Diagnostics
To diagnose injuries to the menisci of the knee joint, the following methods are used:
- ✅ Clinical (complaints and medical history, objective examination of the patient).
- ✅ Radiation (x-ray, MRI, ultrasound).
- ✅ Clinical examination.
There are many methods available to differentiate meniscus damage from other injuries. Since there is no generally accepted method, it is recommended to use several tests at once. In addition, negative test results cannot rule out a meniscus tear, since the sensitivity of the tests is 60-90% depending on the clinical experience of the doctor.
The most important signs of a meniscus tear include tenderness in the joint space, a positive McMurray (maximum flexion, external rotation and palpation in the projection of the joint space when extending the joint in external rotation), Steinmann's sign I (posteriorly moving pain when flexing) and Fouche's (reverse McMurray test with internal rotation of the tibia).
MRI of the knee joint
Many patients report a rotational knee injury or a sudden pain and tearing sensation while doing a squat. Meniscus tears may cause transient restrictions in joint movement and clicking sounds.
Old meniscus tears are accompanied by atrophy of the quadriceps femoris muscle, seasonal extravasation, and transient or permanent limitations of movement in the knee joint. Acute ruptures are usually accompanied by clinical signs of acute trauma, hemarthrosis, and damage to the capsule and ligaments (collateral ligament, ACL)
Symptoms of degenerative changes in the menisci
The main manifestation of degeneration of the menisci of the knee joints is periodic aching pain. Most often they appear after the start of movement after rest, and then intensify after walking, playing sports or physical work. Over time, the pain syndrome gains intensity, which indicates the progression of degenerative changes.
It is also possible that:
- mobility impairments, discomfort while walking, especially on stairs;
- crunching and clicking in the knee during movements;
- a feeling of knee instability (patients often say that they cannot rely on their knee);
- sensation of friction inside the knee joint.
Fragmentation of the free edge of the lateral meniscus can be completely asymptomatic.
If, against the background of this, a rupture or other damage to the meniscus occurs, acute, sharp pain is observed at the time of injury. If the torn piece of cartilage gets under the moving articular surfaces, the knee will be locked in a bent position. Any attempts to straighten it will be extremely painful. At the same time, they also pose a serious threat of even greater injury to the meniscus, so you should never try to forcefully straighten the knee. In such situations, you need to consult an orthopedist! This is often accompanied by rapidly increasing swelling of the knee and the formation of hematomas and bruises.
Traumatic injuries to the menisci that occur against the background of their degenerative changes are usually accompanied by hemarthrosis. In such situations, blood accumulates inside the joint, which requires a puncture to remove it.
Radiation research methods.
In all patients with clear clinical symptoms, radiographic examination should be performed in two projections - anteroposterior and lateral.
Old injuries (2-3 months) are accompanied by changes in the edge of the ipsilateral tibial plateau with the deposition of periosteal deposits or the formation of osteophytes (Rauber's sign), which can grow up or down from the edge of the eminence. It is also possible for the cortex to thicken without the formation of osteophytes. Radiographic signs of meniscal cysts in the anteroposterior projection are depressions of the medial and lateral plateau of the tibia with pointed and sclerotic edges.
Magnetic resonance imaging is a highly informative method for assessing meniscus damage.
knee joint. According to MRI, there are four degrees of changes in the meniscus (classification according to Stoller).
- ✅ Grade 0 is a normal meniscus.
- ✅ Degree I is the appearance of a focal signal of increased intensity in the thickness of the meniscus (not reaching the surface of the meniscus).
- ✅ Degree II - the appearance of a linear signal of increased intensity in the thickness of the meniscus (not reaching the surface of the meniscus).
- ✅ Degree III - a signal of increased intensity that reaches the surface of the meniscus. Only grade III changes are considered a true meniscus tear. It is possible to distinguish grade III a, when the tear extends to one edge of the articular surface of the meniscus, and grade III b, when the tear extends to both edges of the meniscus.
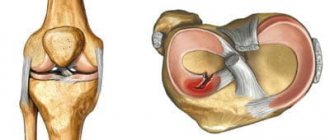
The accuracy of MRI in diagnosing a meniscus tear is approximately 90-95%, especially if a signal of increased intensity is recorded twice in a row (i.e., on two adjacent sections), covering the surface of the meniscus. To diagnose a tear, you can also focus on the shape of the meniscus. Typically, on sagittal plane images, the meniscus has a butterfly shape.
Any other shape could be a sign of a rupture. A sign of rupture is also the symptom of “double posterior cruciate ligament” (or “third cruciate ligament”), when, as a result of displacement, the meniscus ends up in the intercondylar fossa of the femur and is adjacent to the posterior cruciate ligament.
A meniscus tear can be detected by MRI even in the absence of complaints from the patient, and the frequency of such cases increases with age. This shows how important it is to take into account all clinical and radiological data during the examination.
