The buttocks, as the gluteus maximus muscle is called (musculus gluteus maximus), many of us rarely attach importance to, and do not consider these muscles important, and remember them only when the swimming season comes, and the need arises to wear swimming trunks and, moreover, attention is paid form, not function. The gluteal muscles serve several functions beyond just being an attractive seat cushion, and if these muscles are weakened, then a lot of problems arise. Well, if we sit all the time during the day (at work, at home, while eating or watching TV), then what kind of muscle strength can we talk about?
Nature made this muscle large enough not only for the sake of beauty. The gluteus maximus muscle (“MGM”) is the largest and one of the strongest muscles in the human body. The gluteus maximus muscle is the most superficial of the three gluteal muscles and forms most of the shape and appearance of the buttocks. The gluteus maximus muscle runs along the crest of the pelvic bone and attaches to the posterior aspect of the proximal femur and to the iliotibial ligament, providing a connection between the trunk and lower extremities.
The large size of this muscle is one of the most characteristic features of the human muscular system. According to most researchers, humans evolved from ape-like ancestors about two million years ago on the vast savannah of Africa. It is believed that natural selection favored the survival of animals that could escape. Over time, evolution consolidated the anatomical features that allowed humans to run long distances, and the enlargement of the gluteus maximus muscle may have played a decisive role in this process.
Functions of the gluteus maximus muscle.
The gluteus maximus muscle is very important in performing activities such as standing, walking, and running. The function of the muscle in these activities is to participate in straightening the leg, bringing the torso into a vertical position, abducting and adducting the hip in accordance with our body, rotating the hip from and to the center of the body and stabilizing the pelvis. This muscle may also play a role in stabilizing the knee during extension.
During standing up, for example, the gluteal muscle plays an important role in hip extension and pelvic stabilization. During running, this muscle provides stabilization to the torso and helps extend the hip when accelerating and slow down the leg when stopping.
Thus, weak gluteus maximus muscles reduce the ability to perform many of our daily activities effectively and safely. Muscle weakness can make it difficult to perform certain movements that require these muscles, such as standing up, sitting, walking, or running. Sometimes weakness of the gluteal muscles can be associated with back, knee and hip pain.
Muscles of the outer thigh
This includes one large muscle, the structure and functions of which are discussed below.
Tensor fascia lata
A flattened and elongated muscle fiber that rotates the hip and pushes it forward. It connects with the anterior iliac spine at the beginning, at the end it turns into a long tendon, and extends to the middle part of the area under consideration.
The muscle ensures full physical activity of the limb and determines the roundness of the femoral region.
The lower limbs play a vital role in ensuring normal life activities. Thanks to the successful fulfillment of their functional duties, the body moves in space, maintains balance, and a person can exist normally in society.
The anatomical structure of the legs is complex. Thanks to the coordinated interaction of all muscle and nerve fibers, they have the ability to carry out various types of movements.
Studying the structural features of the thigh muscles allows doctors to competently and successfully carry out complex surgical interventions, surgically restore the integrity of the limb, and restore its motor abilities.
How do you know if your gluteus maximus muscles are weak?
For example, here is a simple and quick test that will help determine if you have weak gluteal muscles.
Lie on your back with your knees bent at least 90 degrees. Squeeze your gluteal muscles. Slowly lift your hip off the floor and then straighten your right knee so that your thighs are parallel. Try not to change the level of your pelvis or rotate your hips. If the pelvis deviates or rotates to one side when the leg is extended, then there is definitely weakness in the gluteal muscle. But this test should not be performed by women until at least 6 weeks after giving birth.
Exercise therapy doctors can use additional manual and dynamic diagnostic methods to determine gluteal muscle weakness:
- Manual diagnostic techniques include observing whether the exercises are performed correctly, whether there are any displacements in the movement, or whether other muscles are compensatory in the movement.
- Dynamic methods include digital analysis of video of movement performance, which allows the exercise therapist to examine the movement in detail. Such video analysis allows the physical therapy doctor to evaluate the work of the gluteal muscles in the kinetic chain, to observe the function of the pelvis and lower extremities dynamically, throughout the entire gait cycle.
Symptoms of trauma.
A characteristic and primary symptom for all types of tendon injuries is the appearance of sudden severe pain. The following signs are added to it:
- redness and swelling in the area of injury
- increased sensitivity at the site of injury
- muscle cramps
- hemorrhage
- characteristic crunching sound at the time of injury
- limited movement of the injured limb
- complete ruptures are characterized by the appearance of dips when walking
What can you do to increase glute muscle strength?
There are many exercises you can do that will not only improve the shape and tone of your glutes, but also improve their function.
One leg bridge
Lie on your back with your knees bent at least 90 degrees. Squeeze your gluteal muscles. Slowly lift your hip off the ground and then straighten your right knee so that your thighs are parallel. Keep your pelvis level and don't rotate your hips. Hold for 10 seconds and then return to the starting position. Repeat this exercise on your left leg. Repeat the exercise 10 times. Note: This exercise should not be performed by women until at least 6 weeks after giving birth.
