Damage to the ankle ligaments occurs as a result of injury - a twisted foot, often during sports or in winter, when there is ice. Pain may not occur immediately. After a short time or immediately after the injury, swelling of the ankle joint appears, its contours are smoothed out, and subcutaneous hematomas (bruises) appear. Sometimes patients o at the time of injury. Movement in the ankle joint causes acute pain; it is almost impossible to lean on the leg. You need to apply cold and immobilize the damaged joint, then go to a medical facility where you will have an x-ray of the ankle joint. Often this is not enough and a number of additional examinations may be required, such as ultrasound examination of the joint, magnetic resonance imaging (MRI) to assess the condition of the soft tissue structures (ligaments, tendons) of the ankle joint.
Symptoms of rupture/damage to the ligamentous apparatus of the fingers
Common signs of ligamentous injury include:
- Soreness.
- Limited swelling.
- Passive mobility of the joint in a non-standard direction.
In some cases, the fingers become spindle-shaped. This defect may persist for several months.
When the interphalangeal ligaments are damaged, patients complain of severe pain, weakness in the joint, discomfort when moving, and swelling. If the ligament is completely torn, the finger may become hyperextended. In case of injuries to the dorsum of the hand, the extension function of the fingers (one or more) is impaired. If the nerves are damaged, the fingers may become numb. Other sensory disturbances also occur. Hemorrhages may also occur.
Diagnosis of rupture/damage to the ligamentous apparatus of the fingers in the clinic
Diagnosis of injuries to the ligamentous apparatus of the fingers begins with a simple examination and questioning of the patient. The doctor performs a visual inspection. He determines the type of damage by palpation (palpation of the hand). Additionally, instrumental examination methods are prescribed.
Our doctors have the necessary skills and knowledge for quick and high-quality diagnosis and diagnosis. We can conduct examinations using modern, high-precision, expert-class equipment from the world's leading brands. Diagnosis will take a minimum of time, and the doctor will be able to begin treatment immediately.
The problem of ununited fractures and false joints of long bones still occupies a large place in scientific research. Despite known advances in the treatment of patients in this group, the results leave much to be desired.
According to the literature, this complication occurs after treatment of open fractures in 8% to 35% of cases; after closed fractures, nonunion occurs in 5% to 11%.
The reasons for such a high incidence of complications of bone fractures most often come down to defects in local treatment - inaccurate reposition of fragments, short-term or unstable immobilization, incorrect choice of method for fixing fragments and performing an osteosynthesis operation, suppuration of the fracture site complicated by chronic postoperative osteomyelitis. In open fractures, nonunion may be associated with the nature of the injury - extensive crushing of soft tissues, vessels and nerves, infectious complications and the development of post-traumatic osteomyelitis.
The main methods of treating false joints remain various types of surgical treatment, well developed in recent years: stable intraosseous osteosynthesis, autologous bone grafting, compression-distraction osteosynthesis with the Ilizarov apparatus, external metal osteosynthesis in combination with autologous bone grafting. But, despite all the methods of surgical treatment used, in the future (with this pathology) a longer period of external immobilization is required, compared to fractures.
The main disadvantages of the widely used plaster cast include: heavy weight; fragility during use, especially under load (bandages on the lower limb); contamination of the dressing both outside and inside with skin secretions; When water gets on the bandage, it gets wet and loses all its fixing qualities. All this requires repeated dressing changes during long periods of treatment.
Custom orthoses made of thermoplastic for the upper and lower extremities must meet the following requirements:
- when using them, fixation and dynamic correction of damaged segments should be carried out in a functionally correct position;
- partial unloading of the damaged segment with transfer of the load to healthy areas of the body to allow restoration of limb function;
- hygiene (it must be possible to sanitize the product);
- aesthetics (the orthosis should be light, durable and, if possible, not protruding from under clothing);
- the possibility of early rehabilitation of the patient using an orthosis.
For this purpose, the following types of products have been developed and introduced into clinical practice at our enterprise:
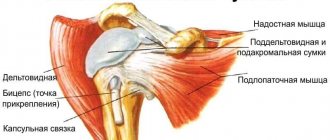
Shoulder splint
It is used after fractures in the area of the shoulder joint and the upper third of the diaphysis of the humerus, during periods of instability; with traumatic lesions of the ligamentous-capsular apparatus; with humeroscapular periarthritis; after operations on the ligamentous apparatus of the shoulder joint.