Treatment of knee meniscus damage
The diagnosis is made after an X-ray examination and, if necessary, an ultrasound examination of the articular cavity for the presence of hemarthrosis.
The therapy is complex and includes sessions of physical therapy, massage, and proper nutrition to reduce the load on the sore joint. For the entire period of treatment, the victim’s leg is fixed with a plaster cast or orthosis.
Conservative methods
Articulation blockade is eliminated by injecting lidocaine with a corticosteroid into the joint cavity. This manipulation reduces pain and prevents the risk of developing hemarthrosis and inflammatory processes. The procedure should be carried out no more than once every two weeks.
Additionally, the doctor prescribes NSAIDs and diuretics (for severe swelling).
After the inflammation is relieved, the patient is prescribed a course of physiotherapy (magnet, laser, electrophoresis, UHF) and massage sessions. If you are immobile for a long time, physical therapy exercises are recommended.
Surgery.
Rationale for the choice of surgical treatment technique.
The arthroscopic method of diagnosis and surgical treatment of knee joint pathology is currently very widespread. One of the most common procedures is endoscopic meniscectomy.
Arthroscopic meniscectomy has a number of advantages over open one, since, being a low-traumatic technique, it makes it possible to examine and manipulate almost all parts of the knee joint, especially in the posterior ones, which previously belonged to the “blind” zones; in addition, arthroscopic meniscectomy provides the opportunity for economical removal only the torn and hypermobile part of the meniscus with minimal disruption of the contact area of the joint, which significantly reduces the time of rehabilitation treatment for patients.
Indications for surgical treatment - arthroscopic meniscectomy
Indications for arthroscopic meniscectomy are pain in the knee joint in the projection of the joint space, repeated blockades of the joint, limitation of joint movements, and ineffectiveness of conservative treatment.
Treatment tactics largely depend on the morphological changes in the meniscus identified during arthroscopy, the results of comparison of clinical and arthroscopic data, as well as the following factors:
- ✅ Patient's age.
In children and young patients, meniscus repair is performed despite potential technical difficulties. In older patients, especially those with medial meniscal lesions, relatively extensive resection including the posterior middle third of the meniscus and posterior horn is recommended. This is necessary to prevent re-ruptures and repeated operations. - ✅ Localization of damage.
For the functioning of the knee joint, the lateral meniscus is more important than the medial one, therefore the main task in case of damage to the lateral meniscus is to ensure its safety and, if possible, perform reconstruction. Extensive resection of the lateral meniscus inevitably leads to osteoarthritis in the lateral part of the joint. Tears of the medial meniscus are more common than lateral ones, and even minor injuries lead to severe clinical manifestations. What is the indication for partial resection? - ✅ Prevalence of meniscus lesions.
- ✅ Related changes.
Associated cartilage damage and joint instability (eg, due to ACL injury) significantly reduce the chances of recovery. To preserve the initial result of suturing the meniscus, it is necessary to perform a one-stage reconstruction of the ligaments and restore joint mobility within several weeks. - ✅ Activity level.
Meniscus repair is always the best option for athletes with acute tears. For professional athletes, the effectiveness of meniscus suturing is much lower due to the need for long-term rehabilitation with limited sports activities.
Instruments required for arthroscopic surgical treatment.
The instruments required for arthroscopic surgical treatment are usually divided into five main types:
- ✅ Mechanical (straight, deflected, curved and retrograde tools: basket forceps, scissors, knives, clamps)
- ✅ Electromechanical (shavers)
- ✅ Electric (electrocautery)
- ✅ Laser
- ✅ Special (guides, staplers, etc.)
Methods of surgical treatment
The following types of treatment exist:
- ✅ Resection.
Meniscal resection is the most commonly performed arthroscopic procedure, which removes unstable torn areas as well as areas of degenerative scarring of the meniscal tissue.
There are several resection techniques: piecemeal resection, en bloc resection, a combination of piecemeal and en bloc resection . The choice of the extent of resection is key. It is important to remove as little of the meniscus as possible and as much as necessary. - ✅ Stitching.
The technique for suturing the meniscus should be simple and quick. If suturing the meniscus takes more than 5 minutes, it is better to resect the torn fragment.
Regardless of the fixation technique used, reconstruction consists of two stages:
- ✅ Refresh the tear zone
- ✅ Repairing the gap
All currently used meniscus suturing techniques can be divided into three main groups:
- ✅ From outside to inside
- ✅ From the inside out
- ✅ Everything from the inside
It is possible to use both suture material and various fasteners:
- ✅ Horizontal seam
- ✅ Single vertical seam
- ✅ Double vertical seam
- ✅ Mitek Meniscal Repair System (H-fix)
- ✅ Clearfix Meniscal Screw
- ✅ Arrow (manual or automatic)
- ✅ T – fix, Biostinger
- ✅ Combination of resection and suturing
- ✅ Refreshing tear edges
- ✅ Debridement, piercing, perimeniscal synovectomy, fibrin plug application.
