- How often do malignant tumors of bone and cartilage tissue occur?
- Risk factors for the development of malignant tumors of bone and cartilage tissue
- Diagnosis of tumors of bone and cartilage tissue
- Treatment of bone and cartilage tumors
- Survival of patients with bone and cartilage tumors
- What happens after treatment is completed?
There are primary and metastatic (secondary) tumors of bone and cartilage tissue.
Primary tumors arise directly from bone or cartilage, and metastatic lesions are observed when other tumors (for example, lung, breast, prostate cancer, etc.) spread to the bone.
Benign tumors of bone and cartilage tissue include: osteoma, osteoid osteoma, osteoblastoma, osteochondroma, hemangioma and chondromyxoid fibroma.
These tumors do not metastasize and, as a rule, are not life-threatening for the patient. Surgical removal of the tumor is the only treatment method that results in a complete recovery for patients.
Osteosarcoma (osteogenic sarcoma) is the most common primary malignant bone tumor (35%).
Most often, osteosarcoma is detected between the ages of 10 and 30 years, but in 10% of cases the tumor is diagnosed at the age of 60-70 years. Osteosarcoma occurs very rarely in middle age. Men get sick more often than women. Osteosarcoma most often affects the upper and lower extremities, as well as the pelvic bones.
More detailed information about osteosarcoma is presented in the section “Malignant tumors in children.”
Chondrosarcoma develops from cartilage cells and ranks second among malignant tumors of bone and cartilage tissue (26%).
It is rarely detected in persons under the age of 20 years.
After age 20, the risk of developing chondrosarcoma increases until age 75. The tumor occurs with equal frequency in men and women.
Chondrosarcoma is usually found in the upper and lower extremities and pelvis, but can also affect the ribs and other bones.
Sometimes chondrosarcoma develops as a result of malignant degeneration of a benign osteochondroma tumor.
Ewing's sarcoma is named after the doctor who described it in 1921. Most often, the tumor occurs in the bone, but in 10% of cases, Ewing's sarcoma can be found in other tissues and organs. It ranks third in frequency among malignant bone tumors. The long tubular bones of the upper and lower extremities are most often affected, less commonly the pelvic bones and other bones. Ewing's sarcoma is most often diagnosed in children and adolescents and rarely in people over 30 years of age.
Fibrosarcoma and malignant fibrous histiocytoma (6%) develop from the so-called soft tissues, which include ligaments, tendons, fatty tissue and muscles.
Typically, these tumors are detected in middle and old age.
The upper and lower extremities and jaw are the most common sites for fibrosarcoma and malignant fibrous histiocytoma.
Giant cell tumor of bone can be either benign or malignant.
The most common type of tumor is a benign one.
10% of giant cell bone tumors are malignant, resulting in metastasis to other parts of the body, as well as frequent local recurrence after surgical removal.
Typically occurs on the upper and lower extremities of young and middle-aged adults.
Chordoma (8%) occurs at the base of the skull or in the vertebrae.
Surgery and radiation therapy are complicated due to the close proximity of the spinal cord and vital nerves. After treatment, patients should be closely monitored, since repeated growth (relapse) of the tumor is possible after many years.
Non-Hodgkin's lymphomas (lymphosarcoma) usually develop in the lymph nodes, but sometimes can primarily affect the bone.
Multiple myeloma arises from plasma cells in the bone marrow and is not a primary bone tumor.
Sometimes the process is localized in only one bone, but usually multiple lesions of bone tissue are observed.
How often do malignant tumors of bone and cartilage tissue occur?
Primary malignant tumors of bone and cartilage tissue account for less than 0.2% of all forms of cancer.
In Russia in 2002, 2218 cases of malignant tumors of bones and cartilage tissue were identified.
The incidence rate was 1.6 per 100 thousand population.
The maximum incidence rate (4.0 per 100 thousand) was registered in the age group of 75-79 years.
The lifetime risk of developing malignant tumors of bone and cartilage tissue is 0.12%.
It is estimated that 2,440 cases of these tumors may be detected in the United States during 2004.
