Osteochondrosis of the cervical spine occurs more often than any other - it spares neither the elderly nor young people over the age of 20. People around him complain about its manifestations every day, attributing their sensations either to magnetic storms, or to energy vampires, or to more prosaic, but still far from the truth, explanations.
The localization of the disease in the cervical region, which includes 7 vertebrae, is explained by the fact that the intervertebral discs in this area are the thinnest. Therefore, their drying out and destruction much faster leads to pinched nerves and abrasion of the vertebral bones - after all, the distance between the bones is already small. Also affected is the poor development of the neck muscles, which modern people use minimally.
Alas, the non-inflammatory process in the spine goes unnoticed for a long time until degeneration of the intervertebral discs moves to the second stage and pain becomes a constant companion. But even this alarming sign is often ignored by people, attributing it to fatigue, or even getting used to it as an everyday “background”. Let’s figure out why you can’t ignore a headache, whether your mother was right when she said “don’t turn your head,” and how to treat osteochondrosis of the cervical spine in order to bring the chronic disease into stable remission.
Symptoms of osteochondrosis of the cervical spine
Discomfort from cervical osteochondrosis extends to the head, neck and limbs of the shoulder girdle. At the initial stages, no special complaints are observed - usually patients simply begin to have a stiff neck more often, which does not seem surprising at all during office work. Gradually, the gap between the vertebrae decreases, the load on the ligaments, muscles of the neck, shoulders and back increases, and the blood supply to the brain and spinal cord deteriorates. This entails a whole chain of nonspecific symptoms; a combination of several of them is a good reason to see a doctor.
Osteochondrosis of the 1st degree of the cervical spine
Signs of cervical osteochondrosis at the initial stage include:
- local muscle tension;
- stiffness of movements and a decrease in their amplitude (when turning the head, rotating the shoulders) after a long stay in one position;
- the need to constantly support your head with your hand while sitting to avoid fatigue and discomfort;
- fatigue and frequent headaches;
- increased irritability and chronic fatigue;
- inability to fall asleep quickly due to attempts to get comfortable, to press the pillow in a comfortable way;
- darkening in the eyes, the appearance of “spots” after a load on the cervical spine or during a morning/sharp rise;
- crunching and other extraneous sounds when tilting the head;
- the appearance of the so-called “lumbago” in the area from the back of the head to the shoulder blades;
- decreased sensitivity in the fingertips, tingling sensation in the hands;
- unusual feeling of weakness in the arms, decreased endurance and muscle strength;
- increased blood pressure - arterial hypertension;
- change in voice, hoarseness for no apparent reason, the appearance of snoring, a feeling of heaviness, “swelling” in the head.
Osteochondrosis grade 2 of the cervical spine
- chronic pain syndrome - the head, neck or shoulder may hurt continuously for 2-3 days or longer;
- problems with sleep - it is difficult to fall asleep or wake up, waking up in the middle of the night due to nightmares caused by oxygen deprivation is not uncommon;
- high weather sensitivity;
- the appearance of pain and spasms in muscles and internal organs, especially if it is necessary to maintain the same position for a long time or change it;
- inability to press the chin to the chest and throw back the head without pain;
- falling head syndrome - clearly noticeable pain when trying to sit without supporting your head;
- numbness of the hands (“hands do not obey”), the appearance of pain in the neck with minimal load on the upper limbs;
- tinnitus and black spots before the eyes, dizziness and even fainting;
- the appearance of clamps;
- cardiac dysfunction;
- migraine;
- constant feeling of nausea;
- proliferation of connective tissue (“thick skin”) in the cervical-collar area.
Ignoring the signs of osteochondrosis of the cervical spine is fraught - next to the spine there are nerves and large vessels that are pinched when the vertebrae are displaced. Complications of the disease include:
- paresis (limitation, weakness of movements) and even paralysis of the arms - one- or two-sided;
- intervertebral hernia is a common cause of disability and disability, including the need for a wheelchair;
- vertebral artery syndrome, which causes dizziness and “noise” in the head, 25% leads to ischemic stroke;
- rapid deterioration of memory, cognitive abilities, vision and hearing;
- impaired coordination of movements, which causes difficulties even when traveling in transport.
