into the proximal one more often. This is called a surgical impacted fracture.
If we consider the symptoms of this type of injury, they are as follows:
- The pain will be localized at the fracture site and becomes more intense when trying to make circular movements.
- It is uncomfortable for a person to hold a limb in weight; he tries to support it under the elbow.
- If attempts are made to move, the greater tubercle will move towards the head.
- Swelling occurs and a hematoma is observed.
- When displaced, crepitations will be heard.
- Pathological mobility is observed.
- The shoulder will become shorter compared to a healthy one.
A surgical fracture of the humeral neck is dangerous because at the time of injury, the integrity of the neurovascular bundle often occurs. The same damage can occur with improper reduction. This violation will lead to the fact that the function of the hand will not be fully restored.
Transcondylar fracture of the humerus
Such injuries are rare, due to the location of the bone. The damage is considered intra-articular, which means that the fracture line runs through the joint cavity. It runs transversely, from one condyle towards the other.
Symptoms of transcondylar fractures include:
- Painful sensations that radiate to the elbow and forearm area.
- Presence of swelling. Sometimes the swelling is pronounced.
- If there is a displacement, then deformation of this area will be visible.
- When you try to feel it, you hear a crunching sound.
- Movements of the elbow, if not completely blocked, are then significantly limited.
A characteristic feature of a transcondylar fracture is trauma to the brachial artery. This increases the risk of gangrene of the hand. If the artery is damaged, you will not be able to feel the pulse in the forearm.
In order for both condyles to be broken, an impressive force must be applied. This could be a fall on an elbow from a height, or industrial accidents, for example, a mine collapse. X-rays often show fractures that form a V or T shape.
The external condyle breaks more often in children. The displacement will be directed outward and upward. The internal and external epicondyles are rarely affected and are accompanied by elbow dislocation.
Comminuted fracture of the humerus
The most severe of all types of shoulder fractures is a comminuted, displaced one. The difficulty is that not only the nerves are damaged, but also the blood vessels. Therefore, treatment necessarily requires surgical intervention.
This type of injury is typical for the adult population.
Depending on the nature and location of the fracture, the following types of comminuted shoulder injuries are distinguished:
- A fracture of the upper part is accompanied by swelling and deformation of the joint. For recovery, surgical intervention is necessary, an obstacle to which can be either advanced age or the presence of a serious illness.
- A fracture of the shoulder in the middle part is dangerous because fragments can damage the radial nerve, veins and arteries. To fix them, it is necessary to use metal pins or plates, or an Ilizarov apparatus.
- If the injury occurred in the lower part of the humerus and there is no displacement of the fragments, then it is advisable to apply a plaster cast. If the fragments are significantly displaced, surgery is necessary.
Anatomy
The humerus forms the upper part of the free limbs (arms). Anatomically, this bone originates from the shoulder joint and ends at the elbow joint. The humerus acts as a connection between the torso and the free limbs (arms). This department has a special structure that is responsible for a wide range of movements of the human hands.
The shoulder girdle is divided into two main bones:
- Spatula.
- Collarbone.
Table No. 1. The two main bones of the shoulder girdle are:
| Bone | Anatomical description |
| The bone has a flat triangle shape. Located behind the body, divided into three edges: lateral, superior, medial. Between the two shoulder blades there are three more angles: lower, upper, lateral. The last angle is distinguished by a thick structure with a glenoid cavity, which is necessary to connect the head of the humerus and the scapula. The neck of the scapula (narrowed place) is adjacent to this depression. Above the cavity there are 2 tubercles (supraarticular and subarticular). |
| This is a tubular bone with an S-shape. The collarbone is easily palpable, as it is located immediately under the skin. It is adjacent to the sternum at the medial angle, and to the scapula at the lateral angle. The collarbone is connected to the sternum by muscle tissue and ligaments. And it is connected to the scapula only thanks to ligaments, so when palpating you can observe roughness and protruding tubercles in the lower part of the clavicle. |
The humerus itself has a tubular structure, round in the upper part, and triangular in the lower part.
Divided into three departments:
- Head and surgical neck. The location of these parts is the joint capsule. They act as a component of the structure of the upper part of the shoulder joint.
- Shoulder body. In medicine, this section is called the diaphysis, has a rounded shape, and is the longest part of the humerus bone.
- Distal part (condylar). Due to this section, the forearm connects to the radius. Located in the lower forearm. Fractures in this place are called transcondylar; by the nature of the damage, these are intra-articular fractures.
Attention. Fractures of the humerus can be complicated by tears in the shoulder's nerves, brachial artery, and muscle tissue.
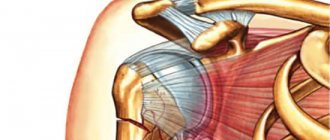
The photo shows the anatomical structure of the shoulder.
