The upper limb girdle (shoulder girdle) is a set of bones and muscles that provide support and movement of the arms. It covers the area from the shoulder joint to the elbow. The bone structure consists of the clavicle, shoulder blades and humerus, followed by the forearm and hand.
The bones of the shoulder girdle connect the acormioclavicular joints (the bony connection between the acromion and the collarbone). The shoulder girdle is attached to the skeleton using the sternoclavicular joints, muscles and ligaments that hold the scapula and upper limb.
Shoulder injuries are common, especially among professional athletes and people who do heavy physical work with their hands. Pathologies are manifested by pain, crepitus, and deformation. Conservative treatment is usually carried out, but in severe cases surgery is necessary.
Shoulder anatomy
Not all people know how many bones make up the shoulder girdle. The skeleton of the upper limb girdle is formed by the following bones: 2 shoulder blades, 2 clavicles, humerus.
The scapula is a triangle-shaped bone that is located on the back surface of the body. The clavicle is a paired bone that is curved along its long axis in the shape of the letter S. It is located horizontally along the front and upper surface of the body. The shoulder girdle includes the humerus.
A diagram of the bones of the shoulder girdle is presented below.
Bones of the shoulder girdle
Some people are interested in the question of what type of bones of the upper limb girdle are. The scapula is a flat bone, while the clavicle and humerus are tubular.
The ligamentous apparatus of the shoulder consists of the acromioclavicular joint and the shoulder joint. The acromioclavicular joint is strengthened by the coracoclavicular ligament. The scapula is supported by the coracoacromial and superior transverse ligaments. The shoulder joint is strengthened by the coracobrachial ligament, as well as the fibers of the supraspinatus, infraspinatus, subscapularis, and teres minor muscles.
Thanks to the muscles, tendons and ligaments, the upper limb has the correct position, it is strengthened and is capable of performing a variety of movements.
The muscles of the shoulder girdle include: motors, coordinators, stabilizers of the scapula. The motor muscles include the deltoid, latissimus dorsi, and pectoralis major. They are involved in performing basic arm movements (extension, adduction, abduction, rotation). The group of coordinating muscles may include: subscapularis, supraspinatus, infraspinatus, teres minor. They are necessary to ensure that movements in the shoulder are coordinated. Scapula stabilizers include the trapezius, rhomboid major, rhomboid minor, serratus anterior, pectoralis minor, and levator scapulae muscles. They regulate the movement of the shoulder blades.
Weak spots
Where the capsule is attached to the radius, its inner surface forms a depression - a sac-like bag, which is directed downward. Here the articular membrane becomes thinner. It is the weak point of the elbow joint. When it becomes inflamed, purulent discharge accumulates in the bag. If it ruptures, the destructive process can penetrate into other tissues, for example, into the fatty tissue of the forearm.
In addition to the ligamentous apparatus, the joint is also strengthened by muscles. But behind and above the capsule, on the sides of the process of the ulna, it is not strengthened by any muscles. This area is the second weak point.
Structure and functions of the clavicle
The clavicle is the only bone in the human body that connects the skeleton to the upper limb. Tubular bone mainly consists of spongy substance. It has a horizontal position and runs along the upper edge of the chest. The clavicle consists of a body and 2 ends:
- The medial (sternal) end connects to the sternum.
- Lateral (acromial) faces the collarbone.
The clavicle consists of a body and 2 ends
The medial end, like the sternum, has a convex curve forward, and its other part is curved backward. The middle part of the bone is slightly compressed from top to bottom. On its lower surface there is an opening through which blood vessels and nerves pass. On the lower surface of the medial end there is a depression to which the ligament connecting the clavicle and the cartilage of the first rib is attached. At the humeral end there is a cone-shaped tubercle and a trapezoidal line. Closer to the lateral end of the lower surface of the body of the clavicle there is a recess for the attachment of the subclavian muscle.
The front and top parts of the bone are smooth, and the lower surfaces to which the muscles and ligaments are attached have roughness in the form of tubercles and lines. On the inner surface of the thick medial end there is a large oval joint - this is the junction of the clavicle with the sternum. The lateral end is wider than the medial end, but not as thick. Above its lower surface is the acromioclavicular joint, which connects the collarbone to the bony outgrowth of the scapula (acromion).
The bony joints of the acromioclavicular joint are oblique, flat, and elliptical in shape. There is a dense fibrous membrane around it, which is strengthened by ligaments. The sternoclavicular joint is also surrounded by a wide fibrous membrane and 3 powerful ligaments. This joint is involved in movements along axes that are perpendicular to each other.
