28 February 2020
36880
0
3.8 out of 5
Fractures are the result of a force that exceeds the resistance of the bone. Compression fractures are no exception and are often the result of injury. They are usually accompanied by head contusion, spinal deformation in the area of injury, and soft tissue swelling. As a result of the injury, the functioning of the pelvic organs and limbs is disrupted, and severe pain occurs.
In children, in the vast majority of cases, compression fractures of the thoracic spine occur, and several adjacent vertebrae are simultaneously affected. But with a compression fracture in children, especially young children, it is not always possible to trace the connection between the episode of application of force to the spine and the presence of a fracture, since they can occur even with a slight load.
Children under 8 years of age rarely suffer spinal injuries.
Most often, compression fractures are diagnosed in children 10–15 years old, since it is at this age that hormonal changes in the body are observed and children are most active, often in traumatic sports and activities. Often, traumatic brain injuries, leg fractures, chest injuries and dislocations are also observed.
What is a compression fracture of the spine in children?
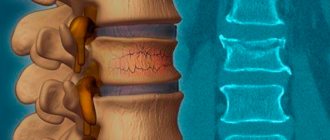
This type of fracture is a type of vertebral injury. When it occurs, one of the parts of the vertebra is flattened, and it takes on a wedge-shaped shape. As a result, the functionality of the musculoskeletal system is disrupted: its shock-absorbing, protective, and balancing properties are reduced.
Sometimes a compression fracture is combined with the formation of fragments that can penetrate the spinal canal and pose a danger to the spinal cord. But even without such a life-threatening complication, injury can lead to serious consequences. Therefore, it is very important to diagnose a compression fracture of the spine in a child as early as possible, to develop and strictly adhere to a treatment strategy. With this approach, fractures in children usually heal quickly and well.
Compression fractures of the cervical spine are especially dangerous, as they can lead to paralysis of the respiratory muscles. And if the spinal cord is also damaged, then complete paralysis will occur.
There are 3 types of spinal compression fractures based on severity:
- mild – vertebral height decreases by 30%;
- moderate – the size of the vertebra is reduced by more than 30%, but less than 50%;
- severe - the vertebra is flattened by more than 50%.
As is already clear, fractures can be complicated or uncomplicated. The latter often occur hidden and cause minor discomfort to the child, which is attributed to a minor bruise. The children's spine is very flexible, and the intervertebral spaces are quite wide. Therefore, even a fall from a small height can cause a compression fracture in a child.
Complicated fractures are always accompanied by neurological disorders, since they damage the nerve roots that weave around the spine or even the spinal cord.
Also, compression fractures of the spine are divided into 3 types based on the nature of the deformation of the bone fragments of the vertebra:
- wedge-shaped - there is flattening of the anterior part of the vertebra, as a result of which it takes on the shape of a wedge;
- avulsion - accompanied by separation of the anterior part of the vertebra and its displacement forward and downward, which causes damage to the ligaments;
- fragmented - the vertebra and most often the adjacent intervertebral disc are crushed into separate fragments, which creates a high risk of spinal cord injury at the time of injury or after it.
Depending on where the blow occurred, fractures of the cervical, thoracic, lumbar and lumbosacral spine are distinguished.
The most vulnerable vertebrae
Fractures can be of traumatic origin, occurring in a healthy spine due to trauma and pathological etiology, when a violation of the integrity of the thoracic vertebrae occurs due to internal processes (for example, osteoporosis). Compression fractures (CFs) are widespread.
Under such conditions, significant pressure occurs on the anterior zones of the vertebral body, followed by cracking of its structures and compression (subsidence) of the vertebra in height. With a critically severe wedge-shaped deformity of the thoracic segment, compression develops on the spinal cord and nearby nerve endings, which causes acute neurological symptoms. According to the ICD (International Classification of Diseases), this category of injuries is assigned the following codes:
- S22.0 if only one thoracic vertebra is damaged;
- S22.0 – with a fracture of several vertebral elements in the thoracic region.
Types of fractures.
Compression fractures occur at the border of the thoracolumbar junction, at any of the levels such as T11, T12, L1 and L2. The area within T11-L2 experiences significant load forces and is characterized by complex biomechanics. T11 and T12 are the most vulnerable points of the thoracic region. The T6 segment is affected somewhat less frequently, and in the rarest cases the lesion occurs on the remaining elements.
Causes of compression fractures in children
The vast majority of children are very mobile, which causes a high risk of injury. Children tend to overestimate their own physical capabilities and often do not think about the consequences of careless actions. Therefore, the main causes of injury are:
- a child falling from a height onto his back, head, buttocks or legs;
- incorrect technique for performing somersaults;
- diving;
- automobile or other accidents;
- heavy objects falling on your head or shoulders.
