Make an appointment by phone +7,,
Make an appointment online
Tenosynovitis is an inflammatory disease that affects the synovium of the tendon sheath. This pathology can be suspected due to such signs as swelling in the area of inflammation, pain in this area and an audible creaking sound in the tendon. Since the resulting pathology causes discomfort, it affects the patient’s usual lifestyle and performance.
What is synovitis
Synovitis is an inflammation of the synovial membrane that lines the inner surfaces of joints and tendons. The shell separates hard tissue and allows the joint to move with minimal bending. Due to its flexibility, it changes shape, adapts to the supporting bases and provides shock absorption to the joint.
For one reason or another, the synovial membrane, which resembles a kind of storage bag for synovial fluid, can become inflamed. It increases in size - visually, swelling forms on top of the joint, causing pain when moving. Over time, the inflamed tissues thicken, additional blood vessels form in them, and bleeding often occurs inside the joint. Prerequisites for complications arise, primarily for joint dysfunction and exacerbation of arthrosis, if it has already developed.
Synovitis – inflammation of the synovial membrane
Possible causes of the disease
The causes of tenosynovitis, as well as its nature, can be different. It usually develops against the background of wounds and injuries, resulting in infection (most often streptococcal and staphylococcal).
Sometimes the disease occurs due to infection with Neisseria gonorrhoeae. If this happens, tenosynovitis develops in the urethra, cervical canal, and pelvic organs. Patients with diabetes mellitus are most susceptible to the negative effects of pseudomonads, fungi and gram-positive microflora, so these microorganisms can lead to tenosynovitis in them.
One of the predisposing factors that can increase the risk of inflammation of the synovial membrane is weakened immunity.
Tenosynovitis: what is it?
This term refers to inflammation of the tendon sheaths, “tubes” filled with liquid lubricant. With the help of these sheaths, tendons connect muscles and bones. Sometimes their outer surface becomes inflamed, which makes it difficult for the structural elements of the musculoskeletal system to slide.
With tenosynovitis, a person also experiences pain and stiffness. However, only a doctor can say what exactly is inflamed. Most often, this problem affects the joints of the upper extremities, especially the wrists, and feet.
Tenosynovitis – inflammation of the tendon membranes
Chronic post-traumatic proliferative tenosynovitis
Post-traumatic tenosynovitis often develops gradually, taking on a chronic, sluggish form. Despite the apparent well-being, a serious deformation process occurs in the area of the tendon fiber.
Proliferative tenosynovitis usually goes through four phases of its development:
- at the initial stage, the synovial membrane gradually thickens, but no pronounced proliferation of villous accumulations is observed during MRI examination;
- villous tissue of proliferative foci of aseptic inflammation begins to form;
- the third stage is characterized by the fact that proliferative tissue from tendon fibers begins to spread into the projection of the joint capsule, forming contracture and stenosis;
- at the fourth stage, this process becomes diffuse and the joint becomes completely immobilized.
There is only one way to prevent chronic tenosynovitis: when the first signs of trouble appear, seek timely medical help.
Why do they become inflamed?
Synovitis or tenosynovitis itself is rarely a sign. Inflammation of the synovial membrane often occurs with rheumatoid arthritis of an autoimmune nature (unexplained origin). The pathology also accompanies juvenile and psoriatic arthritis, rheumatoid fever, lupus, tuberculosis and gout. Synovitis often develops after injuries, like post-traumatic arthrosis, but it manifests itself almost immediately, and not after months or even years.
Why the tendon sheaths become inflamed is still completely unknown. According to one version, it is due to excessive tension in the tendons, which are injured. This happens during the same type of work, for example, at a computer keyboard or on a conveyor belt. Tenosynovitis also accompanies diseases such as rheumatoid arthritis, gout, scleroderma, Reiter's syndrome, gonorrhea and diabetes mellitus.
One way or another, both pathologies are potentially dangerous for the body, since the inflammatory process can spread to neighboring tissues and harm other organs.
Joint inflammation often occurs after injury
What is synovitis and how to treat it, says a practicing traumatologist:
Clinical signs of tenosynovitis
The following symptoms may indicate inflammation of the synovium:
- swelling of the tissue around the diseased tendon, which can be determined by palpation during examination of the patient;
- pain developing in the area of the inflamed tendon;
- violation of joint movements, significant limitation of motor activity;
- soreness of the affected muscles during physical exertion.
The symptoms of tenosynovitis may differ depending on the cause that provoked the disease, as well as the location of the lesion. For example, in the case of an infectious origin, the tissue pathology in the area of inflammation may turn red. Body temperature often rises and signs of intoxication develop. The tendon in which the pathological condition has arisen may appear as a dense, painful cord upon examination.
How to tell if you have synovitis or tenosynovitis
The doctor will determine what exactly is inflamed, but you yourself can understand that inflammatory processes are occurring in the joint. They are indicated by the following signs:
- pain when moving;
- a feeling of warmth in the joint (this is especially felt with rheumatoid arthritis, as blood flow increases);
- the joint swells and increases in size;
- the skin over the joint turns red;
- general body temperature has increased (the most alarming signal indicating an infection in the body).
Is the joint swollen and painful? Don't put off visiting your doctor
How to cure tenosynovitis as quickly as possible?
We offer an innovative method of color pulse therapy, the discovery of which was awarded the Nobel Prize.
The answer is obvious: it is necessary to restore the clear functioning of the brain centers responsible for regulating the musculoskeletal system. The Neurodoctor device solves exactly this problem.
The device is based on the pulse therapy method. This method of treatment is recognized by modern medicine as one of the most progressive and highly effective. Thanks to pulse therapy, certain areas of the musculoskeletal system are “awakened,” which eliminates malfunctions in its functioning. This occurs due to the impact on the control centers of the brain.
How it works?