Splint for the elbow joint
Used for immobilization of false joints of the upper third of the forearm and after surgical interventions on the elbow joint; for inflammatory and degenerative diseases of the elbow joint, as well as for paresis of the muscles of the forearm.
Tutor for the whole hand
Prescribed for false joints of the forearm; for immobilization of the elbow joint after surgery; with paresis of the muscles of the upper limb to give it a functional position; for inflammatory and degenerative diseases of the elbow joint.
Arm device with a hinge in the elbow joint
Used for immobilization of fractures and false joints in the middle and lower third of the diaphysis of the humerus, as well as the upper third of the forearm; after surgical interventions on the elbow joint in order to prevent deformities, stiffness and early activation; for inflammatory and degenerative diseases of the elbow joint, as well as for paresis of the muscles of the forearm.
Clinical example:
Patient Sh., 46 years old. D.Z.: Floppy consolidating comminuted fracture of the humerus
Radiographs of patient Sh. before using the device
Radiographs of patient Sh. after using the device
Appearance of patient Sh. in the apparatus and range of motion in the elbow joint
Abduction splint on the arm with a semi-corset
It is used for fractures of the surgical neck of the shoulder and fractures of the articular surface of the scapula to improve the development of movements in the shoulder joint in the post-immobilization period (makes it possible to wear outer clothing).
Splint for the wrist joint
It is used in patients with flaccid consolidating fractures of the forearm bones in the lower third and metacarpal bones; with inflammatory and degenerative diseases of the wrist joint; in patients with radial or ulnar deviation.
Splint for rigid fixation of the hip joint with a semi-corset
Prescribed for immobilization of the pelvis and hip joint in a certain position, during the period of consolidation of fractures in the hip joint area and the upper third of the thigh, in case of instability of the joint after endoprosthetics.
Splint for rigid fixation of the hip and knee joints with a semi-corset
Prescribed for immobilization of fractures and false joints of the middle and lower third of the femur; for inflammatory and oncological diseases of the hip joint, pelvis and thigh.
Clinical example:
Patient B., 14 years old. D.Z.: Condition after resection and autoplasty of the femur, pseudarthrosis in the third part of the graft.
Before using the orthosis, the patient was in bed rest. After making an orthosis from a polymer material, the patient was taught to walk with the help of a cane; the shortening of the lower limb was compensated by special orthopedic shoes.
Splint for rigid fixation of the knee joint
It is used during the rehabilitation period after injuries and operations in the area of the distal femur and proximal bones of the leg, for injuries of the capsular-ligamentous apparatus of the knee joint, hemarthrosis, arthrosis-arthritis, bursitis, synovitis, meniscitis, as well as for moderate valgus and varus deviation of the leg , with recurvation of the knee joint and paralysis of the muscles of the lower limb of various etiologies.
The splint provides immobilization of the knee joint with fixation of 2/3 of the thigh and 2/3 of the lower leg. If necessary, it is reinforced with metal bars, and the fastening system allows you to create the required degree of compression.
The product is not indicated if it is impossible to load the lower limb, as well as with local dermatitis, pustular infection and fixed flexion contractures of the knee joint.
Splint for rigid fixation on the entire leg and unloading under the tube
It is prescribed for flaccid consolidating fractures and false joints of the upper and middle third of the leg, as well as the lower third of the thigh, for inflammatory diseases of the knee joint, for flaccid and spastic paralysis of the lower extremities, and for a tendency to flexion contracture of the knee joint.
Clinical example:
Patient G., 23 years old.
D.Z.: Pseudarthrosis at the border of the middle and lower third of the thigh, chronic post-traumatic osteomyelitis. X-ray before immobilization.
X-ray 2 months after the start of immobilization
Ankle splint
It is used after fractures of the ankle joint and lower third of the leg when their consolidation is delayed; in case of damage to the ligamentous apparatus of the ankle joint; for arthritis of various etiologies; for destructive diseases of the ankle joint.
Clinical example:
Patient D., 56 years old.
D.Z.: Floppy consolidating fracture of the lower third of the leg. He has been ill for about 1.5 years. The patient has been walking all this time with the help of crutches without putting any weight on his sore leg. After making an individual orthosis, the patient is taught to walk without additional support.
Protective and unloading shin splint
Indicated for delayed consolidation and false joints of the upper third and middle third of the tibia, as well as after operations on the bones of the lower leg. Provides external fixation of the lower leg for the purpose of immobilization and creating the possibility of axial load on the limb.
Clinical example:
Patient B., 46 years old.
