Causes of scoliosis in adolescents
This disease can be of two types. Namely:
- Congenital.
- Acquired.
Treatment of scoliosis in children and adolescents in the first case will be needed due to the fact that there was an abnormal formation of the child’s body in the womb. It is impossible to prevent this state of affairs. Acquired scoliosis is provoked by a number of factors. These include:
- incorrect posture;
- insufficiently strong muscle corset;
- uneven development of bones and muscles;
- carrying heavy weights on one shoulder;
- insufficient physical activity;
- vegetative-vascular dystonia;
- injuries received.
Treatment of grade 2 or 3 scoliosis in adolescents will depend on the reasons that led to this condition.
Scoliosis: what is it
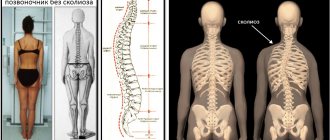
Scoliosis is a steadily progressive lateral curvature of the axis of the spinal column, followed by twisting of the vertebrae and increased physiological curves. This is accompanied by a change in posture and body proportions. Patients have protrusion of the shoulder blades, asymmetry of the shoulders and skewed hip line. Without appropriate therapy, under the influence of physical activity, the deformation constantly intensifies, the chest is distorted, and in severe cases, the body becomes so distorted that the internal organs begin to suffer seriously.
The most dangerous periods for the occurrence of pathology are considered to be the stages of intensive growth of a child, occurring at 4–6 years and 10–14 years. It is at this age that stage 1 spinal scoliosis in children is most often diagnosed for the first time and treatment begins. Although there are often cases when pathology is first detected in adults.
The reasons for the development of the disease lie in:
- developmental anomalies;
- neuromuscular diseases, including SMA (spinal muscular atrophy, cerebral palsy, muscular dystrophy;
- metabolic disorders;
- suffering severe injuries;
- degenerative-dystrophic processes;
- different leg lengths.
Often the cause of scoliosis cannot be determined and treated. In such situations, an idiopathic form of the disease is diagnosed, and all efforts are directed toward eliminating the curvature of the spinal deformity.
Types of scoliosis in adolescents
Scoliosis that occurs in children during adolescence (10–17 years) is called juvenile scoliosis. It differs in the number of arcs of curvature:
- C-shaped - one arc of curvature, this is the most common type of disease;
- S-shaped - the spine is curved in two sections in two directions at once;
- Z-shaped – this type of scoliosis is the most difficult to treat.
It also happens (extremely rarely) that the vertebral curve is accompanied by a curvature of the sternum and a hump on the ribs - kyphoscoliotic scoliosis. Scoliosis also occurs in adolescents from the first stage and progresses to the fourth. On the first, the curvature is 5–10 degrees, on the second – 11–25 degrees, on the third – 26–50 degrees, on the fourth – more than 50 degrees.
Diagnostics
Inspections in schools. As a rule, examinations of schoolchildren are carried out in grades 5-6, when puberty begins and the skeleton begins to grow. The school nurse typically uses the Adam's forward bend test, which is the most common physical screening test for scoliosis. During this test, the child bends forward at the waist with his arms straight out in front, as if plunging into a swimming pool. This usually reveals abnormalities such as bulging ribs or an abnormally shaped back.
The Adam Forward Flexion Test helps detect the presence of a curve, but it cannot determine how severe the curve is. To do this, you need to consult a doctor.
Symptoms
At the very beginning, immediately after its appearance, scoliosis does not show itself at all; characteristic symptoms appear only from the second stage. She is like this:
- the child's head is constantly lowered;
- the shoulders are pulled together, the child is slouched;
- the teenager does not place his shoulders at the same level.
At the third stage, the spine is clearly curved, discomfort and back pain appear, and the head begins to hurt. In addition, parents seriously think about how to treat grade 2 or 3 scoliosis in a teenager when their child develops shortness of breath and the heart begins to beat faster.
Medical Imaging Techniques
Your doctor may order imaging tests, such as X-rays, CT scans, and magnetic resonance imaging (MRI). Image analysis allows the doctor to see where scoliosis has developed in the spine and the extent of the curve. In addition, imaging techniques are very important as they are necessary to plan an individual treatment plan.