Diagnosis of MRI of the thoracic spine for back pain syndrome
In diseases of the spine, pain can radiate to any part of the chest, but most often to the region of the costal cartilages, scapular and paravertebral regions. When the thoracic vertebrae are affected, pain can also occur along the anterior surface of the chest and behind the sternum, so it is very difficult to make a diagnosis.
People of all ages get sick, even children. The pain may resemble angina pectoris, biliary colic and other diseases of the internal organs. When looking for the cause of pain, it is necessary to exclude not only angina pectoris, myocardial infarction, dissecting aortic aneurysm, pneumonia, pleurisy, but also spinal diseases.
The main causes of pain identified by MRI examination are the following:
The most common lesions occur in the intervertebral joints, joints of the ribs and spine - joints of the heads of the ribs and costovertebral joints. Pain from such lesions is localized 3-4 cm lateral to the posterior midline, which approximately corresponds to the location of these joints. Referred pain is often observed in the posterior, lateral and even anterior sections of the chest wall.
Signs of arthrosis of the costovertebral joints
Chest injuries predispose to osteoarthritis of the spine; they are especially common in contact sports.
Signs of osteoarthritis
Herniated discs are quite rare in the thoracic spine, which is due to the great stability of this part of the spine. If hernias occur, they often occur below the level of the Th9 vertebra. The main symptom is back pain, radiating to the innervation zone of the pinched root. Large herniated intervertebral discs can compress the spinal cord, which is manifested by lower central paraparesis, impaired sensation in the legs and lower torso, and urinary incontinence.
Osteochondrosis. Disc herniation, hernial sequestration.
Disc protrusion
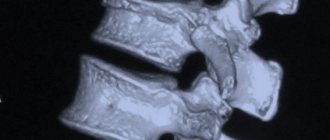
Due to anatomical features, compression fractures of the thoracic spine are most common, both traumatic and pathological, caused by destruction of the vertebrae due to multiple myeloma, metastatic lesions or osteoporosis.
Post-traumatic compression of Th7-Th9, Th11 vertebrae, chr. period, increased thoracic kyphosis
Trauma, compression fracture (acute period)
| Comminuted fracture of the Th11 vertebra | Metastases, pathological fractures of Th9, Th10 vertebrae. Central spinal canal stenosis. |
| Osteoporotic deformity of the Th6 vertebra | Metastases, pathological fracture of the Th10 vertebra. Post-traumatic deformation of the Th2 vertebra. |
Spinal osteomyelitis can be both nonspecific and specific (with brucellosis, tuberculosis, syphilis, typhoid fever). In addition to back pain, general symptoms are observed with osteomyelitis - malaise, weakness, fever. Nonspecific osteomyelitis should be suspected in young people, brucellosis in agricultural workers, tuberculosis in immigrants and prisoners.
Clinical example:
Complaints of severe pain in the thoracic spine. The patient was released from prison, with a history of tbc.
At the Th7-Th8 level, specific tuberculous spondylitis + vertebral bone marrow reconversion.
T1 Sag T2 Sag
T1 Sag T2 Sag
T1 Sag T2 Sag
Т2 Cor Т2 Stir
Т2 Tra
Post-contrast
Spondylitis Th5-Th6; myelitis (Th3-Th6); epiduritis Th5-Th6. Spinal stenosis. Osteochondrosis. Spondyloarthrosis deformans
Deformation and destruction of the vertebrae can be caused by primary tumors of the spine, metastases of tumors of internal organs, as well as tumors of the spinal cord, its roots and membranes.
Extradural space-occupying lesion (Tr vertebra Th7). Spinal stenosis; spinal cord compression.
Multiple metastases involving vertebral bodies and processes, spinal canal stenosis
Hemangiomas of Th5, Th10 vertebrae
The focus of pathological MRS in the anterior-superior parts of the Th12 vertebral body (differential diagnosis between dystrophy /Modic 3 type/ and metastasis.
Intradural extramedullary space-occupying lesion at the level of the T12 vertebra.