Neurodoctor affects the control centers of the brain.
The brain begins to produce dozens of neurohormones and form “corrective” nerve impulses.
Neurohormones are many times more effective than the most powerful drugs in quickly curing the disease. Nerve impulses eliminate pathological processes at the cellular level and correct the functioning of other organs and systems of the body.
LEARN MORE ABOUT THE METHOD
What to expect at your appointment with a rheumatologist?
A rheumatologist deals with inflammatory processes in joints. At the appointment, the doctor will examine the joint, determine the degree of pain, the nature of the pain, redness of the skin, and an increase in local temperature. You will be asked if you have had any recent injuries, and will also check your history of other joint diseases. If necessary, in such cases, an MRI or ultrasound is prescribed, which can determine the amount of accumulated fluid. X-ray diagnostics shows the integrity or damage of tissues.
When there is inflammation of the synovial or tendon membrane, it is important to determine the cause, otherwise therapy will be ineffective. For this purpose they prescribe:
- a blood test for the presence of a bacterial infection in the body to confirm or exclude the bacterial nature of the inflammation;
- puncture of synovial fluid with subsequent analysis of its composition.
They begin to treat inflammation in the joint only when they know the exact cause
Diagnosis of inflammatory lesion
The doctor takes a medical history, examines the patient, and palpates the painful area. If tenosynovitis is suspected, a Mucard test should be performed. It consists in the following. When the hand is abducted towards the elbow, the thumb of which is adducted and the rest are straightened, pain appears in the radius (namely, in the styloid process).
Laboratory diagnostic methods may be needed - bacteriological techniques, blood tests. They help not only to determine the general condition of the patient’s body, but also to identify the cause of tenosynovitis. Especially when it comes to the infectious origin of the disease, as this allows us to determine the causative agent of inflammation.
Among instrumental examination methods, the leading role is played by ultrasound and radiography of the affected area. They give an idea of the condition of the vessels, ligaments, nerves and joints located near the pathological area.
How to treat inflammation in a joint
Self-medication in such cases is very dangerous. Having discovered swelling around a joint, some people make the huge mistake of applying a warm compress to it. This is strictly forbidden due to possible complications. You should also not experiment with other folk methods, because the inflammatory process in the joint can spread to nearby tissues. It's about movement and freedom, about quality of life, so trust your doctor.
The treatment regimen for synovitis and tenosynovitis includes the following drugs:
- non-steroidal anti-inflammatory drugs, such as ibuprofen, which relieve swelling and reduce pain;
- for severe pain, short course corticosteroids;
- for quick pain relief - cold compresses;
- antibiotics – if tests confirm a bacterial infection.
When there is inflammation in the joint, it is very important to reduce the load as much as possible.
Do you need effective treatment, but still have doubts?
“Neurodoctor” is today considered one of the most effective methods of treating diseases of various etiologies. It goes well with traditional treatment methods and allows the body to recover faster. Today the Neurodoctor device is:
- A treatment method that won the Nobel Prize in Physiology or Medicine.
- The development history of the device goes back more than 20 years.
- Neurodoctor takes part in medical exhibitions around the world.
- The press writes about the Neurodoctor device (publications such as KP and others).
- Neurodoctor is used by thousands of people in 26 countries around the world.
- Manufactured in Russia at enterprises of the military-industrial complex.
- Can be used effectively together with any medications, without any side effects.
- The device has no contraindications.
Are injections given into the joint for synovitis?
Synovitis is often combined with arthrosis - degenerative changes in cartilage tissue. If the cartilage is damaged, it sooner or later becomes inflamed, and the inflammation spreads further. Excess fluid forms in the joint, it increases in size and hurts.
Injections of synovial fluid prostheses are the most progressive method of treating arthrosis. A gel is injected into the joint, which pushes the rubbing surfaces apart, replenishes the lack of lubrication and relieves the person from pain. The technique has a minimum of contraindications. But one of them is synovitis, inflammation of the synovial membrane. If this pathology has developed in a joint, you first have to cope with it, and only then focus on treating arthrosis.
Treatment of tenosynovitis in Lipetsk
Modern medicine has learned to qualitatively treat tenosynovitis, helping patients improve their quality of life, eliminating pathology. The most effective methods are also used in the Treatment and Diagnostic Center No. 1 in the city of Lipetsk. Depending on the cause of the disease, its course and other features, the following may be used:
- certain groups of drugs - antibiotics, painkillers, anti-inflammatory, tonic;
- local administration of drugs that eliminate pain and inflammation, stimulating blood flow in the affected area;
- novocaine blockades;
- HILT therapy (high-tech pulsed laser therapy);
- methods of physiotherapy - laser therapy, magnetic therapy, mud therapy, acupuncture, etc.
In case of purulent tenosynovitis, surgical treatment is necessary. The doctor opens the purulent focus and performs manipulations to create conditions for the outflow of pus. But, surgical intervention may be needed not only in such situations. There are a number of other indications.
Experienced doctors at LDC No. 1 select the most optimal treatment methods for a particular patient, which can give excellent results.
Make an appointment with a surgeon in Lipetsk by phone, +7, +7 (4742) 37-04-52 or online
Rehabilitation after tenosynovitis of the hand
When treating tenosynovitis of the hand, special attention is paid to therapeutic massage and a set of exercises. Massage promotes proper blood supply and delivery of nutrients to tissues, thereby accelerating the healing and recovery process. You can do self-massage for therapeutic and preventive purposes. Before each recovery set of exercises, a 20-minute massage session should be performed to make the exercise as comfortable as possible.
The set of exercises is aimed at restoring range of motion and stretching muscles and tendons. When tissues work, they are filled with blood rich in oxygen and nutrients. This process accelerates tissue regeneration and completely eliminates the pathological process.