Although MRI and CT scans may be used in some patients with suspected scoliosis, radiography is the standard imaging modality for identifying and monitoring curve progression.
To see the entire length of the spine, the child must stand during the x-ray. Two types of radiography are commonly used to fully identify curvature:
- posterior/anterior and lateral (side) x-ray.
- When the body is tilted to the side, X-rays determine the flexibility of the spine.
The X-ray results allow the doctor to measure and classify the curve based on its extent in degrees.
- Curves exceeding 25 degrees to 30 degrees are significant.
- Curves exceeding 45 degrees to 50 degrees are severe.
X-rays are not only key to illustrating the full nature of scoliosis—they are also important in determining skeletal age and bone maturity. The progression of the curve may stop once the child reaches adulthood, so knowing how many years are left until growth is complete is important for treatment planning.
To determine the age of the skeleton, the doctor can compare an X-ray of the spine with a standard. This will determine the maturity of the bone tissue and the risk of progression.
X-rays are an integral part of diagnosis, but they are also used to monitor the progression of the curve and guide treatment decisions long after the initial diagnosis has been made. These additional x-rays cause radiation problems, especially the effects on breast tissue.
To reduce any adverse effects of spine scans, doctors limit the number of x-rays a patient receives each year and use lead shields to protect breast tissue.
How to diagnose scoliosis in a teenager
It is important not only to consult a doctor in a timely manner if there are visible problems, but also to be attentive to the state of your child’s health. In order to begin timely treatment of grade 1 and 2 scoliosis in a child, it is worth learning some methods for diagnosing the pathology. Namely:
- Ask the child to lie on his stomach and examine his spine: if you see a curvature that does not go away with a change in position, most likely you have scoliosis.
- Ask the child to stand with his back to you, stretch out his arms and bend over: if you notice asymmetry, it makes sense to see a neurologist
.
In order to confirm or refute the diagnosis of scoliosis, the doctor prescribes an x-ray of the spinal column in an upright position, using the Cobb technique. The doctor will determine the presence of scoliosis and its degree - 1, 2 or 3, and tell you how to treat this pathology in a teenager.
Risk factors for developing the disease
For those who have been diagnosed with one degree or another of scoliosis, the question will always be relevant: what can the disease lead to? Is there a high risk of developing serious complications and developing the disease to more serious degrees?
Of course, there is always a minimal chance, but don’t be scared right away. First, you need to consider the origin of your disease: congenital or acquired. The congenital type has a slightly higher chance than the acquired type. The localization of scoliosis in this case is not particularly important.
There are a number of common factors that can influence the worsening of scoliosis:
One of the reasons for the development of scoliosis is muscle weakness. The presence of deformities in one (or both) parents;- Congenital muscle weakness;
- Poor posture (including hyperlordosis);
- The presence of other deformities not associated with scoliosis (deformations in the chest or hip region);
- Presence of systemic hypermobility. This factor will apply to people involved in one or more sports that require a lot of stretching (ballet, gymnastics, yoga);
- Weak muscle activity and passive lifestyle;
Of course, this is not the entire list of factors that can aggravate the situation. We advise you to consult a specialist as soon as a diagnosis is made. The doctor will be able to give recommendations and monitor the treatment process, and will also ensure that complications do not develop.
Video: “What is scoliosis?”
Treatment of scoliosis in adolescents
The method of treatment is determined by the doctor depending on the degree of development of the disease, as well as the general health of the child. It often happens that juvenile scoliosis is already very advanced and has managed to provoke a lot of complications, so treatment is strictly individual.
Exercise therapy and gymnastics
If you are thinking about how to correct scoliosis in a teenage child, gymnastics will be very useful in this case. The following exercises are used:
- “swallow” - in a position on your stomach, you should raise your arms and legs up and lower them back;
- “scissors” - lying on your back, slightly raise your legs and arms and swing them, crossing and spreading your limbs;
- “bicycle” – raise your legs up on your back and imitate pedaling;
- walking on tiptoes with arms raised up.