Bone cancer
Among all malignant tumors, the percentage of tumors of bone structures is low. Primary bone tumors account for less than 1% of all human malignancies. Bones can also be affected as a result of metastasis from other organs and systems of the body. However, metastatic bone cancer occurs four times more often than the primary tumor.
Bone cancer can occur at any age, but most often it affects teenagers and people in their 20s and 30s. It most often occurs between the ages of 15 and 40 years. Males are more susceptible to this pathology.
The latest methods of plastic and reconstructive surgery sometimes make it possible to replace significant defects in bones and joints after removal of tumors, which leads to more successful rehabilitation of patients.
Risk factors for the development of malignant tumors of bone and cartilage tissue.
Different forms of cancer may have their own risk factors. The presence of one or more risk factors does not necessarily mean the development of a tumor. Thus, most patients with tumors of bones and cartilage do not have obvious risk factors.
Below are selected factors that increase the likelihood of developing malignant tumors of bone and cartilage tissue.
Inherited genes. In some patients with osteosarcoma, the occurrence of a tumor can be explained by the presence of hereditary factors. Li-Fraumeni syndrome predisposes to the development of various tumors, including breast cancer, brain tumors, osteosarcoma and other types of sarcomas.
Retinoblastoma is a rare eye tumor in children. 6-10% of retinoblastomas are explained by hereditary factors. Children with a hereditary form of the tumor have an increased risk of developing osteosarcoma. Radiation therapy for retinoblastoma also increases the risk of osteosarcoma of the skull.
Paget's disease can affect one or more bones and is considered a precancerous disease. This disease occurs most often in people over 50 years of age. In Paget's disease, bones thicken but become brittle, which can lead to fractures. In 5-10% of cases, bone sarcomas (usually osteosarcomas) develop against the background of severe Paget's disease.
Multiple exostoses (overgrowth of bone tissue) increase the risk of developing osteosarcoma.
Multiple osteochondromas are formed by bone and cartilage tissue.
Some people inherit an increased incidence of multiple osteochondromas, which increases the risk of osteosarcoma.
Multiple enchondromas develop from cartilage tissue and predispose to an increased risk of chondrosarcoma formation, although this risk is small.
Radiation may increase the risk of developing bone tumors. However, ordinary X-ray examination does not pose a danger to humans.
On the other hand, high doses of radiation used to treat other tumors may increase the risk of malignant bone tumors.
Thus, radiation therapy at a young age, as well as doses above 60 Gray, increases the risk of bone tumors.
Exposure to radioactive substances (radium and strontium) also increases the risk of developing bone tumors as they accumulate in bone tissue.
Non-ionizing radiation in the form of microwave and electromagnetic fields arising from power lines, mobile (cellular) phones and household appliances is not associated with the risk of bone tumors.
Symptoms of bone cancer
Tumor formations of bone tissue are characterized by a triad of clinical manifestations:
- pain reaction;
- formation in the form of a tumor;
- change in the function of a nearby joint.
Pain is the first symptom of most bone tumors. Primary tumors are characterized by constant, growing pain that tends to intensify, especially at night. This manifestation can be relieved with painkillers for a short period of time.
This is followed by the appearance of a palpable formation. Most often, a dense neoplasm is felt; it does not shift and increases in size. Later, the function of the adjacent joint is impaired.
In later stages of the disease, you may experience:
- weakness, loss of appetite;
- aversion to certain smells and foods;
- increased body temperature;
- cachexia (exhaustion);
- pathological fractures;
- lethargy, adynamia, fatigue from light exertion;
- increase in local temperature over the lesion.
The characteristic clinical signs of various types of bone cancer depend on the location of the formation, its size, involvement of nearby anatomical structures in the process, and metastasis. The most striking symptoms occur when the bones of the skull, spine, and pelvis are affected.
Diagnosis of tumors of bone and cartilage tissue
SIGNS AND SYMPTOMS OF THE DISEASE
Pain in the affected bone is the most common symptom of bone and cartilage tumors. At first, the pain is not constant and worries more at night or when walking in case of damage to the lower limb. As the tumor grows, the pain becomes constant.
The pain increases with movement and can lead to lameness if there is a tumor in the lower extremity.
Swelling in the area of pain may take several weeks to appear. Sometimes the tumor can be felt with your hands.
