Hip endoprosthesis - structure and material
Structure of a total hip joint endoprosthesis - cup (acetabulum) with liner, stem and head replacement © Implantcast How important is the material and shape of the endoprosthesis in total hip replacement?
The hip endoprosthesis consists of four components:
- cup (acetabular component)
- fixed inside the liner
- legs
- head of the hip joint
There are a large number of models of hip joint endoprostheses, because... there is no ideal model. Each model has its own advantages and disadvantages. It is important for the patient that an experienced doctor selects a model individually for each patient. The cost and quality of endoprostheses from well-known manufacturers are approximately the same, but each doctor, after many years of work, has his own preferences. Even the most expensive model, if it is not installed professionally, will not stand and will begin to loosen. The most important thing for a patient is to make sure of the doctor’s professionalism. The Gelenk-Klinik Endoprosthetics Center employs only highly qualified specialists who perform more than 100 endoprosthetics operations per year.
What are the features of the operation?
The hip joint is very loaded and at the same time very mobile - movements in it are possible in completely different planes, which is ensured by its spherical shape. It is surrounded by very powerful muscles that help maintain an upright body position when walking.
The purpose of replacing the hip joint is:
- relief from pain and contracture (limited movement);
- restoration of the ability of the hip to bear the load of body weight and to move;
- restoration of equality of leg lengths;
- ensure long-term good functioning of the hip.
The success of endoprosthetics is ensured by the design and quality of manufacture of the endoprosthesis, and the use of the most durable materials.
As well as the optimal surgical technique, which causes minimal trauma to the muscle and tendon tissues surrounding the joint.
Hip endoprostheses are quite diverse. This is due to the large anatomical variability in the structure of the joint and the various forms of its damage. The correct choice of a suitable endoprosthesis is one of the most important components of achieving a good surgical result.
Endoprosthesis cup (acetabular component)
Inserts for hip joint endoprosthesis made of ceramic, polyethylene, metal with a special titanium coating in gold color © Implantcast
The cup of a cementless endoprosthesis always consists of two components:
- outer metal casing
- liner fixed inside
The liner can be made of ceramics, plastic (polyethylene) or metal
A model requiring cementation is rarely used in the orthopedic Gelenk-Klinik. This is usually a one-piece system made of plastic (eg polyethylene/polyethylene with or without weld metal network structure).
Cost and composition of hospitalization programs
| programs | |||
| hospitalization | for free | for free | 1,200-3,000 rub. in a day |
| operation | for free | for free | from 60,000 rub. |
| anesthesiological support | for free | for free | 20,000-30,000 rub. |
| endoprosthesis | for free | free or self-pay | from 60,000 rub. depends on the type of prosthesis |
| medication provision | for free | for free | from 15,000 rub. |
| need to wait | from 2 weeks to several months | from 2 weeks to several months | no more than 1-2 weeks |
| multi-bed ward | for free | for free | 1,200 rub. in a day |
| single room | 900 rub. per day | 900 rub. per day | 3,000 rub. in a day |
| total cost (if placed in a multi-bed ward) | for free | ONLY the endoprosthesis is paid for free | from 180,000 rub. |
| see details here | |||
Endoprosthesis femoral head
The femoral head of the endoprosthesis is mounted on the upper cone of the endoprosthesis stem and slides in the cup (acetabulum).
Cementless hip replacement stem © Implantcast
Such a sliding friction pair
may consist of various materials with varying hardness and surface texture. Today, the most commonly used combinations are ceramics with plastic, metal with plastic and metal with metal.
Their difference lies in their tendency to wear out and react to sudden peak loads.
Result of the operation
Endoprosthetics allows you to restore the function of the hip, and, consequently, the entire leg. There is a return to a full active life:
- pain stops;
- lameness disappears;
- the length of the legs becomes the same;
- free and painless movements become possible again;
- everyday and even sports activity is restored,
A modern, low-traumatic technique for performing the operation, ensuring the safety of all muscles, as well as the use of high-quality durable endoprostheses provides excellent results and completely eliminates pain and difficulty in movement.