These exercises will help you get rid of the disease over time.
Massage
Treatment of spinal scoliosis in adolescents
This also includes a massage that improves blood circulation in the back muscles. Such influences will allow you to quickly get rid of the curvature of the spinal column.
Surgery
Gymnastics and exercises will be useful for scoliosis of 1-2 degrees in a teenager, but at stages 3 or 4 the child’s health may be unsatisfactory. Surgical intervention is necessary if the disease is accompanied by complications, very severe pain, neurological symptoms, shortness of breath, heart failure, etc.
Posture correctors
Treatment of stages 2 and 3 is impossible without the use of corsets. They will help straighten the teenager’s posture, while reducing the load on the spinal column. If a doctor promptly prescribes a corset for a teenager with scoliosis, the pathology can be completely eliminated.
Scoliosis degrees
According to the international classification, there are 4 degrees of deformation:
- The angle of curvature does not exceed 10°. There is a slight stoop, signs of asymmetry in the waist and shoulder level. The patient involuntarily keeps his head down. An x-ray reveals a tendency to rotate the vertebrae.
- The curvature reaches 11–25°. When changing body position, the curvature of the spine does not disappear. With right-sided scoliosis of the 2nd degree, there is a prolapse of the right half of the pelvis, distortion of the waist triangle and the outline of the neck. A protrusion forms on the right side in the chest area, and a muscle roll forms in the lumbar region. When curving to the left side, the changes are mirror-like in nature. X-rays show twisting of the vertebrae.
- The angle of curvature is in the range of 26–50°. To the above signs is added protrusion of the anterior costal arches and the acquisition of clear outlines of the costal hump. At the same time, the tone of the abdominal muscles decreases.
- The angle exceeds 50°. The body is severely deformed. All of the above symptoms are intensified many times over.
What causes lead to spinal deformity?
As already noted, spinal curvatures in children can be congenital (about 5% of cases) or acquired. The cause of congenital pathology can be dysplastic disorders in the structure of segments of the spine, intrauterine anomalies in the structure of the skeleton during its formation (for example, the absence of any rib or, conversely, the presence of an additional one).
The main causes of acquired deformity are most often associated with daily poor posture. Look at a modern teenager: he has to carry a heavy briefcase, sits at his desk in the wrong position for half the day (slouching and bending in different directions from fatigue, and the optimal height of the desk and chair is not always used), and when he comes home, instead of resting, he plays on the computer, sitting bent over for a long time.
Also, deformation of the spinal column can occur due to improper development of the child’s body (with unequal leg lengths; as a result of the development of Scheuermann-Mau disease or rickets; with muscle damage and weakness after polio), with cerebral palsy. Girls often develop postural kyphosis; it is provoked by disturbances in the development of skeletal muscles and ligaments of the spinal column. Another group of causes of spinal curvature are previous injuries.
Forecast
Scoliosis that appears for the first time in a 6-year-old child usually progresses quickly, and curvature appears early. It is not easy to completely cure the disease, especially if the parents did not seek help in a timely manner. If the disease began at the age of 10 years or older, the prognosis is more favorable. In this case, scoliosis usually does not progress so quickly; with timely treatment, there is every chance of a full recovery. Young people suffering from spinal scoliosis have concessions or are completely exempt from military service.
In particularly complex and advanced cases, children may experience irreversible consequences:
- Serious disturbances in the functioning of internal organs
- Chest deformities
- Pronounced asymmetries of the pelvis
- Muscular dystonia
- Breathing problems
- Formation of a hump in the rib area
Diseases of the children's spine.
Pediatric orthopedics studies the etiology and pathogenesis, clinical course and diagnosis of congenital and acquired deformities of the organs of movement and support, including prevention and treatment with restoration of function.
Interpreting signs of deformation or deviations from the normal development of the spine in children at different ages of life is not always a simple task.