The set of exercises includes flexion/extension movements of the fingers, clenching/unclenching a fist without resistance and with an expander or rubber ball, stretching the hand and individual fingers. Embroidery, weaving, stringing beads, and sculpting small figures fully restore finger motor skills.
When performing exercises, you should pay attention to the presence of pain. Do not forcefully perform movements.
Diseases of periarticular soft tissues: clinical picture, features of local corticosteroid therapy.
GENERAL SECTION
Importance of the issue:
The group of patients with inflammatory processes in the periarticular soft tissues is numerous in the practice of general practitioners, neurologists, and rheumatologists. At the same time, due attention is not always paid to the differential, and, most importantly, to the topical diagnosis of these conditions. In this case, this is hardly justified, since all such processes, as a rule, are easily amenable to local therapy with anesthetics and corticosteroids, provided that the drug is accurately administered to the lesion. On the other hand, the lack of effective therapy can significantly reduce the patient’s functional ability, even to the point of disability (for example, fibrosing capsulitis of the shoulder, as a consequence of poorly treated shoulder-scapular periarthritis, etc.)
General provisions:
Periarticular tissues include muscle tendons, their synovial sheaths, places of attachment of tendons to bone - entheses, mucous bursae, ligaments, fascia, aponeuroses, muscles surrounding the joint.
The inflammatory process can be localized in any of these formations and, accordingly, can be defined as tendonitis
(inflammation of the tendon),
tendovaginitis
(inflammation of the tendon sheath), bursitis (inflammation of the bursa),
tendobursitis
(inflammation of the tendon and bursa),
enthesitis/enthesopathies
(inflammation of the enthesis ),
ligamentitis
(inflammation of the ligaments),
fibrositis
(inflammation of the aponeuroses and fascia),
myotendinitis
(inflammation of the muscle areas adjacent to the tendon). In practice, the term periarthritis is often used to describe damage to any periarticular soft tissue structures. As already mentioned, for successful therapy you need to strive for a more accurate topical diagnosis, try to answer the question “What is affected?” - tendon, bursa, etc., and which muscle or bursa specifically. So, for example, under the general diagnosis of shoulder - scapular periarthritis, processes of different localization are often hidden - subacromial bursitis, subdeltoid bursitis, tendinitis of the long head of the biceps, tendinitis of the infraspinatus muscle, etc. It is possible to differentiate these conditions even without resorting to special research methods (See the chapter “Lesions of soft tissues in various regions of the extremities”).
Etiology and pathogenesis:
All diseases of periarticular soft tissues can be divided into: 1.
primary inflammatory
, when the inflammatory process passes from adjacent structures, most often from joints with arthritis.
2. primary degenerative
, when the development of inflammation is associated with microtraumatization of tendons and ligaments due to excessive loads and (or) trophism in soft tissues.
Neurotrophic disorders contribute to the more frequent development of glenohumeral periarthritis (PSP) in individuals with radicular syndromes in the cervical spine. The same mechanisms underlie the occurrence of PLP after myocardial infarction.
Endocrine disorders, causing a deterioration in metabolic processes in tissues, explain the more frequent development of periarthritis in women during menopause.
In patients with congenital inferiority of connective tissue (diffuse connective tissue dysplasia), microtraumatization of tendons and ligaments occurs even with minor physical exertion, with the subsequent development of inflammatory phenomena. This situation is most often the cause of joint pain in young people.
General diagnostic principles:
Clinically, lesions of the periarticular soft tissues are manifested by pain in the joint area and movement disorders. In this situation, the differential diagnosis is primarily carried out with damage to the joints themselves (see table).
Determining the nature of the lesion of the musculoskeletal system
| SIGN Nature of pain | ARTHRITIS Constant, both at rest and during movement | PERIARTIAL TISSUE DAMAGE Occurs with certain movements |
| Localization of pain | Spread over the entire projection of the joint | Local, the patient indicates the point of maximum pain |
| Active and passive movements | Reduced range of both active and passive movements | Reducing the volume of active movements while maintaining the range of passive movements |
| Nature of swelling | There is effusion in the joint, thickening of the synovial membrane | Asymmetry, connection of swelling with a specific bursa, tendon sheath |
Among the instrumental methods for diagnosing periarticular lesions, thermographic research is used, based on the difference in temperature gradients (d T). An increase in d T is observed in synovitis and periarthritis, but its value in periarthritis is much lower.
For accurate topical diagnosis of periarticular lesions, ultrasound examination of joints is successfully used, which helps to identify the presence of exudate in bursae and synovial sheaths, latent ruptures of tendons and ligaments, and to see the exact localization of the source of inflammation.
General treatment approaches:
1) Elimination of provoking factors
- limiting the load on the affected limb; in case of severe inflammation - complete rest of the limb.
2) Anti-inflammatory therapy
- NSAIDs, local use of ointments with an anti-inflammatory effect (Fastum-gel, Dolgit, Diclofenac-gel, etc.), compresses with 30-50% dimexide solution on the area of greatest pain, local injection of corticosteroids into the affected area structure.
3) Improvement of metabolic and trophic processes
- after reducing the severity of the inflammatory process (reduction of pain, absence of night pain) - magnetic therapy, laser therapy, electrophoresis with dimexide, brine, mud applications (ozokerite, paraffin), vitamin therapy (nicotine calcium) ta, vitamins gr., “B”, antioxidants), biostimulants (aloe, solcoseryl, S.Traumell, S.Zeell) 4)
Rehabilitation
- exercise therapy. When inflammatory phenomena subside, but the range of active movements continues to decrease, massage with joint development, electrophoresis with lidase, balneotherapy.
I would like to dwell in more detail on the issue of local therapy with corticosteroids for patients with inflammation of the periarticular tissues.