The anesthesia methods used make the operation painless and safe, and modern means of rehabilitation ensure rapid and complete restoration of the function of the operated leg.
Return to normal activity and work is possible within 1.5-2 months after surgery.
Cementless fixation of the endoprosthesis
With cementless fixation, all parts of the endoprosthesis are in direct contact with the bone. Therefore, the surfaces of the prosthesis are specially coated and processed in such a way that the endoprosthesis grows into the bone. This process is called "Osseointegration". Special bone substitutes, such as hydroxyapatite and various titanium alloys, are used to cover the endoprosthesis. All components of the endoprosthesis are pressed into the bone using the so-called 'Press-fit-Technik' technique.
This process requires a certain preparation of the bone surfaces in contact with the endoprosthesis.
- To install the endoprosthesis stem, the medullary cavity of the femur is cut out with special cutters in the shape of the endoprosthesis. After this, the leg of the prosthesis is pressed into a previously prepared cavity, which makes it possible to quickly load the leg after surgery.
- When installing a cup, a so-called 'Press-fit' cup is often used. It is driven in and seems to get stuck in the bone, because... by its design, it is larger in size than the corresponding depression. Screw cups with self-tapping external threads that are screwed into the bone are not used at Gelenk-Klinik.
How is the operation performed?
Joint endoprosthetics is a high-tech operation that requires the operating surgeon to be highly qualified and have serious experience.
The operation consists of several stages.
Access
Technically, the operation consists of several stages. First, the so-called “access” to the joint is performed - this is a set of surgical methods, such as dissection and separation of the tissues of the limb, making the hip joint accessible for subsequent actions.
Access is no less important stage of the operation than subsequent ones. The volume of blood loss, the degree of preservation of muscles and ligamentous structures depend on the characteristics of the access; this subsequently affects the quality of rehabilitation.
Modern access techniques make it possible to minimize trauma to muscles and other tissues - this ensures rapid and complete restoration of motor functions.
Removal of altered joint structures
At the next stage of endoprosthetics, some parts of the joint are removed with a special tool and the bone structures are prepared for installation of the components of the prosthesis.
Installation of endoprosthesis
The components of the endoprosthesis are fixed to the bone. The process of their installation is perhaps the most important task for the surgeon, since the accuracy and durability of the endoprosthesis depends on the accuracy of his actions. For installation, either the “press-fit” fixation technique or using bone cement is used.
Suturing tissues
The operation is completed by suturing the tissues surrounding the joint in accordance with their normal anatomical relationship. Sutures or special staples are placed on the skin.
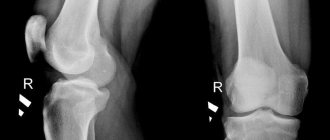
| 05. X-ray before surgery – Dysplastic coxarthrosis of the III degree. | 06. X-ray after endoprosthetics surgery. |
Cement fixation of the endoprosthesis
Bone cement is made by mixing liquid and powder during surgery to create a quickly hardening plastic that bonds the surface of the bone to the prosthetic components. This cementing method has improved significantly in recent decades. Until now, bone cement has been the weakest link in the prosthesis-cement-bone energy transfer chain. Today we use all technical capabilities to optimize the process and use the “Vacuum Cementing Method”.
Cement fixation of the hip joint endoprosthesis© Implantcast
Mixing of cement is carried out in a special vessel in a vacuum, for which a special pump is used. This reduces the number of air pockets in the cement during the curing process and therefore increases the strength of the cured bone cement.
Before applying the bone cement, the bone is cleaned using pulsed lavage. It is an irrigation pump that constantly injects water into a cap with a lid under low pressure. Water is simultaneously pumped out of this cap using suction. Contaminants such as blood residues, bone fragments and fat fractions are removed. This improves the contact between the bone surface and the surface of the endoprosthesis.