Fractures are uncommon and can occur both in the area of the tumor itself and in the immediate vicinity of it.
General symptoms occur during a widespread process and are expressed in the form of weight loss and increased fatigue.
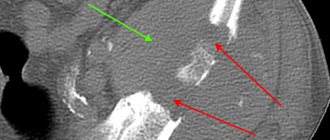
A standard X-ray will most often detect a bone tumor, which may appear as a cavity or additional growth of bone tissue.
Computed tomography (CT) (sometimes with the additional injection of a contrast agent) makes it possible to identify tumors of the shoulder girdle, pelvic bones and spine.
Magnetic resonance imaging (MRI) is especially useful for lesions of the spine and spinal cord.
Radioisotope bone scanning using technetium can detect both the extent of local tumor spread and damage to other bones. This method is more effective compared to standard x-ray examination of bones.
A biopsy (taking a piece of tumor for examination) is mandatory, as it gives the right to confirm or exclude tumor damage to bone or cartilage tissue. In this case, a biopsy can be performed with a needle or during surgery.
After a detailed examination, the stage of the disease is determined.
Depending on the prevalence of the process, stages can be established - from I to IV.
In addition, examination under a microscope makes it possible to determine the degree of malignancy of the tumor.
Mature tumors have a low degree of malignancy, moderately differentiated tumors have an intermediate degree of malignancy, and poorly differentiated (immature) tumors have a high degree of malignancy.
Undifferentiated (most immature) tumors are the most aggressive.
Stages of bone cancer
To determine the stage of bone cancer, the following indicators are used:
- size of the pathological focus;
- damage to the lymph nodes;
- damage to internal organs by metastases;
- degree of differentiation (malignant changes in cells).
This classification is used for all low-quality tumors of the bone skeleton, excluding lymphomas, myelomas, superficial osteosarcomas and chondrosarcomas.
The following stages of the disease are distinguished:
Stage I - has grades A and B: A - the diameter of the formation is up to 8 cm, there is no damage to the lymph nodes and organs, a high or medium degree of tumor differentiation; B – the size of the pathological focus is more than 8 cm, there are no metastases, the degree of differentiation is similar to stage A;
Stage II - has grades A and B: A - lesion up to 8 cm, no metastases, degree of differentiation is low or absent; B – formation larger than 8 cm, metastasis to both lymph nodes and internal organs is not observed, differentiation is similar to stage A;
Stage III – the degree of malignancy (cell differentiation of formation) can be any;
Stage IV - has grades A and B: A - the degree of differentiation can be of any nature, the diameter of the lesion is variable, the involvement of nearby lymph nodes without involving internal organs in the process; B – the diameter of the lesion and the degree of differentiation are any, metastasis to the lymph nodes, the pathological process is observed to involve internal organs.
The degree of malignancy is described by the G index - the higher this indicator, the less differentiated the tumor cells and, accordingly, the more malignant it is.
Classification of bone cancer according to the degree of malignancy (differentiation) and the corresponding stages:
- G1 – highly differentiated;
- G2 – moderately differentiated;
- G3 – poorly differentiated;
- G4 – undifferentiated.
Treatment of bone and cartilage tumors
Surgery is the most important treatment for bone and cartilage tumors. The goal of surgery is to remove the entire tumor within healthy tissue. If a tumor occurs in the pelvic area, surgical intervention may be difficult due to the nearby vital organs.
If 10 years ago the appearance of a malignant tumor on a limb led to the loss of the affected limb, now there is a tendency to preserve the limb.
Part of the affected bone may be removed and the defect replaced with another bone or a metal prosthesis to preserve limb function.
If the tumor size is significant, chemotherapy or radiation therapy is first performed, and then after shrinking the size of the tumor, preservation surgery is performed.
Amputations (removal of a limb) are performed infrequently. In the postoperative period, a prosthesis is made for the patient.
In case of metastatic lesions of the lungs, operations are sometimes performed to remove tumor nodes.
There are two types of radiation therapy for the treatment of tumors of bone and cartilage tissue: external irradiation and brachytherapy. In external irradiation, the source is located outside the body.
The rays are focused on the tumor area.