In the absence of contraindications to this type of treatment, there is no point in delaying this procedure. Patients usually tolerate the injections well. If the technique is followed and modern drugs are used, there are practically no complications, and with correct topical diagnosis and administration of the drug precisely to the site of inflammation, it is possible to quickly stop the inflammatory process and avoid the transition of the disease into chronic forms that are difficult to treat.
For periarticular administration, it is best to use drugs from the Betamethasone group - celeston
(short-acting) or
diprospan
(long-acting).
It is also possible to use hydrocortisone
. The drugs are administered with local anesthetics (novocaine or lidocaine) in one syringe. Doses and number of injections depend on the location (see special section). The use of triamsinolone (Kenalog) drugs for the treatment of tendonitis is undesirable, because they can cause degenerative processes in ligaments and tendons, even to the point of rupture of the latter. Kenalog is intended for injection into hollow synovial structures - bursae, synovial sheaths, joint cavity, therefore, if you are not sure of an exact hit, it is better to use other drugs. After the acute inflammatory reaction subsides, we successfully use periarticular administration of homeopathic medicines Traumell and Zeell. The composition of the preparations includes proteolytic enzymes, a complex of plant alkaloids, and components of cartilage tissue. The drugs have a chondroprotective effect and improve metabolic and trophic processes directly in the affected area. Treatment regimen: 2 ml Zeell (Traumell) + 2 ml novocaine (lidocaine), 1 ml celeston is added to the first 2 injections. All components are administered periarticularly in one syringe. The course of treatment is 5 - 10 procedures with an interval of 3-5 days. Experience shows that these drugs are most effective specifically for diseases of periarticular tissues.
Special section.
Lesions of periarticular tissues in various regions of the extremities.
1. Shoulder joint area.
Subacromial bursitis
The subacromial bursa is separated from the cavity of the shoulder joint by a capsule with the supraspinatus tendon running through its thickness. Laterally, the bursa continues into the subdeltoid bursa. The bursa is bounded superiorly by the acromion and thoracoacromial ligament. Subacromial bursitis is an extremely common cause of pain in the shoulder joint in patients with RA, while true arthritis of the shoulder joint is much less common.
Diff. the diagnosis is made with arthritis of the shoulder joint (see table), arthritis of the acromiocleidoid joint, and supraspinatus tendinitis. To do this, use the Dowborn test or the “painful arc” test. The patient moves the outstretched arm to the side until it touches the ear and slowly lowers it. With subacromial bursitis and supraspinatus tendinitis, pain occurs in the middle of the movement (60-120 degrees abduction). With pathology of the acromial clavicular joint, pain is observed when an outstretched arm approaches the ear (upper sector - the last 15-20 degrees of the arc). The diagnosis is confirmed by palpation tenderness in the projection of the acromial clavicular joint. To rule out supraspinatus tendinitis, an active shoulder abduction resistance test is performed. Pressing the patient's hand to the body, they ask to move the hand to the side. Tension of the supraspinatus muscle occurs when the arm is motionless. With subacromial bursitis, the test is painless, while with supraspinatus tendinitis, pain occurs in the shoulder area.
Treatment:
Injection of corticosteroids into the subacromial bursa is effective.
Doses:
10-20 mg of Kenalog (0.5 ml) or 4 mg of Diprospan (0.5 ml). The needle is inserted into the space between the most protruding part of the acromion and the head of the humerus along the outer surface of the shoulder strictly horizontally, to a depth of 2-3 cm. Correct entry into the bursa brings quick and lasting relief from pain, the abduction function is restored (the patient can comb his hair). How Usually one injection is enough.
Tendinitis of the rotator cuff muscles.
The rotator cuff is formed by 4 muscles: supraspinatus, infraspinatus, teres minor and subscapularis. The supraspinatus, infraspinatus, and teres minor muscles originate on the posterior surface of the scapula and insert into the greater tuberosity of the humerus. These muscles are involved in abduction and external rotation of the shoulder. The subscapularis muscle begins on the anterior surface of the scapula and attaches to the lesser tubercle of the humerus. It is involved in internal rotation of the shoulder.
Tendonitis of these muscles is the most common cause of pain in the shoulder joint, which is associated with the passage of tendons in narrow anatomical channels and the heavy load placed on these muscles.
Damage to the cuff muscles is characterized by pain in the upper outer part of the shoulder, sometimes radiating to the elbow. The pain usually occurs after unusual physical activity. For example, working with your arms raised high when painting ceilings, etc. The supraspinatus tendons are most often affected. Pain occurs in the middle sector of the arch during the Dowborn test and pain with resistance to active abduction of the shoulder (see “Subacromial bursitis”).
If the infraspinatus/teres minor muscles are affected, an active external rotation resistance test of the shoulder is positive. To do this, the patient bends the arm at the elbow joint 90 degrees. The doctor presses the patient’s elbow to the body with one hand, fixes the forearm with the other hand and asks the patient to push his arm outward, resisting this movement. At the time of the test, pain occurs in the upper shoulder.
If the subscapularis muscle is affected, the active internal rotation resistance test is positive. It is carried out similarly to that described above, only the patient is asked to push his hand inward.
Sometimes palpation pain is detected in the projection of the affected tendons. The patient is asked to place his hand on the opposite shoulder. Under the protruding area of the acromion, towards the greater tubercle, the tendons of the supraspinatus, infraspinatus, and teres minor muscles are palpated. Then the patient places his hand behind his back. The subscapularis tendon is palpated under the anterior part of the acromion process towards the lesser tubercle.
Treatment:
Injection of corticosteroids into the tendon of the affected muscle is indicated.
To determine the injection site, you can focus on the most painful points. The drug of choice is diprospan. Dose
2-4 mg (0.2-0.5 ml) with 0.5 ml of 2% novocaine. The drug is injected into dense structures under high pressure. Sometimes injections are performed at several points. Tendinitis tends to be chronic, so injections have to be repeated every few months.