The collarbone performs a supporting function, since the scapula and arm are attached to it. In addition, the bone connects the upper limb to the skeleton, providing it with a wide range of movements. Together with the scapula and muscles, the clavicle transmits forces that affect the arms and the rest of the skeleton. In addition, the bone protects blood, lymphatic vessels, and nerves that are located between the neck and upper limb from pinching.
Rib cage
Its frame is formed by twelve pairs of ribs, thoracic vertebrae and sternum. Unlike animals, the human chest is much wider (laterally) and longer. This is due to the appearance of upright walking - relying only on the legs. Changing the position of the internal organs to vertical ensured straightening and increasing the volume of the chest.
The presence of a heart and lungs inside it obliges this formation to be strong and at the same time elastic. This is ensured by long and relatively soft ribs, as well as a large number of joints.
- At the back, the ribs are loosely fixed between two adjacent vertebrae, which allows them to rotate up and down when breathing.
- In front, they are connected to the sternum through synchondrosis, a sedentary cartilaginous connection.
Clavicle injuries
As you can see, the collarbone performs important functions, but it bears a large load, so it is susceptible to various injuries:
Dislocation of the acromial end of the clavicle with ligament rupture
- Fracture. In most cases, the fracture occurs in the middle of the bone body. There is a left and right clavicle, usually one of them is injured, a bilateral fracture rarely occurs. A fracture most often occurs when a person falls on their arm or receives a direct blow. There is a risk of injury to the fetus' collarbone as it passes through the birth canal. After a fracture of the collarbone, the arm lengthens, the limb in the collarbone area becomes deformed, and the victim cannot lift it.
- Dislocation of the acromial end. The articular surfaces are displaced after a fall on the shoulder. Features of the injury: after the impact, the scapula is pushed down, the collarbone is not so mobile, so it does not move behind it, as a result, the ligaments connecting the bones are torn, and the acromioclavicular joint is dislocated. The injury is manifested by elongation of the arm, swelling and deformation. When you press on the collarbone, it falls into place; after the pressure stops, it rises again.
- Osteolysis of the clavicle. This is a rare disease characterized by complete destruction (resorption) of bone without replacement by other tissue. The exact causes of the pathology are not known, but doctors suggest that it is associated with autoimmune diseases of bone tissue. The only symptom is slowly healing fractures.
If a clavicle injury is suspected, MSCT (multispiral computed tomography) is prescribed - this is a modern study that uses X-rays and conducts a multi-slice scan of the clavicle. Multislice CT allows for qualitative and detailed examination of morphological changes in bones and surrounding tissues.
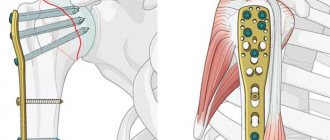
For ordinary clavicle fractures, conservative treatment is carried out, and the patient is given a fixing bandage. If fragments are displaced and soft tissue is damaged, surgery is performed, and bone fragments are connected using special plates, knitting needles or rings. The rehabilitation period plays an important role, when the patient is taught to move the injured arm again.
Anatomical structure and functions of the scapula
A paired triangular bone is located on the back surface of the body on both sides of the spine. Its base is at the top and the pointed end is at the bottom. It is a flat, wide bone that is slightly curved backwards.
The scapula is a paired triangular bone
The scapula consists of an anterior (costal) and posterior (dorsal) surface.
Anatomy of the posterior part of the scapula:
- The spine is a protruding plate of bone that crosses ¼ of the bone and separates the supra- and infraspinatus fossae.
- The acromion process is an elongated, triangular-shaped process at the top of the bone that ends at the spine.
- The coracoid process is the hamate bone. Which is located between the upper edge, the neck of the scapula.
- The neck is the slight narrowing that separates the rest of the scapula from the outer corner.
- Body of the scapula.
- Inner edge of the shoulder blade.
- External corner.
The structure of the scapula in front is simple; it has a wide fossa to which the subscapularis muscle is attached. The inside of the cavity is covered with ridges to which tendons and muscle fibers are attached. In the upper part of the socket there is a transverse depression where the scapula bends along a line that runs at an angle of 90° through the middle of the glenoid fossa, which includes the head of the humerus.
There are 3 angles:
- The superior angle is formed by the superior and medial borders of the bone. It is thin, has a smooth surface and a rounded shape, and fibers of the muscle that elevate the scapula are attached to it.
- Lower. The lateral border of the scapula forms a lower angle with the medial border. This is the lowest thick section of bone with a rough texture. The teres major and several fibers of the latissimus dorsi muscle are attached to it posteriorly.
