The shoulder joint has a complex structure, which provides it with high mobility in different planes: adduction-abduction, flexion-extension, rotation. But at the same time, the shoulder joint is one of the most vulnerable and unstable connecting structures in the body and is often susceptible to various injuries and diseases.
Let's consider the features of diagnosis and treatment of partial rupture of the tendon of the supraspinatus muscle of the shoulder and find out the most common causes of such damage.
Peculiarities
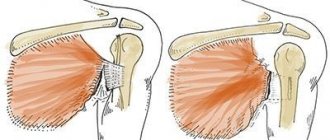
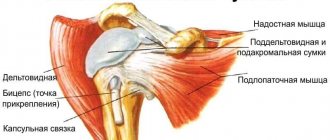
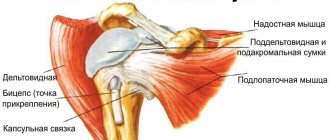
The shoulder joint has a round shape, which provides a high range of motion in it. The necessary strength and stability are factors to prevent the humeral head from protruding from the glenoid cavity. They are provided by the components of the rotator cuff, these include the supraspinatus, infraspinatus, subscapularis and teres muscles, as well as ligaments and tendons. An increase in load is accompanied by an increase in stretching of muscle fibers, which can lead to complete or partial rupture.
Supraspinatus tendon injury
Treatment without surgery or conservatively is usually used for small, non-full-thickness tears. The main goal of conservative treatment is to reduce pain and, if possible, increase the range of motion in the shoulder joint. For this purpose, anti-inflammatory drugs, physical therapy and physiotherapy are used.
Physical therapy can also help the patient prepare for surgery. After a course of physical therapy, there is a noticeable strengthening of the muscles in the shoulder area, and also increased mobility in the joint. Unfortunately, conservative treatment for complete cuff tears is not very effective.
If, despite treatment, there is no improvement within two months, doctors may recommend surgical treatment. According to the latest data from scientists, the most preferred method of treating rotator cuff tears is surgery.
Surgical techniques for cuff repair have undergone significant changes in recent decades. This happened in connection with the introduction of minimally invasive surgery, primarily arthroscopy, into practice.
Arthroscopy has revolutionized shoulder surgery. Arthroscopy, compared to open surgery with a large incision, is a more gentle intervention. Arthroscopy does not damage other muscles that are not affected by the disease, such as the deltoid muscle. An arthroscope inserted into the joint through just a puncture of the skin allows you to see the entire rotator cuff, identify the tear and repair it.
Arthroscopy can also successfully diagnose and treat other associated changes in the shoulder joint. Using special equipment, you can correct the shape of the bones and remove bone growths that lead to damage to the cuff. Special anchors are used to attach the torn cuff to the bone.
The anchor is a small titanium or bioabsorbable (absorbable) screw that is screwed into the bone.
Several strong threads are attached to the anchor, with which the torn section of the cuff is pulled to the bone. The anchor and threads hold the cuff firmly for several months until they fuse with each other.
The use of arthroscopy in rotator cuff repair reduces the amount of surgical trauma, reduces the severity of pain after surgery, and promotes earlier rehabilitation and discharge from the hospital.
Arthroscopic rotator cuff repair is a fairly successful operation with a high rate of good to excellent results and a minimal number of complications.
After surgery, the arm is fixed in an orthosis for several weeks. Therapeutic gymnastics classes begin from the first days. The sutures are removed 12 days after surgery. Discharge from the hospital is possible the next day after surgery.
Long-term inflammation of shoulder components
Long-term inflammation of shoulder components
Determining the causes is a mandatory activity that is carried out during a diagnostic examination and makes it possible to select the most adequate therapeutic tactics and prevent the recurrence of changes.
The best sports clinics and doctors!
Doctor Chechil's Manual Therapy Clinic
Chechil Sergey Vyacheslavovich - Chief physician of the clinic. The main direction is the musculoskeletal system. He has 24 years of medical experience: managing the medical service of a nuclear submarine, managing the special training department of the Paratunka military sanatorium in Kamchatka.
