The metacarpals represent the bony framework of the palm and are important to the function of the hand, connecting the bones of the wrist and fingers. Bone fractures can affect hand grip strength and movement. They are the result of high-energy injuries such as direct impact, motor vehicle accidents, and work-related injuries. Although sometimes a pathological fracture occurs due to minor trauma or stress, when there is an oncological lesion of the bone structure. But, nevertheless, fractures of the metacarpal bones can often be treated conservatively with the help of reposition and proper immobilization, and have a favorable prognosis.
The metacarpal bones are part of the group of small tubular bones of the human body. They have a base, a body and a head. In this regard, fractures of the head, neck (subcapitate), body and base are possible. The most common fracture is a fracture of the neck of the fifth metacarpal (Boxer's fracture).
There are also rare specific fractures of the metacarpal bones, named after the author who first described this fracture. However, these fractures deserve special attention.
In particular, the Bennett fracture and the more severe Rolando fracture. These two fractures are accompanied by subluxation of the first metacarpal.
Bennett's fracture is an intra-articular fracture of the base of the first metacarpal bone with subluxation of the base. Essentially this is a fracture-dislocation. It was first described by the English trauma surgeon Bennet in 1882. A fracture of the base of the metacarpal bone through the joint along the axis, resulting in displacement and subluxation in the joint.
Rolando's fracture is a comminuted (3 fragments) intra-articular fracture of the base of the first metacarpal bone with subluxation of the base. The fracture occurs due to a strong blow to the axis of the finger. Fracture of the base of the metacarpal bone through the joint along the axis and also across. And on the radiograph it resembles the letter U or T. Subluxation in the joint also often occurs.
If these fractures are not treated, the finger remains deformed, and later arthrosis of the trapezio-metacarpal joint, pain and limitation of movements will occur.
Clinically Relevant Anatomy
Hand bones
The metacarpal bones are long, thin bones that are located between the wrist bones and the phalanges of the fingers.
- Each bone consists of a base, body and head.
- The proximal bases of the metacarpal bones articulate with the carpal bones.
- The distal heads of the metacarpal bones articulate with the proximal phalanges and form the knuckles.
- The 1st metacarpal bone is the thickest and shortest of these bones.
- The 3rd metacarpal bone is distinguished by a styloid process on the lateral side at its base.
- Soft tissues commonly injured in fractures include cartilage, joint capsule, ligaments, and fascia.
- In severe polytrauma, tendons and nerves adjacent to the fracture may also be damaged.
First aid to the victim
Some cases require first aid. Such injuries include open injuries with bleeding. The first step is to take measures to stop the bleeding and call an ambulance. Further hospitalization of the victim is carried out under the supervision of a traumatologist or other specialist.
With closed lesions, the injured arm must be immobilized to ensure that its mobility is limited. This is done in order not to accidentally touch the sore spot, and to avoid post-traumatic shock or loss of consciousness when damaged joints are displaced. The arm can be tied with any fabric available at hand. The main thing is that the fingers of the broken hand are bent.
Etiology
Metacarpal fractures (MCFs) typically occur secondary to a direct blow or a fall directly onto the hand.
- These fractures usually occur during sporting activities, especially contact sports. Almost a quarter of cases occur during sporting competitions.
- Sports injuries are a common cause among younger patients.
- Injuries related to physical work are a common cause in middle-aged patients.
- Falls are a common cause of fractures in older people.
- Bone fractures often occur after punching a wall or other hard object (hence the name “boxer's fracture”).
Possible consequences
Hollow bones can be very fragile due to a lack of nutrients that help strengthen them. Therefore, it is worth paying attention to this and taking appropriate measures. If necessary, you can consult a doctor.
In case of a fracture, you must immediately contact a specialist and, if possible, provide first aid to the victim if he needs it. If you take care of your health, you can avoid numerous problems and complications.
Incorrect treatment or poorly performed surgery can lead to disability. Therefore, you should not self-medicate, ignoring the doctor’s recommendations. After minor injuries, motor functions can be restored or a repeat operation can be performed. But in severe cases, the rehabilitation course may take several months, and the result may be negative.
With open wounds, complications often arise that begin with improper healing and pathological changes. In this case, there is a risk of infection, which often leads to rotting of bone tissue.
Difficulties during treatment may arise if the recommendations of the attending physician are not followed or clinical conditions are completely ignored.
Metacarpal fractures
- Typically occurs in patients aged 10-40 years.
- Men are more often affected than women.
- Young people get PPK bones when punching a wall or getting hit in the arm.
- Older women suffer these injuries secondary to low-energy falls.
- The incidence of fractures of each metacarpal increases from the radial to the ulnar side.
- The incidence of 2nd metacarpal fractures is lower than the incidence of 5th metacarpal fractures.
- Bennett's fracture is the most common fracture of the base of the thumb. This fracture is an intra-articular fracture and involves separation of the base of the 1st metacarpal bone in such a way that the part of the bone located closer to the ulna remains in its original position, and the other part is displaced outward.