In addition, when cementing the stem, the medullary cavity of the femur is closed from below, so cement can be introduced under pressure without additional air entering the prepared cavity. This is achieved by using a special suction device to remove blood components and air from the surgical field.
Postoperative period
After surgery, as a rule, a stay in a specialized postoperative observation ward is indicated for 12 to 24 hours. Next - return to the regular ward. Within a few days, the necessary drug therapy and, most importantly, a set of rehabilitation procedures are carried out.
There is no need for long periods of bed rest. Activation begins on the first day.
The period of restrictions is short and the restrictions themselves are not so burdensome - it is enough to exclude some movements in the joint for a while (5-6 weeks) and limit the load on the leg when standing up and walking.
All this is achieved without much difficulty and without a feeling of discomfort.
A modern approach to rehabilitation guarantees complete restoration of joint function within a short period of time.
Here you can learn in detail about the rehabilitation method after surgery. If you're about to have surgery, download this helpful brochure ahead of time.
Discharge from the hospital usually occurs after 5-7 days. Stitches are removed on the 12-14th day.
Compliance with all conditions and recommendations of a specialist, a high-quality operation and a responsible attitude to the rehabilitation period can completely restore the functions of the joint, return you to freedom of movement and the opportunity to lead a full life.
Predisposing factors
BEFORE PREGNANCY:
Gynecological and other diseases of the expectant mother
(uterine anomaly, fibroids, anemia, rheumatic disease);
Poor nutrition and unhealthy lifestyle of the expectant mother
Unfavorable environment
Heredity for dysplasia.
DURING PREGNANCY:
Pathological course of pregnancy
(oligohydramnios, threat of miscarriage, toxicosis, taking medications)
Acute viral and other infections (
ARVI, influenza, syphilis, etc.), especially from 10 to 15 weeks of pregnancy.
DURING CHILDREN:
First or difficult birth
Features of the fetus
(large size, transverse position, breech presentation, multiple pregnancy)
AFTER CHILDBIRTH:
Tight swaddling
Why is excess weight dangerous?
In the older age group, the body mass index often exceeds the norm, which subsequently can interfere with implant healing. In addition, it is against the background of preobesity or obesity of the first/second degree that various pathological processes develop in the body, interfering with the normal course of the operation. Such patients often already have osteoporosis and fragility of bone tissue, heart problems (arrhythmia or tachycardia), and concomitant inflammatory processes.
Before going for endoprosthetics, it is better to lose extra pounds
| To main |
(Radiation Diagnostics News 1998 2: 19-21)
Read the article about X-ray diagnostics
acetabular dysplasia in issue 1 for 1998.
Ultrasound diagnosis of hip dysplasia.
Ulezko E. A., Buchel Yu. Yu., Fen E. P.
7th Clinical Hospital, City Consultative and Diagnostic Center for Children, Minsk.
Early detection of children with congenital dysplasia and congenital hip dislocation is an important task in modern orthopedics. After all, starting treatment for this pathology before 3 months in 97% of children leads to excellent and good results [1]. However, the generally accepted x-ray diagnostic technique still does not allow a full assessment of the condition of the joint in a child in the first three months of life.
Recently, in pediatric orthopedics in children of the first year of life, ultrasound examination of the hip joints has begun to be widely used, which allows, without the use of X-ray methods, to resolve the issue of the presence of dysplasia, subluxation or dislocation. This method eliminates harmful radiation exposure, including the gonadal dose received during X-ray examination of the hip joints. Ultrasound examination makes it possible to evaluate the cartilaginous structures that mainly comprise the hip joint in children in the first months of life, as well as muscle and connective tissue components. The method is non-invasive, it can be reused and functional tests can be used [2].