Т1 Sag Т2Sag
Post-contrast
Intramedullary space-occupying lesion of the thoracic spinal cord at the Th8 level
Extradural space-occupying formation of the spinal canal at the level of the Th12 vertebra (more likely epiduritis, differential diagnosis with volume)
Т1 Sag Т2Sag
post-contrast
Spinal lesions are often accompanied by myeloma and lymphoma.
Multiple space-occupying formations of the mediastinum and paravertebral soft tissues (possibly a lymphoproliferative process)
structural changes in the bone marrow (myeloma)
Among benign tumors, osteoid osteoma should be mentioned separately. This tumor gives a unique clinical picture - back pain increases after drinking alcohol and decreases after drinking aspirin.
Osteoid osteoma
After radiation therapy for various oncological processes of the spine or internal organs, typical changes in the bone marrow of the vertebrae occur - its depletion (fatty degeneration).
Signs of bone marrow depletion of Th6-Th8 vertebrae (post-radiation changes)
Mostly teenage boys are affected.
B-n Bekhterev
Osteochondrodysplasia (Scheuermann-Mau disease)
Osteochondrodysplasia (Scheuermann-Mau disease), born 1984.
Diastomatomyelia
Butterfly vertebra, scoliotic spinal deformity
Multilevel combined anomaly of the spine
Pain in the thoracic spine is often perceived as pain in the heart, or a person waves his hand: “Oh, I just had a cold, it will go away!” But in fact, pain in the thoracic spine can be a signal of many diseases that we are not even aware of. To exclude a pathological process and, if necessary, begin treatment on time, it is necessary to undergo a full examination. One of the most modern and most reliable methods currently is the chest MRI method.
How to treat osteochondrosis of the cervical spine
To combat osteochondrosis of the cervical spine, pharmacotherapy and physiotherapy are used, as well as massage and hydromassage of the cervical-collar area, therapeutic exercises, swimming, balneological and mud treatments, electrophoresis, ultraphonophoresis, acupuncture, ultrasound, shock wave, laser, ultraviolet irradiation, magnetic and other types of hardware therapy. Symptoms and treatment of osteochondrosis of the cervical spine are significantly different for the stages of remission and exacerbation. For example, massage for osteochondrosis of the cervical spine during the inflammatory process is strictly contraindicated - to begin with, ointments and topical creams are used. In the acute period, it is important to restore blood circulation and tissue nutrition, relieve spasm and improve the patient’s quality of life. Therapy aimed at the regeneration of cartilage tissue and osteophytes is carried out exclusively in remission.
Surgical intervention is used extremely rarely - mainly to eliminate concomitant pathologies, such as hernia, vertebral displacement.
Cervical osteochondrosis of the 1st degree responds well to treatment and can even go into stable remission with minor acute episodes. Typically, treatment involves changing lifestyle, maintaining muscle and ligamentous apparatus with the help of therapeutic exercises. The 2nd degree of the disease has a less optimistic prognosis: in this case, treatment is aimed at relieving pronounced negative symptoms and preventing further destruction of the spine.
In some cases, therapy is required for diseases that have become a kind of catalyst for degenerative changes in cartilage. These include curvature of the spine, problems with the endocrine system, incl. hormonal imbalances, metabolic disorders, insomnia, depression, alcohol and nicotine addiction, excess weight, hereditary diseases.
Timely treatment of osteochondrosis of the cervical spine improves motor functions and prevents macrotrauma to the vertebrae, adjacent tissues, nerves, large vessels and organic systems. If you follow medical recommendations and daily maintenance therapy, the development of osteochondrosis can be slowed down and the mobility of the spine can be maintained until old age.
Osteochondropathy of the apophyses of the vertebral bodies[edit | edit code]
Osteochondropathy of the apophyses of the vertebral bodies
(aseptic necrosis of the apophyses of the vertebral bodies, or Scheuermann-May disease, Schmorl disease, osteochondropathy kyphosis, juvenile kyphosis) are more common in young men during the period of growth of the body at the age of 11-18 years. The disease was first described in 1921 by orthopedist Scheuermann, pathologist Schmorl and surgeon May.
The basis of spinal osteochondropathy is considered to be congenital inferiority of the discs and insufficient strength of the endplates of the vertebral bodies. The influence of hormonal factors is noted (the disease is often combined with endocrine disorders), as well as hereditary predisposition (possibly autosomal dominant inheritance). In the progression of deformity, the load factor plays an important role (improper mode, long sitting in a bent position, heavy physical work, carrying loads on the back).