- Lateral. This is the thickest part of the scapula and contains the articular socket that connects to the humerus. At the apex of the lateral angle is the supraglenoid tuberosity, to which the head of the biceps is attached.
There are 3 edges of the scapula:
- The top one is considered the thinnest and shortest. It has a concave shape, occupies the area from the upper angle to the coracoid process.
- Lateral - the thickest edge of the scapula. It starts from the lower edge of the articular socket, passes down and back to the lower corner of the bone.
- The medial edge is the longest edge, which occupies the area from the upper to the lower corner of the bone.
Thanks to the articulations, the scapula connects the humerus and collarbone, providing mobility to the upper limb. The paired bone protects important organs and blood vessels from damage. And also the scapula, together with the muscles, performs a motor function, it allows you to rotate, abduct (to the side, back, forward), and understand the arms.
Development
When a child is born, the shoulder joint is not fully formed, its bones are separated. After the birth of a child, the formation and development of shoulder structures continues, which takes about three years. During the first year of life, the cartilaginous plate grows, the articular cavity is formed, the capsule contracts and thickens, and the ligaments surrounding it strengthen and grow. As a result, the joint is strengthened and fixed, reducing the risk of injury.
Over the next two years, the articulation segments increase in size and take on their final shape. The humerus is the least susceptible to metamorphosis, since even before birth the head has a rounded shape and is almost completely formed.
Pathologies of the scapula
When the scapula is injured, the quality of life decreases; people are not able to care for themselves or perform physical work. The shoulder blades can be damaged by a fall on your back, shoulder or arm, a direct blow, an accident, or a work-related injury.
There is a possibility of bone fracture in the following areas: neck, glenoid, spine, coracoid process, acromion, superior or inferior angle. And longitudinal, transverse or multi-fragmented damage is also possible.
When a fracture occurs, the “Comolli triangle” appears - this is a swelling in the shape of a triangle. On palpation, the pain in the damaged area intensifies. A displaced fracture is accompanied by a crunching sound from bone fragments. In case of intra-articular injury, the shoulder and arm are raised. Blood accumulates in the cavity of the bone connection, so the size of the shoulder increases. When the neck is damaged, the shoulder drops slightly, the acromion protrudes forward, and the coracoid process moves slightly back. With an open fracture, a wound appears through which bone fragments are visible.
Dislocation of the scapula is a rare occurrence. The injury occurs if a person makes a strong jerk with his arm or shoulder, as a result, the bone is displaced. After a dislocation, the coracoid process of the scapula protrudes through the skin, causing sharp pain that intensifies with movement.
Bursitis is an inflammation of the synovial (periarticular) bursae of the shoulder joint. Typically, the disease develops against the background of infection, injury, or an autoimmune disease. With bursitis, pain occurs, the damaged area turns red, swells, a feeling of numbness appears, and it is difficult for the victim to move his arm.
Multi-slice computed tomography will help detect scapular pathologies.
For ordinary fractures, a special splint is placed on the arm on the damaged side, which must be worn for 4 weeks. Then physiotherapy and massage are prescribed, the patient must develop the limb with the help of special exercises. For intra-articular injuries, surgery is indicated.
Bursitis is treated with the use of NSAIDs, steroid hormones, antibacterial agents, analgesics, chondroprotectors, and vitamin-mineral complexes.
Anatomy of the humerus
The humerus is a wide, long tubular structure. It is part of the movable upper limb, unites the ulna, radius, and hand with the human skeleton. Around the humerus there are muscles, nerve trunks, and lymphatic vessels.
Brachial bone
The shoulder structure has the following structure:
- The body of the bone (diaphysis), which is located between the epiphyses.
- Metaphysis is the section of bone that is adjacent to the epiphyseal plate.
- Epiphysis – upper proximal, lower distal end of the structure.
- Apophysis is a process of bone next to the epiphysis, to which muscle fibers are attached.
At the proximal end of the humerus is the smooth round head of the humerus, the articular cavity of the scapula, which form the shoulder joint. Next comes the anatomical neck - this is a narrow groove between the head and the body of the shoulder. Just below the neck there are 2 muscle tubercles (large and small), to which the rotator cuff muscles are attached. Under the tubercles it narrows again, forming a body. On its outer part, almost in the middle, there is a deltoid tuberosity, to which the fibers of the muscle of the same name are attached. On its posterior edge there is a groove of the radial nerve in the form of a flat, gentle groove.