First aid for a fractured humerus
First aid for injury is as follows:
- First, you need to calm the person down and offer him a pain reliever. The following can be used as an analgesic: analgin, nimesulide, ketorol. If a person is experiencing panic, then you can give him a tincture of valerian, 20 drops will be enough, or one tablet of tazepam or triocasin. Valocordin or cordiamine can be used as a cardiovascular drug.
- Then you need to limit your hand movements as much as possible. For this purpose, immobilization is carried out. Small planks can be used as improvised means. One of them should be bandaged tightly to the shoulder, and the other to the forearm. If there are not even planks, then it is advisable to place your hand on a scarf. She throws herself over her uninjured shoulder. In this case, the arm should be bent at a right angle at the elbow. To prevent displacement, it is best to tie such a bandage as tightly as possible to the body.
- During transportation, it is advisable for the person to sit.
Treatment of a humerus fracture
Three methods are used to treat a shoulder fracture: surgical, conservative, and skeletal traction. If the fracture is not complicated by displacement or it can be corrected by performing a one-stage reduction, then applying a plaster cast or other fixing agent is sufficient.
If we consider therapy at the fracture site, we can highlight the following features:
- Treatment of a large tubercle occurs by applying a plaster cast; sometimes it can be supplemented with an abduction splint. This is necessary in order to prevent the development of stiffness in the joint and ensure proper fusion of the supraspinatus muscle. If the tubercle fragment has moved out of place, it must be fixed in the correct position with knitting needles or a screw. After about 1.5 months, the structure will be removed.
- If the surgical neck has been injured, but no displacement has occurred, then you can get by with a plaster cast for a month. When reduction was required, and it was successful, the cast will have to be worn for two more weeks. If it is not possible to straighten the bone fragments, then surgical intervention is necessary. Fixation inside the bone is carried out using plates. If the fracture is of the impacted type, then it is advisable to use either an abductor pillow or a special scarf. The treatment period can be extended up to 3 months.
- When the fracture is localized on the body of the shoulder and displacement is observed, the most common method of treatment was skeletal traction. A person will have to spend up to a month in an immobilized position. Afterwards, plaster will be applied for the same period of time. Recently, the method of skeletal traction has faded into the background; it has been replaced by osteosynthesis, which does not confine a person to bed for such a long period of time.
- Transcondylar fractures are almost always accompanied by displacement of fragments. Their comparison is carried out under anesthesia, and then it is advisable to apply a plaster cast for up to two months.
If vessels or nerves are damaged as a result of fractures, then a special operation is necessary, which involves placing sutures on them. This increases the treatment period and it is not always possible to fully restore the functionality of the limb. As for medications, it is advisable to use calcium supplements, as well as analgesics and antibiotics.
On topic: 12 folk methods for home treatment
Immobilization for a humerus fracture
When complete immobilization of the limb is required, it is advisable to apply a thoraco-brochial bandage.
The technique for applying it is as follows:
- The victim should sit on a high stool or on a table. His limb must be flexed 80 °C for an injury to the upper part of the shoulder and 45 °C for a fracture of the lower bones.
- A layer of cotton wool should be applied to the body, which is secured with bandages.
- The joints of the hand, such as the wrist, elbow and shoulder, are also covered with cotton wool.
- Plaster splints are applied horizontally to the body, and they are attached vertically to the sides.
- One splint should be placed over the shoulder that was injured. It should be attached to the body with bandages.
- Then additional splints are applied over the body, shoulder girdle, forearm, up to the hand. All this is again fixed with bandages.
- A special spacer is inserted between the arm that will be in the cast and the body so that the limb cannot adhere to the body.
This way the limb will be immobilized and bone fusion will proceed correctly.
Rehabilitation after a humerus fracture
After the bandage is removed, it is necessary to proceed to rehabilitation measures. They are an integral part of bone restoration and play no less important role than adequate therapy.
Rehabilitation necessarily includes:
- Physiotherapeutic treatment - you will need to complete several courses, which consist of 10 procedures. Electrophoresis with novocaine and calcium chloride may be recommended. Ultrasound treatment has proven itself well.
- A massage that, if it is impossible to visit a specialized office, can be performed independently. To speed up healing and stimulate blood circulation, you can use specialized ointments and oils.
- Performing a set of special exercises.
Rehabilitation period
After the pin is installed, a rehabilitation period begins. The patient should attend the dressing room regularly. For two months, dressing is carried out strictly in sterile hospital conditions. It is not recommended to carry it out at home during this period - there is a risk of getting an infection.
In addition, during dressing, an x-ray is taken, the doctor looks at the results of osteosynthesis. A physical therapy specialist prescribes limb development classes for the patient. Loads are necessary for the hand to function normally. Special exercises are used for development.