Tendinopathy of the Patellar Ligament The term tendinopathy is a general designation for clinical conditions associated with excessive stress on the tendons and surrounding tissues. Histologically, this condition is characterized by random proliferation of tenocytes, destruction of collagen fibers and subsequent increase in non-collagenous matrix.
Clinically Relevant Anatomy
Healthy tendons are shiny white in color and have a fibroelastic structure. Tenoblasts and tenocytes make up 90%-95% of the cellular elements of tendons. The remaining 5%-10% of cellular elements include chondrocytes, tendon sheath synovial cells, capillary endothelial cells, and arteriole smooth muscle cells.
Oxygen consumption by tendons and ligaments is 7.5 times lower than that of skeletal muscles. A low metabolic rate and a well-developed anaerobic energy capacity are necessary to tolerate loads and maintain tension over long periods of time, reducing the risk of ischemia and subsequent necrosis. However, a low metabolic rate leads to slow healing after injury.
ACL plastic surgery
The cruciate ligaments are under constant tension, so applying sutures to restore their integrity is ineffective. Only in case of a Segond fracture is the integrity of the bone restored by fixing the torn fragment. For reconstruction, plastic surgery is performed using an autograft, that is, using the patient’s own tissues. This is usually the semitendinosus tendon. The efficiency of such operations is high. After completing rehabilitation measures, functionality is restored. However, plastic surgery is not required in all cases.
The need for it is based on:
- results of analysis of the intra-articular cavity, the absence of pronounced consequences of inflammation in the joint with extensive fibrosis and adhesions;
- presence of knee instability and other functional disorders;
- sports activity (the desire to return to sports with certain expected intense loads).
Plastic surgery is not performed immediately, but some time after the injury. However, it is not worth postponing the operation for a long time, since instability causes microdamage to the articular cartilage, which can result in the development of arthrosis. The key condition for surgery is the absence of internal inflammation. Preparation for surgery includes conservative treatment methods. Then plastic surgery is performed using the autotransplantation method. The rehabilitation period after such an operation is very important, and compliance with the recommendations of a rehabilitation physician plays a significant impact on the recovery process.
Epidemiology/Etiology
An injured tendon has a higher rate of matrix remodeling, resulting in mechanical instability and increased susceptibility to injury. The results of histological studies of samples taken from patients with established tendinopathy show either no or minimal significant inflammation. Typically, they indicate proliferation, loss of collagen fiber density, increased proteoglycan content, and neovascularization. Inflammation appears to play a role only in the initiation, but not in the spread and progression of the pathological process.
Previously, it was believed that failure to heal and the resulting tendinopathy of the tendon was associated with chronic overload, but subsequently the same histopathological characteristics were described in tendons that were not overloaded. Lack of load on the tendon is accompanied by the same changes in cells and matrix as in the case of an overloaded tendon. This also leads to a decrease in its mechanical strength.
Causes
The first signs can appear at any age. However, the problems more often concern bodybuilders, fitness enthusiasts and team sports. CrossFit techniques and all jumping exercises that lead to tendinitis of the lateral ligaments of the knee joint are considered potentially dangerous for the joints. Hence the name – “jumper’s knee”.
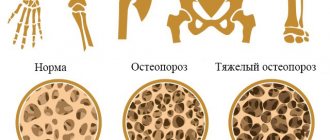
People 45+ have a higher risk of degenerative inflammation. The process is associated with age-related changes that develop due to calcium metabolism disorders, decreased collagen synthesis, and fatty bone degeneration. Inflammation of connective tissue structures is promoted by:
- long-term use of glucocorticosteroids;
- Hamstring syndrome - microtraumas;
- arthritis, deformity
- dying arthrosis of the knee, osteoarthritis;
- lupus erythematosus;
- polyarthritis;
- knee gout;
- scleroderma;
- gonococcal infection;
- Reiter's syndrome.
Provoking causes include flat feet, poor posture, anatomically incorrect location of the cups that pinch the nerves when lifting the leg above 60°.