D.Z.: Pseudarthrosis of the upper third of the tibia, chronic post-traumatic osteomyelitis, fistulous form. Diabetes mellitus He has been ill for about 2 years, during which time he has undergone several osteosynthesis operations without a positive result. When presenting, the patient walks with the help of crutches. The patient was given an individual orthosis and taught to walk without additional support.
Full leg device with knee joint
Prescribed to patients with widespread paralysis or paresis of the muscles of the lower limb; after plastic surgery of the muscles of the knee joint; during recurvation of the knee joint, as well as for unloading and fixing the correct position of the lower limb.
Clinical example:
Patient E., 16 years old. D.Z.: Residual effects of cerebral palsy. Spastic adduction contractures of both legs. In the apparatus, contractures were eliminated, the patient was taught to walk without additional supports
Conclusions:
1. Modern materials and vacuum molding technology make it possible, through individual modeling of products, to bring their configuration as close as possible to the anatomical shape of a body segment and to ensure adequate immobilization of the pseudarthrosis site due to precise anatomical and physiological adaptation to the patient’s body, which makes it possible to carry out early loading of the damaged limbs. The weight of such a bandage is 10 times lighter than its plaster counterpart, which facilitates the functional use and social activity of the patient.
2. The necessary orthopedic products are manufactured within a period of a week to several hours.
3. The use of thermoplastic in traumatology and orthopedics makes it possible to fundamentally change the method of conservative treatment and rehabilitation of patients in the postoperative period. The manufactured orthosis allows, in the stages before consolidation of the fracture, to return the lost function to the limbs. For disabled people with deformities of the musculoskeletal system, dynamic correction should be carried out during treatment in the same orthosis, taking into account the restoration of lost function.
4. The service life of a polymer product is many times longer than the service life of a plaster bandage, it is more hygienic due to the ability to remove the bandage and carry out hygiene procedures, and is less susceptible to mechanical damage under load.
The article was published in the journal “Bulletin of Prosthetists and Orthopedists”, No. 2(8), 2002.
Examination methods
The main examination methods include:
- Ultrasound. An ultrasound examination allows you to assess the condition of the hand and determine the functionality of tendons and ligaments. Examining the hand, the doctor determines damage to the nerve threads, pinching, and small bone fractures that are not visualized on x-rays.
- X-ray examination in frontal and lateral projection. This examination is aimed at clarifying the type of injury. It also allows you to confirm or refute a bone fracture. Also, an x-ray can reveal the degree of injury to hard tissues that are located next to the ligamentous apparatus.
- MRI (magnetic resonance imaging). This survey is accurate and informative. It may be prescribed to clarify the diagnosis.
Examination methods are chosen by the doctor.
Knee meniscus tear.
The meniscus is a crescent-shaped cartilage-like pad inside the knee joint. Its function is load absorption, joint stabilization, and sensitive function. The menisci are located on the surface of the tibia on the outside of the joint (lateral meniscus) and on the inside (medial meniscus).
Meniscal injury is the most common knee
. Its ruptures can occur during rotational movements in the knee joint or during sharp bending and sharp straightening of the leg.
The types of ruptures are quite varied. The meniscus can delaminate, tear lengthwise or crosswise, or there can be a combination of injuries. The torn part of the meniscus can move during movement and block the knee joint. The constant movement of the meniscus fragment causes clicking and crunching in the joint, accompanied by shooting pain. With stable ruptures without displacement of the fragment, the pain in the joint is constant aching, increasing with physical activity.
A meniscus tear can be suspected based on patient complaints, injury history and clinical examination, identifying positive symptoms and tests when examining the knee joint. However, the diagnosis should be confirmed by magnetic resonance imaging data. Indications for surgery are determined taking into account an MRI study, which visualizes the nature and type of meniscus damage and the location of the tear.
Recently, the main method of surgical treatment of meniscus tears is arthroscopy. Open operations are too traumatic and do not bring the desired result. During arthroscopic surgery, 2-3 5mm punctures are made in the area of the knee joint. A camera and mini-instruments are inserted into the joint cavity to treat the meniscus. Depending on the nature of the damage, the damaged part of the meniscus is resected (partially excised) or, if possible, sutured.
In the postoperative period, the patient can immediately step on his leg during resection of the meniscus, or he is prescribed walking with crutches without supporting the leg when the meniscus is sutured. The timing of load limitation is prescribed immediately after the intervention and depends on the operation performed, the nature of the meniscal damage, the patient’s activity, his age and possible concomitant injuries in the joint.