Tendinitis of the long head of the biceps
The tendon of the long head of the biceps passes along the intertubercular groove into the capsule of the shoulder joint. The protrusion of the synovial membrane of the shoulder joint creates a synovial sheath for this tendon. Tendonitis of the long head of the biceps tendon causes pain in the upper anterior portion of the shoulder. Pain occurs after physical activity associated with overstrain of the biceps muscle (heavy lifting). On palpation, pain in the intertubercular groove is determined. Abduction and rotation of the shoulder are usually not impaired. To identify damage to the biceps tendon, an active supination resistance test of the hand is performed. The position of the patient's arm is the same as when examining the rotator cuff. The doctor clasps the patient’s hand with both hands and asks him to actively supinate the hand, resisting this movement—if the long head is affected, pain occurs.
Treatment:
Inject 2-4 mg of diprospan with 0.5 ml of 2% novocaine into the intertubercular groove until dense structures are reached.
2. Elbow joint area
External epicondylitis (“tennis elbow”)
Attached to the lateral epicondyle of the humerus are the muscles involved in wrist extension—the extensor carpi radialis longus and brevis (the clenched fist muscles) and the brachioradialis muscle. Inflammation of the tendons of these muscles where they attach to the bone is called lateral epicondylitis. The muscles are weak flexors of the forearm, so if they are damaged, the function of the elbow joint is practically not affected.
This pathology usually affects people over 35 years of age. The appearance of pain in the elbow joint is preceded by an unusual load - working in the garden, playing sports after a long break, etc. The patient accurately indicates the place of greatest pain, corresponding to the external epicondyle of the humerus. Pain may radiate down the outer surface of the forearm to the hand. The pain is easily reproduced by resistance to active extension of the wrist joint.
Treatment:
Local administration of Diprospan or Hydrocortisone is very effective.
It is natural that the symptoms of epicondylitis intensify on the first day after the injection (tissue reaction is not hydrocortisone crystals). The patient should be warned about this. Improvement occurs on the 2nd day; if necessary, the procedure is repeated after 10 days. The dose
of the administered drug is 10-15 mg of hydrocortisone or 2-4 mg of diprospan with 1.0 ml of 0.5% novocaine.
Internal epicondylitis (golfer's elbow)
The tendons of the muscles attached to the medial epicondyle are affected - pronator teres, ulnar and radial flexors of the hand, and palmaris longus. Medial epicondylitis is less common than external epicondylitis. Palpation pain is detected at the site of muscle attachment. Pain may radiate along the ulnar surface of the forearm to the hand. Pain is also reproduced by resistance to active flexion at the wrist joint with a supinated forearm.
Treatment:
The technique of local administration of diprospan with novocaine (hydrocortisone) and the dose of drugs are similar to those described above for external epicondylitis, but the tissues here are less dense. It should be remembered that the ulnar nerve passes between the internal epicondyle of the shoulder and the olecranon process and, if inserted carelessly, it can be injured.
Olecranon bursitis
The superficial bursa of the olecranon process is located above the eminence of the olecranon process, and does not communicate with the cavity of the elbow joint. Inflammation of the bursa occurs in isolation as a consequence of chronic injury to the posterior-inferior surface of the elbow (in car drivers resting their elbow on the door), or in combination with arthritis due to gout and RA. In the area of the olecranon, a low-painful round formation the size of a chicken egg with a soft consistency appears. It becomes clearly visible when the arm is extended at the elbow joint. With isolated bursitis, the function of the elbow joint is not noticeably affected.
The bursa is punctured at the site of the greatest fluctuation; the resulting fluid is often hemorrhagic in nature (a consequence of traumatization of an already inflamed bursa). If an infectious etiology of bursitis is excluded, 30-40 mg of Hydrocortisone or Triamsinolone is administered after evacuation of the effusion.
3. Brush area
Nodular tenosynovitis of the finger flexors.
The finger flexor tendons or annular ligament in the area of the m/phalangeal joints are affected. The “snapping finger” syndrome develops, which is associated with the appearance of a nodule on the flexor tendon (a consequence of a primary or secondary dystrophic-inflammatory process), which makes it difficult for the tendon to slide into the vagina at the level of the fibrous canals in the joint area, and then completely blocks movement.
Typical complaints from the patient include a clicking sensation when bending and straightening the finger. As the process progresses, the finger freezes in the position of flexion or extension contracture. Upon examination, a nodule is palpated on the palm or palmar surface of the finger in the projection of the flexor tendon.
Treatment:
Injection of corticosteroids into the flexor tendon is effective. The injection is carried out in the palms up position. The needle is advanced towards the tendon sheath at an angle of 30-45 degrees. Usually short-acting corticosteroids are used - 12-18 mg of Hydrocortisone (1-1.5 ml of suspension) or 0.2 ml of celeston. If necessary, the injection is repeated 2-3 times at weekly intervals. More powerful drugs are rarely used. If the process lasts for a long time and there is no effect from the administration of HA, it is advisable to use hyaluronidase preparations in the form of electrophoresis or applications (Ronidase). It is rarely necessary to resort to surgery.
Ganglion
(hygroma) - a nodule, the size of a pea or slightly larger, located on the back of the hand or in the area of the wrist joint in the projection of the extensor tendon sheaths. It is a hernial protrusion of the synovial vagina. Pain or discomfort occurs when moving your fingers. The contents of the ganglion are synovial fluid.
Treatment:
puncture and administration of a small dose of corticosteroids. Surgery is rarely necessary.