Kovtun Yuri Vadimovich - neurologist, chiropractor, specialist in the selection and installation of orthopedic individual insoles. Certified Kinesto Taping Specialist.
Clinic video
Clinic website - www.chechil.com
Moscow Scientific and Practical Center for Sports Medicine
Muzykantov Mikhail Konstantinovich - Traumatologist-orthopedist of the traumatology department.
Clinic website - mnpcsm.ru
Family Clinic
Davis Andrey Evgenievich - Orthopedic traumatologist. Doctor of the highest category.
Clinic website - Semeynaya.ru
for the popularization of amateur sports!
Partial rupture
Partial rupture
Depending on the prevalence, an isolated change occurs, affecting only the supraspinatus muscle, or a combined injury, in which several components of the shoulder joint, including bones, change at once.
Signs
A partial full-thickness rupture of the supraspinatus tendon is accompanied by the development of a fairly characteristic clinical picture, including the following symptoms:
- Pain in the girdle area of the upper limb from the side of the changes, which occurs abruptly after an injury or increases gradually against the background of the development of the pathological process.
- Impairment of the functional state, accompanied by the fact that it becomes difficult to raise the arm up.
- Decreased stability, leading to frequent shoulder dislocation (development of habitual dislocation).
- The appearance of inflammatory signs, including redness of the skin of the upper limb girdle, swelling of soft tissues with an increase in shoulder volume, increased pain that can bother a person at rest.
The severity of clinical manifestations depends on the degree of damage to the connective tissue fibers of the supraspinatus tendon.
Rehabilitation
The postoperative period begins with immobilization of the limb in a neutral position using a support bandage. Patients are allowed pendulum movements and strength grasping exercises, which continue for 6 weeks. Passive flexion in the supine position is allowed after 6 weeks. Active exercises begin no earlier than 8-10 weeks. Cross adduction is acceptable from 8 to 10 weeks. From the 12th week you can begin exercises with loads on flexion and internal and external rotation.
Return to physical activity depends on the integrity of the restored area, severity of pain, range of active movements and strength requirements.
Ultrasound
Ultrasound
In order to determine the severity and location of a partial rupture of connective tissue components, an additional objective examination is prescribed. It includes modern techniques that make it possible to assess the condition of internal structures. These include radiography, tomography (layer-by-layer scanning of tissue using X-rays or the effect of magnetic resonance of nuclei), arthroscopy (visual examination using an optical device inserted into the joint cavity), ultrasound (ultrasound examination).
Treatment
Therapeutic measures in case of diagnosed partial rupture of connective tissue components are complex. Conservative treatment is predominantly prescribed, which includes several areas of action:
- General recommendations aimed at limiting functional load. If necessary, the joint is immobilized (immobilized) for the entire period of therapy.
- Prescription of medications including anti-inflammatory drugs, chondroprotectors, vitamins.
- Physiotherapeutic procedures that relieve the severity of chronic inflammation and also accelerate the process of tissue regeneration (healing), these include magnetic therapy, ozokerite, and mud baths.
A more pronounced change in the properties of the connective tissue components is the basis for performing surgery with plastic surgery of the fibers of the connective tissue components. In modern clinics specialized in the treatment of structures of the musculoskeletal system, a low-traumatic technique of arthroscopic manipulation is used.
Diagnostics
A detailed radiological examination is an important diagnostic measure.
Radiography
- In the anteroposterior projection, performed in a vertical position, a “fixed” superior migration is revealed, the distance between the head of the humerus and the acromion process is measured (normally up to 11 mm, less than 6 mm - a gap, surgical treatment is required).
- The tangential projection allows the assessment of degenerative changes in the joint.
- “Y” projection allows you to evaluate the morphology of the acromial arch.
- The axillary view demonstrates the concentric change in contours and illustrates the asymmetry of the joint.
MRI is the best way to evaluate the condition of muscles and tendons. On medial muscle sections, fatty degeneration of muscle tissue can be detected.
In Europe, the method of contrast CT is popular, used for the same purpose.
The development of ultrasonography has allowed dynamic assessment of the rotator cuff. It is easy to compare the affected joint with the opposite one by changing its position.