As X-ray studies of a normal spine show, at the age of 10-12 years, additional apophyseal points of ossification of the vertebral body appear in the intervertebral cartilaginous discs, having a triangular shape on a radiograph in a lateral projection. The process of their bone fusion begins at the age of 14-15 years, and ends at 18-20 years. As a result, the vertebral body changes from a biconvex shape, characteristic of childhood, to a biconcave shape, which is characteristic of an adult.
Disruption of enchondral ossification in the area of growth zones of the vertebral bodies (apophyseal zones) in Scheuermann-May disease leads to their wedge-shaped deformation and the formation of kyphosis. Most often, 3-4 middle or lower thoracic vertebrae are affected; localization of the process in the lumbar spine is quite rare. The most typical involvement in the pathological process is the VII, VIII, IX and X thoracic vertebrae.
Among all diseases of the spine, osteochondropathy is the most common, but due to its asymptomatic and painless course, it is not always diagnosed.
The development of spinal osteochondropathy is divided into levels, stages and severity. The osteochondropathy process is characterized by typical localization in the thoracic region (58.6%), less often in the thoracolumbar (18.2%) and lumbar (17.8%). In 5.4% of children the process is widespread. The disease is rare in the cervical spine.
During osteochondropathy, three stages are distinguished depending on age. Stage I, the initial stage, is considered to occur during the immature period of the spine. Stage II, blooming, as occurring at the beginning of ossification of the apophyses of the vertebral bodies and intensive growth of the spine. Stage III, the final one, as corresponding to synostosis of the apophyses of the vertebral bodies.
Residual signs of osteochondropathy persist for up to 30-50 years. Osteochondrosis often develops against their background.
The severity of spinal osteochondropathy is determined by:
- prevalence, i.e. the number of affected vertebral segments;
- the severity of cardinal signs (severity of deformation of the vertebral bodies, degree of narrowing of the discs, the presence of single and multiple anterior and posterior Schmorl's hernias);
- the presence, as well as the severity of pain in the spine and secondary membrane-radicular syndrome;
- the degree of limitation of function and decompensation of the spine, determined by the deviation of the body to the side and back.
In children and adolescents, three degrees of severity of osteochondropathy have been identified, depending on the severity of the above symptoms.
Clinical picture[edit | edit code]
The disease develops slowly and goes through three stages over the course of a number of years. The clinical picture of spinal osteochondropathy depends on the child’s age, stage and severity of the pathological process. The earliest sign of osteochondropathy is considered to be pathological posture, and the most characteristic symptom is kyphotic deformity of the spine. However, the transition of pathological posture to kyphosis was not noted. Fixed kyphosis occurs in no more than 50% of cases of Scheuermann-May disease, and severe kyphosis in only 5%.
Most often and early (from 5-6 years old) in children with spinal osteochondropathy, asymmetry of the shoulder girdles, shoulder blades, lines and triangles of the waist, paravertebral asymmetry, which (unlike dysplastic scoliosis) is unilateral, is determined. In the initial stage, protruding spinous processes are identified at the level of pathological changes, the palpation of which is painful.
Early on, a restriction in forward body tilt can be observed. Stage I continues until ossification of the apophyses of the vertebral bodies occurs and is characterized by slightly increased thoracic kyphosis
In stage II of the process, approximately half of the patients develop kyphosis. Its formation is accompanied by increased lordosis in the cervical and lumbar regions, and scoliosis can also form at the same time. The deformation becomes fixed. The addition of radicular syndrome of discogenic origin leads to even greater limitation of spinal mobility. Severe forms of kyphosis occur in no more than 5% of children. In 15% of children with spinal osteochondropathy, a flat back is formed, and in 34%, the physiological curves of the spine remain within normal limits.
In stages II and III of spinal osteochondropathy, children and adolescents often report a feeling of fatigue in the back and pain in the spine, as well as in the lower extremities. These symptoms are mild and unstable. After a night's rest they usually disappear.