The lower edge of the bone is wide, bent anteriorly, muscle fibers are attached to it, and it also participates in the structure of the elbow joint. The joint consists of the condyle of the humeral structure with the bones of the forearm. The inner edge of the condyle is the block of the humerus that connects to the ulnar structure. The head of the condyle, together with the radial structure, forms the humeroradial articulation. Above the condylar head is the radial fossa. On both sides of the trochlea are the ulnar and coronoid fossa. The humerus has lateral and medial epicondyles (rough convexities) on the outside and inside. On the surface of the medial process there is a groove with the ulnar nerve trunk.
The functions of the humerus, despite its simple structure, are important. It increases the swing when a person moves his arm. This structure helps maintain balance when the center of gravity shifts during walking. It helps determine the correct support of a person on the upper limbs in various specific body positions (for example, while climbing stairs).
Lower limb
Starts from the groin folds and ends at the fingertips. The leg has three sections: the thigh, shin and foot. Their joints are the largest in the body.
The basis for the leg is formed by the hip joint, which is formed by the large head of the femur and the acetabulum of the pelvis. The recess provides almost complete coverage of the head, which causes rare dislocations of this joint. Additionally, it is strengthened by powerful ligaments both outside and inside.
The knee is formed by the condyles of the femur, the articular surface of the tibia and the patella. To create stability, there are two cartilage plates - menisci. Maintaining integrity is provided by many ligaments inside and outside the knee. It is supporting in function, and therefore is inactive - only flexion and extension are carried out.
The ankle joint is shaped like a fork formed by the bones of the lower leg and foot. This structure is necessary for normal support of the leg - when standing, under body pressure, these formations firmly hold each other.
A noteworthy joint in the human body is the elbow joint, which connects the shoulder and forearm. The joint is formed by 3 bones: the ulna, humerus and radius.
Shoulder injuries
Shoulder dislocation is a common occurrence that is associated with arm mobility. The displacement can be anterior, posterior, or inferior. When a dislocation occurs, the mobility of the limb is limited, pain and swelling appear. When the nerve is compressed, a feeling of numbness occurs.
A fracture most often occurs from a direct blow to the shoulder, falling backwards onto the elbows, or falling forward onto the arms. Typically, the integrity of bones is compromised in weak areas:
- Anatomical and surgical neck of the humerus.
- The area near the condyles.
- The area near the head of the humerus.
- The middle of the bone.
The injury is manifested by severe pain and impaired mobility. After some time, the shoulder swells, hematomas appear, and the damaged area becomes deformed.
Osteomyelitis is a purulent inflammation of the bone due to the penetration of microbes into the bone marrow through the blood. This disease is common because the humerus is abundantly supplied with blood. The pathological process provokes the destruction of bone tissue, as a result, fractures form without significant external influence.
Reference. Among the commonly diagnosed pathologies of the humerus are arthritis (inflammation of the joint).
Pseudarthrosis is also a common pathology. Not all patients know what it is. This is an abnormally formed joint that appears at the site of a non-union fracture of the humerus. With pathology, the functionality of the hand is impaired, but there is no pain.
Palpation and visual inspection can identify injuries and diseases of the humerus. X-rays can help differentiate a fracture from a dislocation. MRI and multi-slice computed tomography can detect malignant tumors. A multislice tomograph will help to examine the bone structure in detail and determine pathological changes.
When a dislocation occurs, a health care worker gives the victim a painkiller, compares the fragments of the joint, and then immobilizes the limb. Simple fractures are also treated conservatively. If the bone fragments are displaced, then surgery is necessary. The bone fragments are connected using knitting needles or screws, and then a Turner plaster splint is applied. If necessary, skeletal traction is performed first.
Exercise therapy will help develop the shoulder joint for flexibility. During rehabilitation, mechanotherapy and physiotherapy are indicated.
Blood supply
The blood supply to the structure is carried out using an extensive network of arteries, through which nutrients and oxygen enter the joint tissues. Veins are responsible for removing waste products. In addition to the main blood flow, there are two auxiliary vascular circles: the scapular and the acromiodeltoid. The risk of rupture of large arteries passing near the joint significantly increases the risk of injury.
Blood supply system of the shoulder joint
Elements of blood supply
arteries:
- suprascapular
- front
- back
- thoracoacromial
- subscapularis
veins:
- humeral
- axillary
The most important
Now you know which bones form the shoulder girdle. The shoulder blades, collarbone and humerus take part in the formation of important joints, and thanks to muscles and ligaments, they provide mobility of the upper limb. Fractures of the clavicle and humerus occur more often than injuries to the scapula. This is due to the fact that the scapula is a fairly strong bone, which is protected by a thick layer of muscle. After identifying an injury, the affected limb is immobilized, and in case of complex fractures, an operation is performed to compare bone fragments. Therapeutic gymnastics and physiotherapy will help speed up recovery.