Exudative tenosynovitis of the extensor fingers
- often accompanies inflammatory arthropathy of the hand area. It manifests itself as limited swelling on the dorsal side of the wrist joint. A differential diagnosis is made with arthritis of the wrist and radioulnar joints, which are also accompanied by swelling of the dorsum of the hand. To do this, ask the patient to bend and straighten the hand. With extensor tendovaginitis, during extension of the hand, the swelling moves distally, repeating the movement of the tendons.
Treatment:
The synovial vagina is punctured at the site of greatest swelling, the exudate is removed and 0.2-0.5 ml of celeston (diprospan) is injected. If necessary, repeat the procedure.
Stenosing tenosynovitis of the abductor longus and extensor brevis of the 1st finger (De Creven's disease).
The disease was described about 100 years ago as an occupational disease of laundresses. The tendons of the long abductor and the meek extensor of the 1st finger pass in the 1st canal of the dorsal ligament. The narrowing of this canal as a result of inflammatory phenomena leads to compression of the tendons and the development of the clinical picture of DeCreven’s disease.
Currently, the disease occurs in young women in the first months after childbirth (a sharp increase in household workload) and in patients with hypermobility syndrome in the 2nd half of life. The clinic consists of the appearance of attacks of severe pain in the area located 1.5-2 cm proximal to the base of the 1st finger (“anatomical snuffbox”). You can also see swelling in this place. A convenient diagnostic test is to reproduce a pain attack when bringing 1 finger to the palm, fixing it with other fingers and passively or actively abducting the fist towards the elbow. A differential diagnosis is made with radiation styloiditis, in which maximum pain is localized proximally, above the styloid process, and intensifies with active supination of the wrist.
The most effective treatment
De-Creven disease - injection into the tendon sheath of the indicated muscles of a mixture of 12-20 mg of Hydrocortisone and 1 ml of 0.5% novocaine (or 0.5 ml of celeston with novocaine). The drug is injected into the area of the anatomical snuffbox towards the tendons. Sometimes the injection is performed at several points. As a rule, one procedure is sufficient.
Radiation styloiditis
- tendoperiostitis of the tendon of the long supinator of the forearm at the site of its attachment to the styloid process of the radius. Mostly women aged 40-60 years are affected (most often dressmakers). Styloiditis is usually right-sided, which indicates the importance of frequent microtrauma due to the characteristics of professional activity. The main clinical sign is pain in the area of the styloid process of the radius (slightly above the inner edge of the wrist joint), which increases with supination of the forearm. Local swelling is often found in this area. The radiograph reveals periosteal reaction and osteoporosis of the styloid process. A differential diagnosis is made with DeCreven's disease (see above).
Treatment:
The disease is difficult to treat. Sometimes it is effective to administer diprospan in a dose of 0.3 ml to the insertion site of the supinator tendon. The injection is repeated at intervals of 2-3 weeks.
Ulnar styloiditis
- tenosynovitis of the extensor carpi ulnaris or stenosing ligamentitis of the 4th canal of the dorsal ligament of the hand, in which the tendon of the extensor carpi ulnaris passes. Radiation styloiditis is much less common. The cause of the disease is trauma to this area or professional microtraumatization (for seamstresses, typists, etc.). Clinically - spontaneous pain in the area of the styloid process of the ulna, intensifying with radial abduction of the hand and radiating to the 4th-5th finger. A local painful swelling is palpated above the styloid process.
Treatment:
The same as with radiation styloiditis.
4. Hip area.
Trochanteritis, subtrochanteric bursitis.
Inflammation of the tendons at the site of their attachment to the greater trochanter - trochanteritis - is a common cause of pain in the hip joint. This disease often complicates the course of moderate osteoarthritis in women 40-60 years old. And it manifests itself with pain radiating along the outer surface of the thigh. A typical patient complaint is the inability to lie on a certain side. There is a distinct local pain in the trochanter, preservation of the volume of hip rotation and pain with resistance to its active abduction. Clinically, trochanteric enthesopathy (trochanteritis) is indistinguishable from subtrochanteric bursitis - inflammation of a small bursa also located in this area. But this has no practical significance, since in both cases the therapy is the same.
Treatment:
Injection of corticosteroids into the greater trochanter area is effective. The injection technique is simple. The needle (0.8 - 40 mm), with pronounced subcutaneous tissue (0.8 - 70 mm), is directed perpendicular to the surface of the skin until it reaches the trochanter. Infiltrate the entire painful area as close to the bone as possible with a mixture of 80 - 125 mg of hydrocortisone or 8 mg of Betamethasone, with 6 - 10 ml of 0.5% novocaine. The effect is usually complete and long lasting.
Enthesopathy of the ischial tuberosity
- inflammation of the tendons at the site of attachment to the ischial tuberosity. It occurs both as part of some sero-negative spondyloarthritis (reactive arthritis, ankylosing spondylitis) and independently. The ischial tuberosity is located in the lower part of the buttock and experiences a lot of stress when the patient is sitting, especially on a hard base. A typical patient complaint is pain in this position, to a lesser extent when walking at the moment the leg is lifted off the floor.
Treatment:
Local corticosteroid therapy is also effective. By palpation, the point of highest pain corresponding to the ischial tuberosity is determined. The needle is directed perpendicular to the skin surface towards the tubercle until it touches the bone tissue and the painful area is infiltrated with 40 - 60 mg of hydrocortisone (0.5-1.0 ml of diprospan) with 3 - 4 ml of 0.5% novocaine. Needle 08 - 40 mm.
5. Knee joint area
Prepatellar bursitis.
In the area of the knee joint, you can encounter isolated bursitis (prepatelar and infrapatelar). The prepatellar bursa is located superficial to the patella and does not communicate with the joint cavity. The cause of bursitis is often chronic trauma to the patella (working on the knees), sometimes gout. Purulent bursitis is rare, always as a result of an acute injury with a violation of the integrity of the skin.
Clinically, prepatellar bursitis is characterized by the appearance of a local, slightly painful swelling on the anterior surface of the joint.