Make an appointment
Treatment of rupture/damage to the ligamentous apparatus of the fingers in the clinic
When the ligaments of the hand apparatus are torn, treatment can be either conservative or surgical.
Usually a plaster splint is placed on the arm for 2-3 weeks. It allows you to fix the hand in a functionally and anatomically correct position. The patient is then observed. If, after removal of the cast and rehabilitation therapy, instability of the joint remains, surgical treatment is prescribed. The operation can also be performed in fresh cases with severe instability of the joint. The intervention is aimed at applying a special suture to a ligament that is torn or torn with a bone plate.
If for some reason suturing is impossible, autoplasty of the ligament is performed. As part of the operation, channels of small diameter (2-3 mm) are formed in the bones in the direction from the back to the palm. A tendon graft is taken from the palmaris longus muscle. It is performed in a figure-of-eight pattern and tightened to eliminate lateral instability but preserve the ability of the fingers to flex and extend. The ends of the graft are sutured. Rehabilitation after such an operation lasts 2-3 weeks.
Important! If the damage is not detected promptly or treated, periarthritis may develop. At the same time, the fingers increase in volume, and the pain persists for a very long time. The patient loses the ability to move his fingers normally and is forced to change his usual lifestyle.
Prevention of rupture/damage to the ligamentous apparatus of the fingers and medical recommendations
To prevent damage you should:
- Try to reduce the risk of injury. To do this, you must always make all movements carefully. Before any physical activity, you should warm up the ligamentous apparatus and the joints themselves. It is very important to monitor the condition of your muscles.
- Visit a doctor regularly if your ligaments and joints are weak (especially if you have any chronic diseases of the musculoskeletal system). An experienced specialist will not only talk about preventive measures, but will also constantly monitor the health status of his patient.
- Pay attention to proper nutrition. You should definitely include foods that are good for your ligaments in your diet. These include fatty fish, ginger, garlic, broccoli, walnuts, fresh berries and fruits. On your doctor's recommendation, you can take complex vitamins regularly.
If you want to learn everything about preventing ligamentous injuries, contact our doctor. You can also make an appointment if you have an injury. Our doctor will prescribe the necessary diagnostics and then carry out treatment. Call us or leave a request on the website!
Anterior cruciate ligament rupture.
Ligaments give stability to the knee joint and keep it in the correct position during movement. The most commonly injured ligament requiring surgery is the anterior cruciate ligament (ACL). This ligament is a strong cord of connective tissue that is directed from the anterior surface of the tibia to the posterior surface of the intercondylar notch of the lateral femoral condyle. The ACL provides anterior-posterior rotational stability and is an important element of proprioception in the sensory chain (proprioception is the ability to perceive the position and movement in space of one’s own body or its individual segments).
Clinical manifestations of an ACL rupture are: pain, limited movement in the knee joint, swelling, hemarthrosis (blood in the joint), redness of the joint area. With minor injuries, these manifestations are minimal, edema and hemarthrosis may not develop. During the examination, the doctor checks the strength of the ligamentous apparatus by performing some tests to determine the stability of the joint.
There are several degrees of ACL rupture, based on the number of damaged fibers and the amount of displacement of the tibia:
- Grade I is a partial rupture in which a small part of the fibers is damaged, but the general anatomy of the ACL is preserved. This degree of damage is also called sprain, but this term is not entirely correct, since the ligament does not stretch, but an incomplete rupture of its fibers occurs.
- II degree - damage to about 50% of the fibers, but the anatomical integrity is still preserved, while the length of the ligament increases. Instability 1+.
- III degree – complete rupture, disruption of the integrity of all fibers, which leads to disruption of the anatomy of the ACL and disruption of joint functions. Instability from 2+ to 3+.
For instrumental diagnostics, radiography is used to exclude possible bone pathology, and MRI is used for direct visualization of ligamentous damage. By comparing clinical manifestations with research results, a decision is made on the need for surgery.
The operation is performed using arthroscopy. Repairing your own torn ligament is currently of little use. However, work to preserve one's ACL is gaining momentum. The most common is plastic surgery of the anterior cruciate ligament from the patient’s tendons of various locations of the lower limb (pes anserine tendon, peroneus longus tendon, patellar ligament, tendon of the quadriceps femoris muscle).
In the postoperative period, it is recommended to walk with crutches without supporting the leg for 2-3 weeks, fixation of the knee joint in a splint (an orthosis that prevents the knee from bending), compression stockings, classes with a rehabilitation specialist, a course of antibiotics, painkillers and anti-inflammatory drugs.
Make an appointment