In a newborn, the spine has the shape of a gently curved arc, i.e. uniform kyphosis: in the supine position on a flat surface, the spine becomes straight. At 3-4 months of life, the child raises and holds his head, tilting it back; as a result of balancing the occipital and scalene muscles, physiological cervical lordosis develops. At 6-7 months, the child sits, the spine is easily mobile and under the influence of gravity of the head, shoulder girdle, viscera, stable lordosis and balancing by the back muscles, thoracic kyphosis is formed. At 8-9 months the child begins to stand, 10-12 months to walk, and due to the muscles that flex the hip, the pelvis tilts forward, dragging the lumbar part of the spine. The torso in an upright position is balanced by the gluteal muscles and back muscles - a physiological lordosis of the lumbar spine is formed.
The physiological curvatures of the spine in the sagittal plane, which are characteristic of the adult spine, which appeared by the end of the first year of life, continue to develop and are individually formed during the growth of the child by the age of 17-22. Orthostatic, i.e. The vertical position of a person determines statics and posture. External conditions, daily routine, nutrition, physical overload during sports, past illnesses, as well as everything that introduces an imbalance into the balanced state of the muscular-ligamentous “framework” and spine have a great influence on the formation of posture. As a result, correct or pathological posture is formed.
Kyphosis is a curvature of the spine in the sagittal plane with a convexity posteriorly. There are upper thoracic, lower thoracic, lumbar and total kyphosis.
Congenital kyphosis is observed extremely rarely and is localized in the thoracic and upper lumbar region. The deformity is detected early - in the first half of life, as soon as the child begins to sit. As the child grows, the deformity increases noticeably, proceeds painlessly and without neurological symptoms, and reaches pronounced proportions by the time of puberty. The child's growth is stunted. If deformity is detected, back massage and corrective gymnastics are used, and as the process progresses, surgical fixation of the spine is performed.
Acquired kyphosis can be the result of rickets, osteochondropathy, and compression fractures of the vertebral bodies.
Rachitic kyphosis is a consequence of general muscle hypotonia in severe rickets. Develops quickly as soon as the child begins to sit. Rachitic kyphosis is characterized by a uniform posterior curvature of the lower thoracic and lumbar spine. Therapy for such a condition is complex: it is, first of all, the treatment of rickets, mandatory fixation of the child in a special crib, and conducting massage courses to strengthen the muscles of the back, abdomen, and limbs.
Lordosis is a curvature of the spine in the sagittal plane with a convexity forward. Physiological lordosis of the cervical and lumbar spine is the result of the formation of a person’s orthostatic position. Pathological or excessive lordosis is localized mainly in the lumbar spine and may be the result of pathological changes in the lumbar vertebrae and surrounding tissues of a congenital (spondylolysis and spontaneous spondylolisthesis, wedge-shaped vertebrae) and acquired nature. Among the latter deformities, it most often develops as a compensatory curvature when the process is localized in another part of the spine (kyphosis of the thoracic region, round back), with deformation of the lower extremities, dysfunction of the muscles of the trunk and limbs (coxa vara, ankylosis of the hip joint in a vicious position, congenital dislocation of the hip , weakness of the gluteus maximus muscles and hyperfunction of the hip flexors), etc. Congenital lordosis in older children with a latent course can manifest itself as rapid fatigue and pain in the lower back. Compensatory lordosis in children is most often asymptomatic.
When treating lordosis, it is first necessary to eliminate the main cause that caused the development of pathological lordosis. A special complex of therapeutic exercises, massage, and physiotherapy are recommended.
Scoliosis is the most common type of deformity in children. Scoliosis is a curvature of the spine in the frontal plane, caused by pathological changes in the spine and paravertebral tissues, prone to progression of deformation with static-dynamic disorders and functional changes in internal organs. Based on the etiological factor, congenital and acquired scoliosis are distinguished. Congenital scoliosis - the basis of its origin are anomalies in the development of the spine and ribs (accessory, wedge-shaped vertebrae and hemivertebrae, synostosis of the spinous processes, accessory ribs), dysplasia of the lumbosacral spine, which defines the concept of “dysplastic scoliosis”.