Lying hip extension
Lie on your stomach, 1-2 pillows under your hips. Bend your knee 90 degrees. Squeeze your glutes and slowly lift your heel toward the ceiling. Don't let your back sag. Hold your leg in this position for 10 seconds and then return to the starting position. Repeat 10 times. Note: if you have back pain, then this exercise can only be performed under the supervision of a physical therapy doctor.
Channels in muscle tissue
In the muscles of the zone under consideration, between the layers of the fascia lata - superficial and deep - there is a femoral canal. There are two holes in it:
- The upper one passes through the broad medial muscle and the long adductor muscle, its lower end connects to the lower adductor foramen.
- The lower (deep) is directed inside the inguinal ligament, separated by it in front, by the femoral vein on the outside and by the ridge vein in the back.
Sensitive nerve fibers and large blood vessels (femoral vein, artery of the same name and saphenous nerve) pass through them.
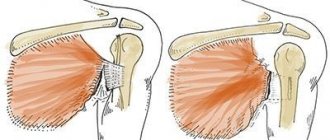
Shoulder abduction
The shoulder abductor muscles cross the sagittal axis of rotation in the shoulder joint and are located lateral to it. The humerus is abducted by the following muscles:
1) deltoid and
2) supraspinatus.
The deltoid muscle (see Fig. 54) begins
from the clavicle (anterior part of the muscle), acromion (middle part) and the spine of the scapula (posterior part), and
is attached
to the deltoid tuberosity of the humerus.
The shape of this muscle somewhat resembles an inverted Greek letter “delta,” which is where its name comes from.
The function of the deltoid muscle is as follows. If the front and back parts alternately work, then the upper limb moves forward and backward, i.e. flexion and extension.
Features of adductor training
We offer recommendations that will help increase the effectiveness of adductor muscle training:
- Work your adductors on the same day as your glutes workout. This will avoid shortening the adductors;
- After your workout, do some light stretching. This will also help avoid shortening and improve the ductility of the fibers;
- To pump up the hip adductors, use high weights and low repetitions (for men);
- To strengthen the adductors and get rid of cellulite , work with light weights for a large number of repetitions (for women);
- Women are allowed to do stretching, yoga, and Pilates on their free days to improve the flexibility of the adductors.
Sample training program for the hip adductors
We recommend combining training of the adductors with training of other muscles of the lower body.
Example:
- Warm up on a jump rope or treadmill for 5 minutes;
- Squats (4/6-8);
- “Wide” leg press in the simulator (3/10-12);
- Forward lunges with kettlebells (3/10-12);
- Leg abduction in the simulator (3/10-12);
- Calf raises in a vertical machine (3/15-20).
The considered example of an activity is more suitable for men. Girls can adapt the training to suit themselves, for example, replacing classic squats with a plie variation. After working out your lower body, we recommend doing some simple stretching.
Clinical picture
In approximately 50% of cases, it is preceded by local trauma - severe eversion of the posterior segment.
Women over 40 years of age and younger athletes are more often affected.
- Patients often do not seek help in the early stages (in the 1st or acute phase), because symptoms are mild.
- Patients usually present in stage 2 or subacute phase, with diffuse swelling and heat in the medial ankle and along the tendon. Patients experience difficulty or a feeling of instability when lifting the heel on the affected side, and the heel does not supinate when lifting it off the surface.
- In stage 3 or the chronic phase, the patient notices a gradual decrease in the height of the longitudinal arch, the development of a flat foot on one side, and fatigue in the lower limb when walking. When viewed from behind, there is excessive abduction of the forefoot (too many toes sign). In severe cases, loss of the longitudinal arch, eversion of the calcaneus. Excessive wear on the medial heel of a shoe.
Muscles that flex and extend the hip
To carry out these movements, there are six functional muscle groups in the hip joint.
Hip flexion. The muscles that produce flexion of the thigh in the hip joint include the muscles that cross the transverse axis of this joint and are located in front of it.
These include: 1) iliopsoas , 2) sartorius , 3) tensor fascia lata muscle; 4) pectineus; 5) rectus femoris muscle
Hip extension In hip extension, muscles take part that also cross the transverse axis of the hip joint, but are located behind it.
These muscles go both from the pelvis to the thigh and from the pelvis to the lower leg. These include: 1) gluteus maximus; 2) biceps femoris; 3) semitendinosus; 4) semimembranosus; 5) adductor magnus
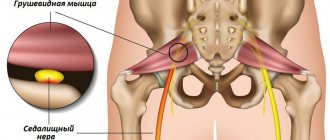
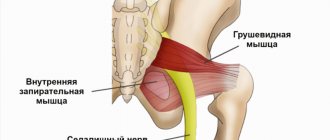
Hip abduction. The hip abductor muscles cross the sagittal axis of the hip joint and are located on its lateral side.