PPK can be divided into three categories:
Types of Metacarpal Fractures
- A body fracture occurs when a person hits another person or object. In most cases, surgery is not necessary to treat this condition.
- Fractures of the metacarpal body often result from longitudinal compression, torsion, or direct impact. They are described by the appearance of the associated fractures and can be classified as transverse, oblique, spiral and comminuted.
- Fractures of the base of the metacarpal bone are rare and have minimal consequences because there is little movement of the joint. More common are fractures of the base of the fifth toe, which are the result of a longitudinally directed force.
How to identify an injury
The origin of fractures is very diverse, however, the signs indicating injury have similar properties. General signs of injury are expressed as follows:
- manifestation of acute pain in the affected area;
- the presence of a bluish or purple tint to the skin;
- significant swelling;
- with some injuries, internal bleeding occurs, forming a pronounced hematoma;
- if the bones of the foot are damaged, pain is felt when walking, which makes movement painful;
- There are cases when, with a strong blow, the bone undergoes severe deformation, and its head is difficult to feel.
Characteristics/Clinical picture
5th metacarpal fracture
Patients with metacarpal fractures typically have:
- Pain.
- Edema.
- Hematoma.
- Limitation of mobility.
- Deformation. Joint asymmetry may be observed; it may also appear that the joint is missing.
- Displacement of the fingers may also be noted.
- A fracture of the metacarpal head is associated with axial compression of the extended finger, which causes severe discomfort.
- When the base of the metacarpal bone is fractured, wrist movements or longitudinal compression increase pain.
- Any angulation of the ACC can lead to pseudoclaw deformity.
Possible complications
Even timely assistance does not exclude the occurrence of various complications after a fracture. These include:
- improper fusion of bones,
- limited movement of fingers and palms,
- the appearance of infectious lesions and suppuration (possibly due to untimely or improper treatment of an open wound during a fracture or during surgery).
A broken metacarpal bone may heal incorrectly if the cast is applied poorly or if the hand is already in a cast. As a result of this complication, frequent occurrence of pain in the area of injury, as well as limited movement, is possible. In such cases, doctors perform a deliberate fracture of the fused bone and its subsequent treatment.
Grade
The assessment includes:
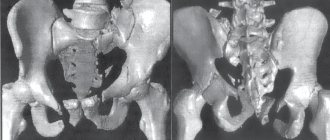
- Standard radiographs of the hand (antero-posterior, lateral and oblique). In the vast majority of cases, this will be enough to confirm the diagnosis and formulate a treatment plan. Confirmation of more subtle lesions can be obtained using specialist views such as Brewerton (metacarpal heads), Roberts and Betts (thumb).
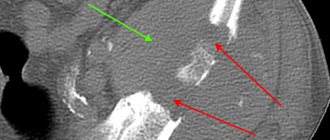
- A CT scan is sometimes necessary for base metacarpal fractures to rule out/confirm the presence of intra-articular displacement and determine whether surgery is necessary.
Diagnosis of injuries
To diagnose the condition of the injury, its characteristics and degree of complexity, specialists use the following methods.
- First of all, it is necessary to interview the patient, and then conduct a visual examination, take the necessary tests and determine the cause of the injury.
- Taking an x-ray. Photographs of the hand from both sides and from the side, depending on the location of the fracture.
- For multiple fractures with complications, computed tomography is necessary.
Typically, for experienced traumatologists, diagnosis is limited to a simple examination, and an x-ray is sufficient to confirm it.
Treatment
The goal of treatment is to restore the anatomy and function of the hand.
- Antibiotics and tetanus prophylaxis are treatment options for open fractures according to standard guidelines.
- Treatment will vary depending on the integrity of the skin (open or closed fracture), number of finger/metacarpal fractures, degree of bone fragmentation, displacement, rotation, etc.
- The general practitioner/specialist, after assessing the patient's condition, should perform gentle tests and imaging to determine whether surgery is required.
- If surgery is not required, a physical therapist will create a special splint that will keep the joint in the correct position while it heals.
Cervical injury
Damage to the metacarpal bones in the neck area occurs as a result of a sharp push. As a result, the head of the bone fits directly into its body without back cushioning. In this case, the bone itself does not move, but remains in place. Sometimes this condition may be considered normal, however, with a very strong blow, the bone can go deep into the cavity, which will noticeably shorten the finger.
If the fracture angle is slight, it can be treated without surgery, otherwise urgent surgery will be required. Leaving an injury untreated is not recommended, even if it is so small that it seems trivial. Over time, it will make itself felt: the consequences may be different, but restrictions on motor function and pain when trying to restore them are guaranteed.
Physical therapy
The goal of rehabilitation is to restore strength and full range of motion.
- For this purpose, hand exercises with light resistance are prescribed. This is where resistance bands and a ball can be helpful, especially if there is scarring and limited flexor motion develops.