The head of the femur in children in the first months of life consists of cartilaginous tissue. The ossification nucleus of the femoral head often appears at 3-5 months. Ultrasound can detect the ossification nucleus several weeks earlier than x-ray. The cartilaginous portion of the femoral head weakly reflects ultrasound waves, providing a window for examining the acetabulum.
The acetabulum consists of unossified cartilage, which is visualized as a zone of reduced echogenicity, limited by the edges of the ilium and ischium.
Labrum consists of hyaline cartilage of low echodensity and a small amount of fibrinous cartilaginous tissue of higher echogenicity.
As the child grows, the bony margins of the acetabulum and proximal femur obstruct ultrasound penetration and are visualized as highly echogenic structures. Sometimes air is found in the joint cavity in the form of unstable spots of high echogenicity that disappear when the limb moves, which is regarded as a normal phenomenon.
The method of ultrasound examination of the hip joints and the ultrasound classification of their congenital pathology were first developed by the Austrian doctor Graf in 1984 and are now generally accepted [3,4].
Ultrasound examination of the hip joints is performed with a 5.0 or 7.5 MHz linear sensor. The child is laid on his side, the leg is bent at an angle of 20-30o at the hip joint, which allows you to get the best oblique cut. It is recommended to conduct the study in a special setting, which can be easily made independently from foam rubber or a blanket ( Fig. 1
). Since newborns do not have lumbar lordosis, the optimal scan can be obtained with the scanning plane (sensor) positioned parallel to the lumbar spine. The image of the joint should be obtained as close to the midline of the joint as possible. The sensor is installed in the projection of the greater trochanter. At the beginning of the study, it may be useful to move the transducer along the proximal femur, which is visualized on the transverse scan as a crescent of high echogenicity. Moving the sensor posteriorly allows you to obtain an image of the midline section of the femoral head, which has the shape of a spherical formation of reduced echogenicity. At least two high-quality scans of each joint should be taken for further comparison.
| Rice. 1. Position of the child during the study. Laying. |
Indications for ultrasound examination are: symptoms of “clicking” and “slipping” in the first week of life; limitation of hip abduction; asymmetry of the gluteal folds; shortening of the leg; violation of hip rotation; birth in breech position; increased muscle tone in the lower extremities; the presence of pathology of the hip joints in close relatives.
Normal ( Fig. 2
) the head of the joint is centered in the acetabular cavity.
The bony part of the roof is visualized almost horizontally, the cartilaginous part (limbus) is defined as a hyperechoic strip covering the head of the joint. The main line is drawn along the edge of the ilium, parallel to it, through the center of the acetabular cavity. The line of the bony roof passes through the bony prominence and the y-shaped cartilage and forms the alpha angle. The line of the cartilaginous roof is drawn through the bony prominence along the base of the limbus and forms the angle beta ( Fig. 3
).
| |||||||||||||||||||||||||||||||||||||||||||||||||
How is an ultrasound of a child’s joints performed?
The child lies on the couch, and the diagnostic specialist delicately moves the ultrasound machine sensor in the groin area. During the ultrasound, both hip joints are examined along with adjacent bone and soft tissue formations. To do this, the doctor turns the child from the back, either to the right or to the left side. In the ultrasound machine, the received ultrasonic impulses are converted into electrical ones and displayed on the monitor in the form of an image. In addition, the modern Japanese ultrasound diagnostic device used in our Center, along with ultrasound, allows us to conduct Doppler measurements - a duplex (double) study of blood flow in the artery circumflexing the femoral head. This gives the doctor additional information and allows you to prescribe the optimal course of treatment. The procedure is quick and comfortable for the child.
Each childhood age has its own norms and echographic features of ultrasound of the hip joints, and these norms are fundamentally different from adult indicators. The doctors of our Child Health Center have all the necessary equipment, as well as experience and knowledge, allowing them to take into account all the intricacies of conducting and interpreting a children’s ultrasound, so they can always choose the most effective therapy for the baby. Your task is to bring your child to the examination on time!
Useful!
|