Also, flattening of the vertebral bodies can be a consequence of spinal weakness, which occurs against the background of pathologies in the child’s development or other diseases of the musculoskeletal system. These may include osteoporosis (often observed with long-term use of corticosteroid drugs), osteomyelitis, cancer, etc.
Even natural childbirth can cause a compression fracture in a child immediately after birth or subsequently as a result of the formation of vertebral dislocations. The situation is aggravated by a deficiency of minerals in the body, especially calcium, which may be a consequence of an unbalanced diet of the mother during pregnancy.
Mechanisms of occurrence of a thoracic fracture
The leading provoking factors are:
- a strong blow to the spine;
- traffic accident;
- falling from a height, landing on straight limbs or buttocks;
- severe osteoporosis, in which pathogenesis can occur with the simplest loads, even at the moment of sneezing or coughing;
- lifting weights;
- intraosseous neoplasms, hemangiomas;
- cancer pathologies of other organs.
The most common circumstances of fracture.
Women are most susceptible to osteoporosis after menopause. As statistics show, about 40% of female patients closer to 70-80 years old have CP of at least one vertebral body.
Signs of spinal compression fracture in children
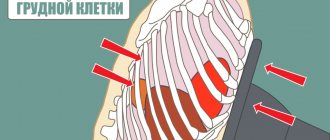
The main manifestations of spinal injury are severe pain at the site of application of force and short-term cessation of breathing. Often the pain radiates to the chest, the child cannot fully inhale and exhale, and the head takes a forced position - leans down. In this case, the victim tries to avoid moving his head, and the neck muscles reflexively tense. Sometimes the pain is so severe that the child cannot get up on his own, and the nasolabial triangle acquires a bluish tint.
With cervical fractures, pain is mainly present in the neck area and intensifies with head movements. There is definitely a reflex tension of the muscles, as a result of which the neck can bend.
Gradually, the pain subsides, breathing difficulties disappear, and the child makes attempts to rise to his feet. This causes parents to make false conclusions about the insignificance of the injury and the absence of the need to seek medical help.
According to statistics, less than 30% of children receive qualified medical care for spinal compression fractures in the first day after injury.
The pain goes away completely within a few days if the child adheres to bed rest. Physical activity provokes increased pain and fatigue. Therefore, there are also such indirect symptoms of a compression fracture of the spine as:
- stiffness of movements;
- gait changes;
- lethargy;
- lethargy.
Sometimes there is a slight protrusion of part of the broken vertebra.
Since the blow often falls not only on the spine, there may additionally be injuries to the arms or legs, as well as damage to internal organs. Thus, when the lumbar region is injured, abdominal pain, swelling and soft tissue hematomas may be present.
If the fracture is complicated, neurological symptoms occur immediately after the injury or after some time:
- decreased muscle tone and limited mobility;
- loss of control over urination and bowel movements;
- numbness in the arms or legs;
- decreased severity of reflexes;
- disruption of the functioning of internal organs innervated by nerve roots corresponding to the level of damage to the part of the spinal cord.
Such situations cannot be delayed, as they can lead not only to permanent disability, but also to death.
Therefore, after a fall, a blow to the head or back, or in the absence of such, the child’s parents should consult a vertebrologist or traumatologist if he or she experiences:
- breathing problems;
- back muscle tension;
- swelling, hematoma at the site of injury;
- stiffness of movements;
- pain in the chest or stomach.
Physical rehabilitation
Rehabilitation for a spinal fracture is the next stage of the treatment process of paramount importance. After providing first aid, even if it involved minimally invasive cementoplasty, the patient must strictly observe a specific physical regimen for a certain period, attend physiotherapeutic sessions, undergo therapeutic exercises, etc. It cannot be otherwise if you have suffered such a serious injury.
Complicated injuries and those provoked by osteoporotic processes require a very careful selection of recovery methods. Therefore, it would be more advisable to take care in advance where to undergo rehabilitation after a spinal fracture; today there is no particular shortage of good specialized institutions.
Prescribing any restorative tactics to yourself is strictly prohibited! Rehabilitation of patients with a spinal fracture is being developed exclusively by the treating doctor together with a rehabilitation specialist. Our recommendations are given in general form and are for informational purposes only, so before using them, consult with a specialist about the possibility of using them for your specific medical problem.
We will talk about that important period when complete bone consolidation has already been achieved, since some patients at this stage stop working on their spine, but in vain. It is after 2-3 months that all emphasis should be directed toward developing and strengthening the musculoskeletal corset, which has become considerably weakened after prolonged immobilization and long-term unloading. In addition, thanks to the unique physical organization, the work of the gastrointestinal tract, cardiovascular system, respiratory system, reproductive, urinary system and many other important components of the body, which are entirely dependent on the health of the spine, will be stabilized.