Acquired scoliosis is more often expressed as signs of other diseases. Static scoliosis is observed with shortening of the lower limb, unilateral congenital dislocation of the hip, contractures of the hip and knee joints. Neurogenic and myopathic scoliosis occurs due to imbalance of the back muscles, with neurofibromatosis, syringomyelia, deforming muscular dystonia, rickets. Scoliosis is known due to extensive post-burn scars of the torso, diseases and operations of the chest cavity and chest organs. Scoliosis can be caused by tumors of the spine and paravertebral localization.
Metabolic disorders are often accompanied by the development of scoliosis.
Idiopathic scoliosis is a special, most common form that manifests itself as an independent disease. In the pathogenesis of scoliosis, great importance is attached to degenerative-dystrophic processes in the epiphyseal cartilage and the disc itself, epiphysiolysis of the discs under the active influence of the neuromuscular system. When viewed from the front, pay attention to posture; it is possible to identify a forced position of the head and asymmetry of the face, different levels of the shoulder girdle, deformation of the chest, deviation of the navel from the midline and different levels of the iliac crests. When viewed from behind, one shoulder girdle is higher than the other, the scapula on the concave side of the spinal curvature is close to the spinous processes and is located below the opposite one, asymmetry of the chest and costal hump, and asymmetry of the waist triangles are revealed. When viewed from the side, the severity of kyphosis and the size of the costal hump are noted. In addition to the examination, the specialist doctor also evaluates the mobility of the spine and the strength of the back muscles. The diagnosis of scoliosis is made after consulting an orthopedist with all the necessary tests and an x-ray examination of the spine with the pelvis captured in the anteroposterior direction with the patient standing and lying down and a profile picture in the lying position.
Based on localization, the following types of scoliosis are distinguished: cervicothoracic; chest (can quickly progress with severe functional disorders of breathing and the cardiovascular system); thoracolumbar (tends to progress with impaired respiratory function and cardiovascular system, accompanied by pain), lumbar (characterized by a mild course, rarely gives severe degrees of deformation); lumbosacral, in which the pelvic bones are included in the arc of curvature, creating a misalignment with a relative lengthening of one leg (may be accompanied by pain); the combined type of scoliosis is characterized by the presence of two primary arcs of curvature (it is stable). According to the severity of scoliosis, scoliosis is classified into first, second, third and the most severe fourth degree.
The progression of scoliosis depends on the age of the patient, the type and degree of deformity. An intense increase in deformation is observed during the period of rapid growth of the child, reaches a maximum during puberty, in girls at 11-13 years old, in boys at 14-16 years old, and usually ends when growth stops. For the most part, scoliosis that manifests itself before 6 years of age has an unfavorable course; it is more favorable after 10 and especially after 12 years of age. With pronounced progression, scoliosis is classified as decompensated, without a tendency to progression or with slight progression over a long time - as compensated. Children with compensated scoliosis of initial degree should be treated in a clinic and at home, with a slowly progressive course - preferably in specialized boarding schools, with intensive progression in an orthopedic hospital.
Treatment of scoliosis is aimed at stabilizing the existing curvature, preventing its progression and compensating for scoliosis by increasing the stability of the spine and developing an orthostatic position with restoring the balance between the curvature of scoliosis.
Treatment consists of a set of measures that include reducing the static load on the spine and organizing the correct motor mode in a preschool institution, school and at home. In this case, it is necessary to eliminate the causes that contribute to spinal deformation: prolonged sitting, incorrect position in bed, incorrect posture when standing, carrying heavy objects in one hand, etc. It is necessary to carry out a complex of therapeutic exercises (a complex of therapeutic exercises is compiled by a specialist in physical therapy individually for each patient or groups of identified patients) and massage courses, physiotherapy sessions. Along with this, sports games with a ball, swimming, and skiing are recommended.
Practice shows that conservative treatment complexes have a beneficial effect on the correction of scoliosis.
Preventive focus is one of the main links in pediatric orthopedics. Early diagnosis and treatment eliminate the progression of deformities and prevent dysfunction of the organs of support and movement. This determines the main task of the orthopedist and pediatric surgeon together with the pediatrician.