Treatment:
The bursa is punctured to obtain a viscous liquid. It is rarely possible to remove it completely. After excluding the infectious nature of bursitis, 20-40 mg of hydrocortisone or 0.5 ml of diprospan is injected into the bursa.
Relapses of bursitis can be avoided by eliminating the etiological factor (protection of the knee joint during chronic injury, control of uric acid levels during gout).
Anserine bursitis (enthesopathy of the crow's foot area).
The “foot anserine” is the site of attachment to the tibia of the tendon of the sartorius, graceful and semitendinosus muscles, where a small bursa is located. This place is located 3-4 cm below the projection of the knee joint fissure along its medial surface. Inflammation of this area very often develops in obese women suffering from arthrosis of the knee joints. Typical complaints of the patient are pain when walking in the indicated place. The pain intensifies when going up the stairs (unlike the pain associated with arthrosis, the pain intensifies when going down). “Starting pain” is typical - after prolonged sitting, the beginning of walking causes pain. The patient points with his finger the painful point corresponding to the location of the anserine bursa. Upon examination, sharp palpation pain with an area of 3-4 sq. cm is determined. Often the symptoms of enthesopathy bother the patient more than the manifestations of gonarthrosis itself.
Treatment:
Injecting corticosteroids into the bursa area is very effective. A 0.8-40 mm needle is inserted into the point of maximum pain perpendicular to the skin surface and advanced into the tissue until it touches the bone surface. For infiltration, use a mixture of 0.5-1 ml of celeston with 2 - 3 ml of 0.5% novocaine (the need for more powerful drugs is rare, usually betamethasone). Infiltrate the entire painful area, trying to inject the drug as close to the bone surface as possible. If the procedure is carried out correctly, the pain should disappear after 3-4 minutes.
Enthesopathies of the lateral surface of the kneecap.
Another possible localization of enthesopathies is the inferolateral surface of the patella on the lateral or medial side (accompanies gonarthrosis). The diagnosis is made by palpation, noting that the patient responds most to pressure at the above points. There may be several of them on both sides of the patella. It has been shown that peripatellar administration of mildly acting drugs (hydrocortisone) in this category of patients has no less, and often greater, effect in comparison with intra-articular administration. Considering that in osteoarthritis, the introduction of corticosteroids into the joint assumes their effect on cartilage metabolism and is undertaken only with obvious synovitis, such an approach may be the method of choice for the category of patients with pain and the absence of obvious synovitis.
6. Ankle and foot area.
Tenosynovitis of the peroneal muscle.
The muscle tendon passes under the lateral malleolus; when it is inflamed, you can see a sausage-shaped thickening along the tendon sheath. When walking, patients note pain in this place. Treatment consists of injecting 30-40 mg of Hydrocortisone or 10 mg of Triamsinolone with novocaine (0.3 ml of Diprospan) into the tendon sheath. The needle is directed along the tendon under the ankle. The introduction should be relatively free, with resistance to the fluid flow, the needle is moved in the tissue until it disappears. When injected into the tendon sheath, it gradually increases in volume.
Achilles tendinitis (Achilles tendonitis), posterior talar bursitis - a condition often found in seronegative spondyloarthritis. Severe damage to the Achilles tendon can be seen in patients with joint hypermobility syndrome with severe flat feet, usually over the age of 30 years. With Achilles' pain there is swelling and pain with stress in the area of the well-known tendon or where the tendon attaches to the heel bone. In the latter case, pain may be associated with bursitis of the posterior talar bursa, which is located here. The pain is excruciating and is most pronounced when walking and standing for long periods of time.
Treatment:
Triamsinolone preparations should never be injected into the Achilles tendon area. There are many known cases of subsequent tendon rupture, which were a consequence of the locally degenerative effect of this drug. Hydrocortisone and Betamethasone are the drugs of choice for this pathology. Using a small needle, a suspension of corticosteroid with novocaine is injected fractionally into the 2-4 most painful points along the tendon. For posterior talar bursitis, the drug is injected directly into the bursa. In this case, the needle is directed from the lateral side just above the posterior calcaneal tubercle and slowly advanced towards the bursa until a sensation of “failure” is felt. At this point, you can get a few drops of liquid. If there is no fluid in the bursa, the correct administration of the drug will help to check the addition of 0.3-0.5 ml of 2% novocaine to the corticosteroid. After a successful injection, the pain subsides within a few minutes.
Subcalcaneal bursitis.
The subcalcaneal bursa is located on the lower surface of the calcaneus at the site of attachment of the plantar aponeurosis. Pain in the heel area is called thalalgia and can be of dystrophic and inflammatory origin. Inflammatory thalalgia is a common (and sometimes the only) manifestation of some seronegative spondyloarthropathies (urogenic reactive arthritis, ankylosing spondylitis). The degenerative nature of enthesopathy with the formation of heel spurs (calcification of the enthesis) is common in older people.
Treatment:
Corticosteroid injection therapy for thalalgia is often more effective than other treatments (physical therapy, radiotherapy). For moderate pain during exercise, use a heel insert made of dense-elastic material with a cutout corresponding to the pain point. Often this is enough for dystrophic pain in older people; after a while the pain subsides on its own. If the effect is insufficient and in case of inflammatory thalalgia, a corticosteroid is injected into the painful point. Injections into the heel area are painful, with bursting pain associated with the fine-mesh structure of the fiber around the aponeurosis and the abundance of pain receptors in this area. Adding an anesthetic to a corticosteroid does not reduce pain, since the maximum pain is expressed at the time of administration (including the anesthetic). After determining the point of greatest pain and thoroughly treating the field with iodine and alcohol, the needle is inserted from the medial or lower side to the heel tubercle until it touches the bone surface. The drug suspension is administered against significant tissue resistance. It is rarely necessary to administer more than 1 ml of the mixture. Accurate delivery of the drug is the key to the effect. Adding a local anesthetic (2% novocaine, lidocaine) to the suspension allows you to judge its accuracy already in the first minutes after the injection - palpation pain should disappear. If the effect is insufficient or the pain recurs, the injection is repeated after 2-4 weeks. Due to the painfulness of the procedure, it is better to immediately use long-acting drugs - diprospan.