They are attached mainly to the greater trochanter. These muscles include: 1) gluteus medius; 2) gluteus minimus; 3) piriformis; 4) obturator internus; 5) gemini;
6) tensor fascia lata muscle
Hip adduction Hip adduction is carried out by muscles that cross the sagittal axis of the hip joint and are located medial to it.
These include: 1) comb; 2) thin; 3) long adductor; 4) short adductor; 5) adductor magnus.
Supination of the hip The muscles that supinate the hip, except for the iliopsoas, cross obliquely the vertical axis of the hip joint.
The iliopsoas muscle supinates the thigh due to the special location of the lesser trochanter (not only anteriorly, but also medially). The muscles that supinate the thigh include: 1) iliopsoas; 2) quadratus femoris; 3) gluteal muscles, of which the medius and minimus supinate the thigh only with their posterior bundles; 4) sartorius; 5) obturator internus and obturator externus; 5) pear-shaped; 6) twin.
Pronation of the hip The group of pronator muscles of the hip is relatively small.
These include: 1) the tensor fascia lata muscle 2) the anterior bundles of the gluteus medius muscle 3) the anterior bundles of the gluteus minimus muscle 4) the semitendinosus, semimembranosus and gracilis muscles. Circular movement of the hip In the hip joint, all muscle groups located around it produce, acting in turn.
Knee joint: structure, shape, movements, blood supply. Muscles that produce movement in a joint.
Formed by the condyles of the femur and the articular surfaces of the tibia, the patella. Condylar compound joint. Possible movements: flexion, extension, rotation.
Ligaments – anterior and posterior cruciate, tibial and fibular collateral ligaments.
It consists of the following formations: 1) bones - femur, tibia and patella, 2) muscles, 3) nerve endings and blood vessels, 4) menisci, 5) cruciate ligaments.
The knee joint consists of the femur and tibia, these tubular bones are connected to each other by a system of ligaments and muscles, in addition, in the upper part of the knee there is a rounded bone - the patella or kneecap.
The femur ends in two spherical formations - the femoral condyles and, together with the flat surface of the tibia, form a connection - the tibial plateau.
The patella is attached to the main bones by ligaments and is located in front of the kneecap.
Its movements are ensured by sliding along special grooves on the femoral condyles - the pallofemoral recess. All 3 surfaces are covered with a thick layer of cartilage tissue, its thickness reaches 5-6 mm, which provides shock absorption and reduces thorns during movement.
Connecting components
The main ligaments, together with the bones that make up the knee joint, are the cruciate ligaments.
In addition to them, on the sides there are lateral collateral ligaments - medial and lateral. Inside there are the most powerful connective tissue formations - the cruciate ligaments. The anterior cruciate ligament connects the femur and the anterior surface of the tibia.
It prevents the tibia from moving forward during movement.
The posterior cruciate ligament does the same thing, preventing the tibia from moving posterior to the femur. Ligaments provide connection between bones during movement and help to maintain it; rupture of the ligaments leads to the inability to make voluntary movements and lean on the injured leg.
In addition to the ligaments, the knee joint contains two more connective tissue formations that separate the cartilaginous surfaces of the femur and tibia - the menisci, which are very important for its normal functioning. Menisci are often called cartilage, but in their structure they are closer to ligaments.
Menisci are rounded plates of connective tissue found between the femur and the tibial plateau. They help to correctly distribute the weight of a person’s body, transferring it to a large surface and, in addition, stabilize the entire knee joint.
Knee muscles
The muscles located around the joint and ensuring its operation can be divided into three main groups: 1. anterior group of muscles - hip flexors - quadriceps and sartorius muscles, 2. posterior group - extensors - biceps, semimembranosus and semitendinosus muscles, 3. medial ( internal) group – adductor muscles of the thigh – thin and large adductor muscles.
One of the most powerful muscles in the human body is the quadriceps.
It is divided into 4 independent muscles, located on the front surface of the femur and attached to the kneecap. There, the muscle tendon turns into a ligament and connects to the tibial tuberosity.
The intermedius muscle, one of the branches of the quadriceps muscle, also attaches to the knee capsule and forms the knee muscle. Contraction of this muscle promotes leg extension and hip flexion.
The sartorius muscle is also part of the muscles of the knee joint. It starts from the anterior iliac axis, crosses the surface of the femur and goes along the inner surface to the knee.
There it goes around it from the inside and attaches to the tuberosity of the tibia. This muscle is two-part and therefore participates in flexion of both the thigh and lower leg, as well as in the inward and outward movement of the lower leg.
Thin muscle - starts from the pubic joint, goes down and attaches to the knee joint.
It helps with hip adduction and ankle flexion.
In addition to these muscles, the tendons of the biceps femoris, tendinous, semimembranosus and popliteus muscles pass through the knee joint.
They provide adducting and abducting movements of the lower leg. The popliteus muscle is located directly behind the knee and helps with flexion and internal rotation.