- ✅ Non-interference
Not all identified meniscus tears manifest clinical signs. In this regard, it is necessary to correlate morphological data with the patient’s complaints.
Position of the patient during surgery.
It is preferable to use the patient position with the knee bent. The patient is placed on the operating table in a supine position with the legs bent at the knee joints at an angle of 90 degrees to relax the femoral muscles and relieve tension in the muscles of the lower extremities.
The thigh is rigidly fixed in a special stand, the knee is bent, and the lower leg hangs from the table. This provides a medial fulcrum, which allows for valgus and varus loads to be created in the joint.
The use of a tourniquet and extremity bleeding remain controversial issues in arthroscopic surgery.
Operation execution scheme
Standard lower arthroscopic approaches .
The inferior lateral approach is performed with a narrow scalpel (45 degrees to the frontal plane of the knee) in a triangle bounded by the lateral edge of the ligamentum patella (1 cm from it), the lateral femoral condyle and the tibial plateau (1 cm above it).
The lower medial approach is made with a scalpel in the same way, but under visual control of the arthroscope inserted into the joint cavity from the lateral side and along the guide needle, which is used to pre-puncture the knee in the medial triangle. The latter access is used for the introduction of microsurgical manual and power instruments.
Main stages and technique of arthroscopy:
Procedure for examining the knee joint.
- ✅ Upper section: synovial volvulus and patellofemoral joint are examined with the joint extended.
- ✅ Medial compartment: widening the medial joint space for viewing the posterior medial space is achieved by valgus deviation of the tibia with the knee extended and bent (170-150 degrees); for optimal viewing of the anterior medial space, flexion of the joint up to 90 degrees is recommended.
- ✅ Intercondylar department: examination of the articular elements located in it is carried out with a bent (up to 90 degrees) knee with an almost horizontal arrangement of the arthroscopic viewing system. In this position, it is sometimes possible to penetrate the medial edge of the anterior cruciate ligament, providing a view of the posterior cruciate ligament and the insertion of the posterior horn of the medial meniscus.
- ✅ Lateral section: examined in the position of joint flexion (up to 80-100 degrees) with varus deviation of the tibia, which leads to expansion of the lateral joint space.
When examining the menisci and condyles of the femur, flexion-extension and rotational movements of the leg, palpation of the joint space from the outside, the use of a hook-shaped arthroscopic probe, and, if necessary, the use of other approaches are required.
The following instrumental support for the operation is optimal: basket forceps and straight scissors - necessary for cutting off torn fragments in the posterior and middle segments of the menisci; scissors curved at an angle of 20 and 60 degrees - for working on the anterior segment of the menisci. It is mandatory to model smooth transitions at the boundaries of the resected and remaining parts of the menisci using lateral (90 degrees) forceps and smoothing the edges with an electric knife.
Typically, arthroscopic meniscectomy is performed from two anteroinferior approaches: lateral and medial
. During surgery, sometimes it becomes necessary to change positions between the arthroscope and the surgical instrument, and in difficult cases, to use additional approaches.
It is advisable to stop the operation if the duration exceeds 45 minutes due to imbibition of soft tissues by the irrigation fluid and if visibility deteriorates due to heavy bleeding.
During medial meniscectomy, the viewing optical system is inserted through the lower lateral approach, and the surgical instrument is inserted through the lower medial. To do this, under visual control, the most direct distance to the damaged segment of the meniscus is selected and an injection needle is inserted into the anteromedial part of the joint, along which an incision is made with a scalpel.
The optimal access to the posterior segment of the medial meniscus is an incision in the suprameniscal zone at a distance of 1 cm from the ligamentum pattela. In this case, the inserted surgical instrument should be located as parallel as possible to the tibial plateau.
For external meniscectomy, the anteroinferior lateral incision should be made lower than usual to improve access to the posterior aspect of the joint. Resection of the posterior and middle segments of the meniscus can be facilitated by introducing the arthroscope through the infero-medial approach, and surgical instruments directly through the infero-lateral approach.
When working in the anterior segment, it is advisable to use instruments curved 90 degrees and insert them into the joint cavity through the anteromedial approach. Such a scheme is not mandatory, and the position of the instruments depends on the convenience for the operating surgeon and ensuring maximum atraumaticity of the surgical intervention.
Causes of meniscus injury
First of all, chronic diseases affect the destruction of the meniscus. They make its tissues fragile, thin and inelastic. It is enough to slip and make an awkward sudden movement, and a rupture will occur. This can happen even without the fact of a fall. Diseases that reduce the quality of meniscus tissue:
- rheumatoid arthritis;
- gout;
- gonarthrosis;
- chronic intoxication.
The most traumatic movement for the meniscus is rotation of the leg with the knee joint bent. This is why meniscal tears are common in hockey players and skiers - both sports involve a characteristic movement of the leg in a bent position.