Dolgaleva A.A.
Literature:
1. V.A. Nasonova “Clinical rheumatology” - Moscow 1989 2. Michael Doherty “Clinical diagnosis of joint diseases” - Minsk 1993 3. A.G. Belenky - Intra-articular and periarticular administration of corticosteroid drugs for rheumatic diseases. (textbook for doctors) - Moscow 1997
Depending on the stage of the disease, we choose one or more treatment methods in Moscow:
Osteopathy in Moscow
Soft technique of working with the spine, joints, muscles, ligaments, internal organs. Eliminates pain and starts the self-healing process.
Therapeutic massage, osteopathy, manual therapy in Moscow
Helps bones and joints take the correct physiological position, relieves pain and spasms, relaxes muscles.
Acupuncture in Moscow
Work on biologically active points. It affects the affected area and the body as a whole. Eliminates the cause of the disease and removes the symptoms.
Tenosynovitis of the flexor fingers
Tenosynovitis of the finger flexors usually develops after injury. The patient experiences pain, swelling of one or more fingers, and the tendon thickens. As a rule, the wrist flexor tendons are affected along with the annular ligament. The tendon slides into the vagina with difficulty, and as the pathology progresses, it completely immobilizes and assumes a flexed position. If you palpate, a nodule will be felt on the palmar side.
If the doctor decides on a surgical treatment method, then the operation is complex, since the palmar surface contains multiple anatomically significant structures that are easy to damage.
Doctors also identify other factors of the disease:
- joint degeneration. For example, very often de Quervain's tenosyvitis of the tendon of the long head of the biceps affects a disease similar to bursitis;
- genetic predisposition;
- dangerous infectious diseases: HIV, syphilis, herpes, tuberculosis. In such cases, the infection does not enter through the wound, but spreads throughout the body through the blood;
- age: everyone has known for a long time that with age, a person’s bones and joints become worse and often succumb to various injuries; strain and overwork of the tendon. As a rule, this factor is familiar to people of certain specialties. For example, a person constantly loads a specific muscle group while others remain unused. That’s why the lack of variety in movement puts a lot of stress on the body, which leads to the development of tenosynovitis. This problem is very familiar to office workers who have a sedentary job.
Special forms of the disease
Inflammatory lesions of tendons and synovial sheaths in patients of this group develop due to:
- metabolic disorders;
- for systemic and endocrine diseases;
- dystrophic changes in organs and tissues;
- genetic pathology.
Nodular tenosynovitis most often affects middle-aged and elderly women. New growths 2-5 cm in size appear on the hands, wrist, and interphalangeal joints, growing from the synovial tendon sheaths. Since 1852 (the first description of this pathology), discussions about their origin have continued. Various assumptions have been made, the main theories being tumor, infectious, genetic. There is no consensus. It is difficult to treat; after surgical removal of the formations, relapses occur.
De Quervain's tenosynovitis was first described as an occupational disease of laundresses. The tendons of the extensor longus and flexor brevis of the first finger pass in the same synovial sheath. Their thickening as a result of repeated microtrauma leads to limited movement of the thumb. It develops in kindergarten teachers with frequent holding of children, and in women in the postpartum period due to the burden of caring for a child. Patients complain of pain at the base of the first finger and the inability to perform usual work.
A peculiar form of inflammation of the tendons and synovial sheaths of the forearm is crepitant tenosynovitis. Develops with frequent repetition of the same type of hand movements. Swelling and redness appear on the back of the forearm. A special symptom is crepitus (if you place your palm on the affected area and ask the patient to move his fingers, a peculiar crunching sensation is felt on palpation).
Tenosynovitis of the arm: shoulder, forearm and wrist joint
Acute tenosynovitis of the hand can be a consequence of increased physical activity. Tenosynovitis of the shoulder is often diagnosed in representatives of certain professions: hairdresser, builder, finisher, installer. And tenosynovitis of the forearm is more common among tailors, cutters, musicians and tennis players. Programmers and other people who work on a computer run the risk of developing tenosynovitis of the wrist joint, which in its symptoms will be similar to carpal tunnel syndrome.
Clinical manifestations of hand tenosynovitis will be as follows:
- nagging pain in the area of the affected tendon;
- severe limitation of limb mobility in the shoulder, elbow or wrist joint;
- decreased muscle strength;
- swelling, puffiness, pain on palpation;
- redness of the affected area.
The pain can be relieved with cold or non-steroidal anti-inflammatory ointment. However, full treatment requires an integrated approach and long-term rehabilitation.
Tenosynovitis of the extensor fingers of the hand
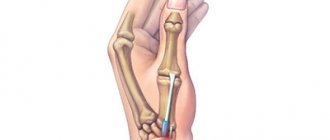
Tenosynovitis of the extensor fingers of the hand can affect either one or several extensor tendons. Since the skin is mobile, and inflammation is not accompanied by obvious pain, attention is paid to the pathology when a tendon rupture occurs.
If the conservative method of 4-month treatment is ineffective or the tendon ruptures, the doctor prescribes surgery, after which the patient is given a plaster cast for 14 days. After the first day after surgery, gymnastics is prescribed, aimed at developing movements in the free interphalangeal joints.
Sometimes a tendon transfer is performed. In this case, the donors are the extensor tendons of the other finger or the extensor carpi longus. This method is very effective and ensures complete restoration of limb function.