- Soft tissue repair can be more challenging (compared to bone repair).
- Rest and elevation are important, as is splinting (poor splinting can lead to stiffness, pressure sores, or even compartment syndrome).
Friends, on July 17 in Moscow, as part of the #RehabTeam project, Anna Ovsyannikova’s seminar “Rehabilitation of the hand after a fracture of the distal radius (fracture of the “radius in a typical place”)” will take place.” Find out more... In addition, on July 18, she will conduct a seminar “Rehabilitation of the hand after fractures of the metacarpal bones (Boxer fracture).” Find out more...
Physical therapists use a range of techniques to restore movement in the hand, wrist and fingers. These include:
- Eliminate swelling with massage and compression clothing.
- Soft tissue massage helps relieve muscle tension and pain.
- Developing a home exercise program for patients with specific recommendations for movement and strengthening exercises.
Here are the steps to follow for a stable fracture (you can use this or another of the stabilization methods below):
- A non-operative treatment involves strapping the injured finger to another finger. This can be done with or without a splint.
- Splinting for a fracture should be as follows: wrist extension 20 degrees; flexion of the metacarpophalangeal joint by 60-70 degrees and extension of the interphalangeal joint.
- If we are dealing with a stable fracture, it makes sense to start movements earlier.
- As a rule, active exercises to increase the range of motion without resistance can begin 2-3 weeks after surgical treatment (on intact or adjacent joints).
- Active movement. If the fracture is fixed, an active increase in range of motion may begin earlier. Most fractures are treated with immobilization, but active motion can begin after three weeks of therapy, starting with joints not affected during the initial immobilization. This phase usually lasts 3-6 weeks.
- Active movements involve sliding of tendons.
- Tendon gliding is important to prevent adhesions, increase circulation, and reduce swelling and compression at the fracture site.
Tendon gliding exercises
Exercises for tendon gliding
- The claw hand exercise can be used to improve the glide of the extensor digitorum tendon over the metacarpal bones.
- An exercise to block the deep flexor digitorum to improve the sliding of its tendon along the phalanges.
- A hook fist position that promotes selective gliding of the flexor digitorum profundus tendon.
- An exercise to block the superficial flexor digitorum to improve the sliding of its tendons along the middle phalanges.
- A straight fist position that promotes selective gliding of the superficial digital flexor tendons.
Passive movements
- Passive movements can be started after sufficient clinical healing after approximately 5-6 weeks of therapy.
- The timing of the onset of joint mobilization depends on the structures involved in the injury. If structures resisting force are not involved in the injury, joint mobilization can be initiated at the same time as active movement. Compression from a fracture can result in shortening, angulation, or rotation of the bone.
- Traditional passive range of motion exercises are designed to help joint cartilage heal and reduce swelling and stiffness.
- Resistive movement. Four weeks after injury, light resistance can be performed (this is true for most PKCs that are treated with immobilization). Active movements should only be continued if healing has not yet begun.
- Resistance exercises should also be postponed while the fracture is being fixed with pins (until the pins are removed). Light resistance exercises help in scar remodeling and improve movement. There are several types of resistance exercises, such as weight training. This type of exercise strengthens the superficial and deep flexors of the fingers.
- Functional exercises and work simulations should be incorporated into resistance exercises as soon as possible.
Rehabilitation
The main task of the rehabilitation period is the fastest return to full functioning of the hand. The success of rehabilitation and its timing are very individual. They are determined by the following factors:
- type of injury;
- its location and type;
- the condition of the victim's body.
Rehabilitation effects are a complex that usually includes physiotherapy and physical therapy.
The patient must perform simple finger movements while still in a cast. After the immobilization is removed, exercise therapy begins in full. Exercises begin with those that are designed to work the wrist. The doctor selects specific exercises. Their complexity increases over time, up to one hundred percent recovery.
It’s also a good idea to include activities such as assembling and disassembling a children’s construction set (“Lego” will do), folding pictures from puzzles, and similar activities that involve subtle and precise movements of the hand.
This development of the arm will bring the return of full range of motion closer and will make it possible to speed up the return to work. Especially if your professional activity involves manual labor. For intra-articular and complicated fractures, much more time is spent on physical therapy.
From the arsenal of physiotherapy, the effect of a magnetic field accelerates the healing of bone tissue. 8–10 procedures are prescribed, dispensed every day. Mechanotherapeutic effects on the interphalangeal and wrist joints also help well.
The thumb of the right hand should be especially carefully developed, if, of course, it is the dominant one.
Preventive actions
To avoid injury, experts recommend following simple rules
- Observe safety precautions at work and at home.
- Be extremely careful when transporting heavy objects, playing sports, as well as under other circumstances associated with an increased risk of injury.
- Constantly monitor the condition of the musculoskeletal system, perform physical exercises that help strengthen bone tissue.
- Take vitamin complexes and minerals containing rich amounts of calcium.
Never perform any physical activities while intoxicated.