In stage I, but more often in II and III, a weakly positive Lasegue symptom is determined, less often - Wasserman, shell symptoms, which are combined with a limitation in tilting the body forward and, perhaps, serve as the cause of such a limitation.
There is a group of adolescents with stage II (usually III) of the disease with more constant pain in the lumbosacral region, which, as a rule, is accompanied by radicular syndrome, often occurs for no apparent reason and often disappears without treatment.
X-ray examination[edit | edit code]
X-ray examination provides a reliable diagnosis of spinal osteochondropathy only in stage II of the process.
In stage I of osteochondropathy, there are no cardinal signs, but indirect signs may occur. These include:
- projection narrowing of discs on a frontal radiograph;
- unilateral rotation of the vertebrae in the thoracic and lumbar region;
- slight wedge-shaped deformation of the vertebrae at the level of developing pathological kyphosis;
- flattening of the vertebral bodies with an increase in their dorsoventral size;
- narrowing of the discs in comparison with those above and below them.
When ossification nuclei of the apophyses of the vertebral bodies appear (from 7-8 years), all the signs characteristic of osteochondropathy are determined:
- wedge-shaped deformation of the vertebral bodies, flattening and increase in their dorsoventral size;
- massive lumbar vertebrae;
- violation of the integrity of the endplate;
- narrowing of the intervertebral spaces, uniform or only in the posterior sections;
- anterior and posterior, single or multiple Schmorl's hernias. Variable and rarer signs include marginal fracture of the bodies (usually lumbar vertebrae), disc calcification, retrolisthesis and spondylolisthesis.
After synostosis of the apophyses with the vertebral bodies, the wedge-shaped deformation decreases, due to which in stage III kyphosis and scoliosis decrease somewhat.
Treatment[edit | edit code]
They recommend general strengthening treatment, vitamin therapy, a rational regime of work and rest (sleeping on a hard surface), developing correct posture, and unloading the spine. In order to strengthen the muscle corset, therapeutic exercises, swimming in the pool, and massage of the back muscles are prescribed. Some authors recommend wearing a corset with a pelot at the apex of the deformity in the position of extension of the spinal column. With early treatment, it is possible to stop the development of the process and the formation of severe deformation. In isolated cases, with severe kyphosis with neurological symptoms, surgical treatment is indicated.
Admission to sports is prohibited.
Drug treatment of osteochondrosis of the cervical spine
At the beginning of the disease, patients are advised to take chondroprotectors, rehydration and saturation of cartilage tissue with nutrients. Vitamin-mineral and antioxidant complexes are actively used, incl. of natural origin. Drugs for the treatment of osteochondrosis of the cervical spine are used mainly externally or orally - in the form of warming, locally irritating, anti-inflammatory ointments, tablets, capsules. For stage 2 osteochondrosis, in addition to the above, analgesics, antispasmodics (muscle relaxants), and nonsteroidal anti-inflammatory drugs (NSAIDs) are used. Treatment is lifelong, but some drugs (painkillers, glucocorticosteroids and others) are prescribed in courses due to their harmlessness.
Chondroprotectors
Chondroprotectors in medicine are drugs that contain glycosaminoglycans and chondroitin sulfates. In everyday use, the names “glucosamine” and “chondroitin” are more common. Being the structural basis of cartilage tissue, they play the role of “building blocks” that the body uses to restore intervertebral discs. Taking chondroprotectors is complex - they have a beneficial effect on all articular surfaces in the body and inhibit the development of not only cervical, but also other types of osteochondrosis, as well as arthrosis and other degenerative cartilage diseases. These drugs must be taken for life and on an ongoing basis - since cartilage is devoid of blood vessels, their nutrition occurs through a diffuse method. This means that the growth of new cells is very slow - the first results are observed only after 3-6 months of taking chondroitin-containing products.
Ointments for osteochondrosis of the cervical spine
To treat cervical osteochondrosis, ointments with a vasodilating, anti-inflammatory and anti-edematous effect are used. To improve blood circulation, bee or snake venom is often added to their composition, and propolis and natural essential oils are added to strengthen the walls of blood vessels. For mild pain, local analgesic creams or ointments with an irritating effect can be prescribed, designed to distract the patient from unpleasant sensations. Warming ointments activate trophic and metabolic processes in tissues, preventing their destruction and restraining the degenerative process.