Clinical picture
The main manifestations of tendinopathy are pain and decreased functional activity. The pain is usually associated with exertion. At an early stage, pain appears only at the beginning of physical activity and disappears during its process. Usually the patient is able to localize the painful area quite clearly. In the early stages, the pain is described as “severe” or “sharp,” and sometimes as “dull,” especially if the pain persists for several weeks.
Examples of tendinopathy include the following conditions: rotator cuff tendinopathy, lateral and medial epicondylitis, patellar ligament and Achilles tendinopathy.
Diagnostics
The doctor makes a diagnosis based on a history of sports or other injuries and a characteristic clinical picture. Additional examination methods (ultrasound, CT and MRI of the knee joint) are usually not required.
An x-ray of the knee sometimes shows slight thickening of the soft tissue. With ossifying tendonitis, there are foci of calcification.
Reference! CT, MRI and ultrasound are indicative of advanced stages of the disease. Ultrasound of the knee joint reveals a violation of the tendon structure. MRI and CT scans reveal ligament damage.
Laboratory tests are relevant for secondary symptomatic tendonitis. Rheumatoid diseases are indicated by anticiruline antibodies and rheumatoid factor, accelerated ESR, and metabolic pathologies are indicated by increased levels of creatinine and uric acid.
Most often, tendinitis is differentiated from injuries to the bone structures of the knee joint and rheumatoid diseases. The decisive method in this situation is the x-ray diagnostic method.
Physical examination
The examination includes examination for muscle atrophy, asymmetry, edema and erythema. Atrophy is often present in chronic conditions and is an important clue to the duration of tendinopathy. Also, when examining pathological tendons, swelling, erythema and asymmetry may be observed. Range of motion testing is often limited on the symptomatic side.
The physical examination should include tests that load the tendon to simulate pain and other stress tests that assess the condition of adjacent structures.
Physical therapy
The use of eccentric exercises has been proposed to accelerate tendon remodeling through the formation of interfiber bonds. What causes tendon healing in the eccentric mode is not known for certain, but it is assumed that the forces generated during eccentric loading are greater than during concentric exercises.
It is possible that eccentric exercise not only has a beneficial mechanical effect on the tendons, but also acts on pain mediators, reducing their presence in the affected tissues. In any case, the positive effects of eccentric exercise are evidenced by studies conducted on athletes and people leading a sedentary lifestyle.
However, there are many questions regarding what variables can influence the outcome of training: should the training be painful, how long should it be, what method of progression should be chosen, etc.
To date, three basic principles have been formulated for the eccentric training regime:
- Tendon length - if the tendon is pre-stretched, its length at rest will be greater, and the tension during movement should be less.
- Load – by gradually increasing the load on the tendon, we can expect an increase in its strength.
- Speed – Increasing the speed of contraction requires more force.
However, more research is needed to confirm these conditions.
Symptoms of tendinosis
Common symptoms of tendinosis include:
- pain during movement, which goes away with rest,
- passive movements of the limb are practically painless,
- palpation of the affected tendon is unpleasant, painful,
- it is compacted, redness is visible on the surface, an increase in temperature over the affected area,
- When moving, you can hear a crunching or crackling sound.
Depending on the location, there are characteristic features of tendinosis.
Tennis elbow (lateral epicondylitis)
- damage to the wrist extensors. In this case, pain occurs in the elbow area and radiates upward, into the shoulder, along its outer part and along the forearm. There may be weakness in the hand, difficulty in lifting cups, shaking hands or wringing out clothes.
Golfer's hand , baseball player's hand (medial epicondylitis)
– damage to the extensors and muscles that rotate the forearm. It manifests itself as pain in the inner part of the elbow, pain when bending the hand down, pressing on the hand.
Querwen's disease
– tendinosis of the tendons of the thumb, manifested by pain when extending and abducting the thumb. Pain when palpating the base of the thumb, as well as pain when connecting the pad of the thumb to the little finger.