Diagnostics
Patients with suspected compression fractures of the spine are delivered in a supine, fully fixed position to the traumatology and neurology departments. The doctor examines the patient and finds out under what circumstances the injury occurred. He palpates the soft tissue in the projection of the injury site and determines the degree of pain.
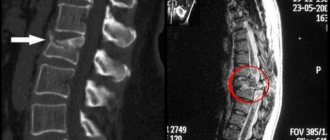
To finalize the diagnosis, the patient is referred to:
- radiography of the spine in two projections;
- CT;
- electromyography;
- scintigraphy;
- MRI.
If a doctor suspects that a child has osteoporosis, he will order densitometry. And to exclude head injuries and damage to internal organs, in the presence of appropriate symptoms or prerequisites, it is recommended to perform an X-ray of the skull and an ultrasound of the internal organs.
Treatment
Initially, victims are provided with first aid directly at the scene of the incident by doctors from the ambulance team. The child is given an anesthetic, carefully placed on a stretcher, immobilized and taken to a specialized medical facility.
Diagnosis is carried out directly there and therapy is prescribed based on the research results. Most children are indicated for spinal traction, which involves the use of a special apparatus. The patient is placed on an orthopedic bed and secured to the head or shoulders with loops of the device. Then a tensile load of the required magnitude is created. Sometimes reposition can also be used, that is, a gradual increase in the angle of the bed. This allows you to improve the degree of extension of the spine.
For uncomplicated fractures, conservative therapy is prescribed, including:
- compliance with bed rest and wearing an orthopedic corset subsequently for at least 2 months;
- drug treatment;
- exercise therapy;
- physiotherapy;
- manual therapy.
But if neurological symptoms occur or a real threat of spinal cord damage is detected during the examination, the child is recommended to undergo surgical intervention.
Drug therapy
Depending on the complexity of the fracture, children may be prescribed:
- analgesics;
- antibiotics;
- corticosteroids;
- chondroprotectors;
- immunomodulators;
- calcium and vitamin D supplements.
Exercise therapy
Physical therapy exercises are important for maintaining muscle tone, reducing the risk of developing muscle atrophy and improving the functioning of internal organs. They begin almost from the first days of treatment. Initially, the specialist performs breathing exercises with the child.
As the spine recovers, they move first to performing passive exercises, then active ones, but still from a lying position. After the child is allowed to stand up and move independently, new exercises are introduced. The complexity and intensity of the load gradually increases.
Physiotherapy
To increase the effectiveness of conservative therapy, children are recommended to undergo a course of physiotherapeutic procedures, including:
- electrophoresis;
- myostimulation;
- Ural Federal District;
- UHF;
- ultrasound therapy;
- massotherapy.
Surgical treatment of spinal fractures in children
For complicated fractures, surgery is always prescribed. It is also indicated for compression fractures of grades 2 and 3 or the absence of effect from conservative therapy.
Depending on the characteristics of the injury, the neurosurgeon may recommend one of the types of modern minimally invasive surgical interventions. Some of them are performed through a pinpoint puncture of soft tissue in the projection of the affected vertebra. Therefore, after the procedure, not even an invisible scar remains on the skin.
Other surgical methods are more traumatic, but are also used to solve more complex problems. Therefore, only a neurosurgeon can correctly select the optimal surgical tactics for a compression fracture of the spine in a child.
Vertebroplasty
Vertebroplasty is one of the methods of percutaneous surgery, which involves filling the defect formed as a result of injury with a special mass called bone cement. It can be carried out if the height of the vertebra is reduced by no more than 70%.
Bone cement is a thick, viscous polymer-based mass that tends to harden quickly and is highly safe and biocompatible.
The essence of the operation is to insert a thin hollow needle into the body of a broken vertebra under local anesthesia under the control of an image intensifier. Once it reaches its target, prepared bone cement is injected through it. Thanks to its creamy consistency, it fills all the cavities of the vertebra, and the quality of elimination of the existing defect is controlled by the neurosurgeon through the image intensifier. The substance hardens completely in 8–10 minutes and turns the vertebra into a highly durable conglomerate, after which the needle is removed and the insertion site is covered with a sterile bandage.
In addition to polymethyl methacrylate, bone cement contains a contrast agent and antibiotics. This allows you to accurately control the quality of filling the vertebra with it and minimize the risk of developing infectious and inflammatory postoperative complications.