Tablets for cervical osteochondrosis
In the treatment of cervical osteochondrosis, tablets play a supporting role. Complex action analgesics are usually prescribed in tablet form - for example, analgin, ibuprofen or nimesulide, which have an anti-inflammatory effect. To relieve acute pain of a spasmodic nature, no-spa and similar medications can be prescribed.
For osteochondrosis of the cervical spine, it is especially important to take medications that strengthen blood vessels and improve blood microcirculation (for example, Actovegin). This helps curb the negative effect that this disease has on the brain, leading to hypoxia and malnutrition.
Injections
Injections in the treatment of cervical osteochondrosis are carried out locally to remove the local inflammatory process, which is insensitive to other methods of influence. For severe pain, lidocaine and novocaine blockades are also indicated. They represent the introduction of an anesthetic cocktail (it can contain over a dozen components - NSAIDs, glucocorticosteroids, decongestants, hyaluronic acid and other ingredients for nourishing and rehydrating cartilage). Spinal blocks should only be performed by specialists due to the high risk of damaging the spinal cord and nerve endings during injection, as well as the possible presence of contraindications.
A diet high in protein and moderate carbohydrate intake helps prolong the effect of taking medications. Including sea fish, shellfish and other dishes rich in gelling agents, calcium and vitamin D3 in the menu has a positive effect on the persistence of remission.
Spinal osteochondropathy: causes, diagnosis, treatment
The formation of the disease occurs in adolescence (from 11 to 18 years). In the first stages, it is quite difficult to identify it, since osteochondropathy does not manifest itself in any way. But if it is possible to diagnose it in a timely manner, after completing a course of special medical therapy, the disease is completely cured, and the growth of bone structures stops.
Features of the pathology
As a rule, the disease occurs in the thoracic spine. There are rare cases when it is observed in the cervical or lumbar region. Osteochondropathy is the destruction of the vertebrae or intervertebral discs. The disease is divided into types:
- Chondropathic kyphosis is the development of an inflammatory process in muscle tissue at the point of contact with the vertebral bodies, resulting in deformation of the latter to a “wedge” shape. This causes the spine to curve, leading to kyphosis.
- Chondropathy or “Calvet's disease” is a process of destruction within the vertebral body, during which the vertebrae become wider and decrease in length. A process appears, at the site of which pain occurs when exposed to external influences.
- “Krümmel’s disease” or inflammation in the body that forms as a result of suffering severe trauma. In this case, the vertebrae are deformed, and there is a curvature of the spine
in the posterior direction.
Causes of pathology
The death or destruction of bone tissue can be the result of a disruption in its blood supply, provoked by the following factors:
- Genetic predisposition;
- Changes in hormonal levels;
- Infectious diseases;
- Calcium and some vitamins cease to be absorbed;
- Congenital diseases of the musculoskeletal system;
- Hemocirculation disorders;
- Frequent microtraumas of the spinal column;
- High physical loads on the back, in particular on the spine.
Diagnosis of osteochondropathy
To avoid serious consequences, it is necessary to diagnose the pathology in the early stages, which is quite difficult to do, but is possible with the help of an X-ray examination or MRI. In addition, you should pay attention to the child’s behavior:
- There are complaints of unexpressed pain, which usually stops after rest.
- Rapid muscle fatigue, weakness, the appearance of asymmetry.
- As the disease progresses, the pain becomes more intense.
- There is a change in the shape of the spine, which leads to the destruction of bone tissue.
- The appearance of a tubercle or process at the site of damage to the vertebral bodies.
- It becomes difficult to tilt your body or head forward.
- At the last stage of pathology development, deformation of the chest occurs.
Treatment of the disease
As a result of untimely diagnosis of osteochondropathy, complications arise, the most common of which are kyphosis, spinal displacement and flat back. Middle-aged people may develop osteochondrosis. As a result of tissue death, the risk of fractures increases, so it is very important to consult a doctor immediately after the appearance of at least one of the syndromes.
The main goals of treatment therapy are:
- Relief from pain.
- Correction of posture and return of the vertebrae to their original position.