Brachytherapy involves the use of radioactive material injected directly into the tumor. This type of irradiation can be used either alone or in combination with external irradiation.
In some patients, especially those with poor general condition, radiation therapy may be the mainstay of treatment.
In patients with Ewing's sarcoma, radiation therapy is the main treatment method.
After non-radical surgery, radiation therapy is prescribed to destroy the remaining part of the tumor.
Radiation may be used palliatively to reduce symptoms of the tumor, such as pain.
During radiation therapy, side effects may occur in the form of skin changes and increased fatigue. These phenomena disappear on their own soon after the end of treatment. When the pelvic area is irradiated, nausea, vomiting and loose stools may occur.
Radiation therapy given to the chest area can cause lung damage, which in turn can lead to shortness of breath.
Radiation in the area of the upper and lower extremities is in some cases accompanied by swelling, pain and weakness. Radiation therapy may worsen the side effects caused by chemotherapy.
Depending on the type of tumor and stage of the disease, chemotherapy can be used as the main or auxiliary (to surgery) treatment.
In this case, a combination of antitumor drugs is used. The most active drugs for these tumors are: methotrexate (in high doses in combination with leucovorin), doxorubicin and cisplatin.
In some cases, chemotherapy is prescribed before surgery to shrink the size of the tumor; in others, immediately after surgery to destroy remaining tumor cells. In patients with extensive spread (metastasis) of the tumor, other antitumor drugs can be used: vincristine, etoposide, dactinomycin, ifosfamide.
Chemotherapy, while destroying tumor cells, also damages normal cells, causing side effects and complications. The severity of side effects depends on the type of drug, total dose and duration of use.
Temporary side effects include: nausea, vomiting, loss of appetite, baldness, and mouth ulcers. A decrease in the number of red blood cells, white blood cells and platelets in the blood as a result of bone marrow damage can cause anemia (anemia), increased susceptibility to infection, and bleeding.
Types of bone cancer
Bone cancer is most often divided into:
- bone-forming lesions;
- cartilaginous tumors;
- tumor formations arising from the bone marrow;
- giant cell tumor;
- other neoplasms.
Bone-forming tumor formations include:
- benign – osteoma, osteoblastoclastoma;
- malignant course – osteosarcoma, parosteal osteosarcoma.
Cartilaginous neoplasms include:
- benign course – chondroma, chondroblastoma, osteochondroma;
- malignant - chondrosarcoma.
Bone marrow neoplasms are combined into a general group:
- Ewing's sarcoma;
- reticulosarcoma of bone;
- bone lymphosarcoma;
- myeloma.
Other tumors are considered to be:
- chordoma;
- neurofibroma;
- neurilemmoma.
Osteosarcoma is the most common malignant tumor, accounting for about 60% of all bone cancers. Ewing's sarcoma occurs in 10-15% of cases. Chondrosarcoma accounts for about 10-12%.
Patient survival prognosis
With timely diagnosis and timely treatment, the 5-year survival rate of patients with osteosarcoma reaches 70%, and for primary lymphoma it is more than 60%. For chondro- and fibrosarcoma, the 5-year survival rate is about 70%.
Our experience shows that treating bone cancer is possible!
The developed and tested methods of our Oncology Center are aimed at curing this disease, reducing its symptoms, preventing the progression of the disease and improving the quality of life!
The Russian-Japanese Oncology Center uses only proven and well-proven methods.
Diagnostics
Small benign tumors may not cause any symptoms and are often discovered by chance . Primary malignant tumors are often diagnosed at pathological fractures as a result of bone deformation.
In the diagnosis of neoplasms of bones and soft tissues, instrumental studies are used ( radiography, ultrasound, CT ), which give an idea of the presence of a neoplasm and its location relative to other tissues and organs.
Benign tumors differ from cancer in that they have clear boundaries, while the malignant process is characterized by growth into nearby tissues.
If cancer is suspected an MRI study is highly effective , which allows you to determine the nature of the tumor and helps doctors choose the key treatment method.
All methods for diagnosing cancer, including laboratory tests, are available to patients at our medical center in Kyiv. biopsy can be performed for subsequent histological examination.