Thanks to vertebroplasty, it is possible not only to eliminate the consequences of a vertebral fracture, but also to increase its strength, which is a good prevention of injuries to this spinal motion segment in the future. In 85% of cases, the method improves the result instantly.
Kyphoplasty
Kyphoplasty is very similar to vertebroplasty, but has broader capabilities. With its help, you can not only eliminate a vertebral defect, but also restore its natural size. Therefore, it can be used when the vertebra is flattened by more than 70%. An additional advantage of kyphoplasty is the ability to eliminate kyphotic deformity, which is often observed with compression fractures in children.
The main difference between this method and vertebroplasty is the introduction of a balloon into the broken vertebra, into which a saline solution with a contrast agent is injected. This allows you to “straighten” it to normal size and completely eliminate the deformation of the ridge.
Manipulation is also carried out under the control of an image intensifier through a pinpoint puncture of soft tissue. Therefore, the neurosurgeon can accurately determine how much saline solution should be injected into the balloon. Once the anatomical dimensions of the vertebra have been restored, the fluid is removed and the vertebra is immediately filled with bone cement. After 10 minutes, it hardens, which allows you to remove the cannula and cover the pinpoint puncture of the skin remaining after the operation with a sterile bandage.
An additional advantage of the method is that it reduces the risk of bone cement leaking outside the spine.
Transpedicular fixation
If a compression fracture of the spine in a child has led to the development of instability, it is impossible to correct the situation using microsurgical methods. In such cases, neurosurgeons have to resort to transpedicular fixation.
This operation is performed only under general anesthesia and involves the use of titanium structures to secure the injured vertebrae in the correct position. It is performed through a soft tissue incision in the projection of the broken vertebra. Then the neurosurgeon exposes the processes of the vertebra and its arches. This allows you to visualize the intersection of the transverse and articular processes.
It is at this point that a special probe makes a hole into which titanium screws are screwed. Each vertebra has two such points. Depending on the complexity of the situation, the manipulation is repeated on all vertebrae requiring stabilization. Often the final design includes 4-6 screws. Between them, springy rods are passed through special holes in the caps, ensuring uniform distribution of the load during physical activity on all fixed vertebrae.
The variety of sizes and shapes of titanium screws allows you to choose the best option for each situation and damage to any part of the spine in a child of any age. And since titanium is an absolutely biologically inert material, characterized by high strength, the created structure does not harm the body and can last for several decades.
Rehabilitation after surgical treatment of injury
The duration and complexity of the rehabilitation period depend on the nature of the resulting fracture. Immediately after surgery, patients are usually placed in a plaster cast or an orthopedic corset. How long you will need to wear it is determined by what surgical treatment tactics were used.
Drug therapy is also prescribed. After some time, the patient is recommended to undergo massage, exercise therapy and physiotherapy.
During rehabilitation, parents bear a lot of responsibility. They should closely monitor the child’s physical activity, correct use of the orthopedic corset and nutrition. It is recommended to enrich the diet with foods that contain high levels of calcium, magnesium, zinc and B vitamins.
Symptoms and medical care
Let's start with the symptoms that are characteristic of this classification of traumatic lesions. The main symptoms include:
- acute local pain, it can radiate to the arms and legs;
- pain when palpating the diseased part;
- local swelling and hyperthermia of soft tissues,
- visible traces of injury on the skin (redness, abrasion, bruise, etc.);
- loss of sensitivity in the limbs, feeling of muscle weakness;
- asymmetry of the vertebral axis and visible deformities;
- reduction in range of motion or complete immobility of the problem area;
- difficulty breathing;
- girdle pain in the abdominal cavity;
- general malaise, sometimes fever.
In the early period, emergency drug therapy is recommended in parallel with an accurate determination of the nature and severity of the injury to determine the advisability of surgical treatment. Based on the results of a thorough diagnosis, the doctor decides whether to perform surgery or treat conservatively. Upon completion of the treatment cycle, rehabilitation always follows at a certain stage; after a fracture of the thoracic spine, etc., it is an extremely necessary measure.
Possible complications
Compression fractures of the spine in a child are a serious situation that cannot be neglected. If you do not follow the doctor’s recommendations or even lack qualified medical care, you may develop:
- spondylitis;
- kyphosis;
- osteochondrosis;
- spinal canal stenosis;
- paresis, paralysis;
- vertebral instability;
- disturbances in the functioning of internal organs, including the heart, lungs, gastrointestinal tract and pelvic organs.
Timely treatment, including surgery, allows the child’s spine to fully recover in most cases, especially with grade 1 compression fractures. Problems and consequences of injury usually occur with complicated fractures, since it is often at the time of injury that serious injury occurs to nerve structures that cannot be restored.