- Reducing the risk of osteochondrosis and other complications.
- Restoring the proper functioning of the intervertebral discs, vertebrae and body mobility (in case of difficulties when bending the head and body forward).
Correcting posture and restoring the proper functioning of the vertebral bodies are the most important goals in the treatment of osteochondropathy.
Therapeutic therapy completely excludes strong physical activity (including exercise therapy), physiotherapy, massage in any form, and taking medications not prescribed by a doctor. Sometimes bed rest on a hard surface is prescribed. If there is severe pain and a change in the shape of the vertebrae, a traction procedure with a load is performed on a beveled surface or under water. A prerequisite for treatment is adherence to a proper diet prescribed by a doctor and including foods high in vitamins A and B and calcium.
It happens that patients come with an advanced disease, when the process of developing complications has already started or there are pronounced changes in the spine. In such a case, surgical intervention cannot be avoided.
With osteochondropathy, the patient experiences various types of pain. In addition, the disease involves the destruction of bone tissue. To relieve a person from unpleasant sensations, medications are prescribed:
- Analgesics;
- Vasodilators;
- Multivitamin preparations based on calcium;
- Medicines that help restore intestinal microflora and absorb microelements from consumed foods.
Strong physical activity should be completely avoided. This condition especially applies to jumping in any form and lifting heavy objects. If there is no pain, a set of special therapeutic exercises is prescribed with a gradual increase in repetitions and a frequency of up to 3 times a day. An effective exercise for all patients is walking with a reclining stick located at the level of the thoracic spine. You need to grab it from behind with bent elbows.
The remaining physical exercises included in the treatment complex are developed individually together with the doctor, based on the person’s condition and taking into account the characteristics of the course of osteochondropathy.
Author: K.M.N., Academician of the Russian Academy of Medical Sciences M.A. Bobyr
Osteochondropathy of the vertebral body[edit | edit code]
Osteochondropathy of the vertebral body
(Calvet's disease, flat vertebra) was first described by J. Calve in 1925. This disease is not considered rare, and according to some data, among tumor and dysplastic processes in the spine in children and adolescents, it accounted for 20%. The pathology is based on aseptic necrosis of the spongy substance of the vertebral body. The duration of the disease is from 2 to 5-6 years. Flat vertebrae are more common in boys aged 3 to 16 years; mainly, at the age of 7-14 years, the thoracic vertebrae are most often affected, then the lumbar and cervical vertebrae. More than half have multiple eosinophilosis.
Clinical picture[edit | edit code]
Early symptoms of the disease include fatigue in the back, radiating pain or pain in the spine, which may first appear at the moment of jumping or somersaulting over the head. In these cases, pain may be a consequence of a pathological fracture of the vertebral body.
When palpating the spinous processes, tenderness and button-like protrusion of the spinous process of the affected vertebra are determined. Trunk bending and extension may be limited, and radicular and spinal symptoms may occur. Sometimes the disease begins with a rise in temperature to 39? C. Blood tests determine increased ESR and eosinophilia.
X-ray examination[edit | edit code]
Diagnosis is based primarily on the results of X-ray examinations.
On a profile X-ray, the affected vertebra is compacted, evenly flattened and expanded in the anteroposterior direction (platybrachyspondyly). The vertebral body takes on the appearance of a narrow strip, its anterior edge protrudes anteriorly, and the intervertebral spaces are widened.
Treatment[edit | edit code]
The basis of treatment is unloading of the spinal column (bed rest on the back on a hard bed or in a plaster bed with a reclinating cushion under the affected vertebra) and therapeutic exercises. Lying down, massage, general and therapeutic exercises are performed, aimed at reclinating the flattened vertebra and strengthening the back muscles (creating a muscle corset). During the recovery stage, it is recommended to wear a removable orthopedic corset that relieves stress on the spinal column. Some authors consider it advisable to perform posterior spinal fusion in order to stabilize the spine and quickly verticalize (lift to a vertical position) the patient.
Athletes at particular risk are boys aged 3 to 16 years (mainly from 7 to 14 years old) who engage in acrobatics, artistic gymnastics, weightlifting, martial arts, jumping, and team sports.
Admission to sports is prohibited.