Patellar tendinosis (jumper's knee)
– pain in the knee area, tendon swelling, swelling. Untreated tendinosis can cause patellar tendon avulsion.
Quadriceps tendinosis
resembles a patella problem, but usually occurs in older athletes.
Post-tibial tendinitis
with damage to the tibialis muscle it gives pain in the tendons, pain in the heel, in the arch of the foot. May lead to flat feet and heel spurs. The pain intensifies when running and carrying heavy objects.
Shock wave therapy
Extracorporeal shock wave therapy is an intervention based on the use of high-energy electromagnetic waves, which has recently become popular for the treatment of various diseases of the musculoskeletal system. It is most often used to treat tendinopathies.
ESWT is of interest to clinicians for two reasons. First, it stimulates the metabolic activity of the target cells, which promotes tissue healing. Secondly, it is assumed that ESWT has an effect on localized nociceptors, which leads to a decrease in pain intensity.
Acoustic shock wave signal transduction is converted into a biological signal, which leads to cell proliferation and/or differentiation. Most research regarding ESWT has focused on better understanding the mechanisms that lead to mechanosensitive feedback between acoustic impulses and specifically stimulated cells. However, the mechanisms that allow tissues to recognize and convert the intensity, frequency, amplitude and duration of an acoustic signal into a biological response are still not fully understood.
The effect of ESWT on pain intensity has also not been fully studied. It is believed that the mechanical effect is focused on the primary afferent nociceptive C-fibers, which are responsible for the sensitization of the affected tissues.
The rationale for the clinical use of ECVT remains the stimulation of soft tissue healing and the inhibition of pain receptors (nociceptors). There is no consensus regarding the use of low-energy extracorporeal shock wave therapy, which does not require local anesthesia, as opposed to the use of high-energy extracorporeal shock wave therapy, which requires local or regional anesthesia.
Although ESWT is popular in the rehabilitation world, the scientific rationale for treating specific pathologies, including tendinopathies, is still evolving. There are conflicting opinions in the literature in favor of the use of ESWT for tendon injuries.
Low Level Laser Therapy
There is no consensus regarding the use of low-level laser treatment for tendinopathies. There are also a number of unresolved problems associated with the use of low-level laser therapy in combination with other interventions, especially exercises, mainly in the tendon remodeling phase.
Iontophoresis and phonophoresis
Iontophoresis and phonophoresis involve the use of ionizing current or ultrasound to deliver drugs locally. Typically, corticosteroids and non-steroidal anti-inflammatory drugs are used for this purpose. Both methods are widely used, but all randomized controlled trials have failed to provide reliable evidence of their effectiveness.
Friction massage
There is currently little evidence to support the use of this method in the treatment of tendinopathies. In particular, a Cochrane review suggests that friction massage is not superior to other treatments for tendinopathies.
Ultrasound
Therapeutic ultrasound is widely used in the treatment of tendinopathies. Despite this, there are few clinical studies demonstrating the effectiveness of ultrasound in promoting tendon healing.
Most in vivo studies have confirmed the effectiveness of ultrasound treatment. However, in the era of evidence-based medicine, further research, especially randomized control trials, is needed to determine how effective ultrasound is in the treatment of tendinopathies.
There are only two pathologies in the treatment of which ultrasound has shown good results. These are lateral epicondylitis and calcific supraspinatus tendinopathy.
Hyperthermia
Early data on hyperthermia are encouraging but remain preliminary. Only two randomized clinical trials have been published that evaluated hyperthermia versus therapeutic ultrasound in the treatment of tendinopathies. These studies reported a decrease in pain intensity and improved well-being of patients in the hyperthermia group compared to the ultrasound group.
Rehabilitation
After arthroscopic plastic surgery, the patient goes home on the day of surgery. It is recommended to apply cold to the knee for 24 hours and immediately fix the leg with an orthosis. Then they begin to perform exercises, which are given with a gradual increase in load. Physical therapy is a set of exercises developed individually for each person. At first, the exercises are performed when visiting a clinic, then independently at home. Mechanotherapy - exercises on simulators are given in a later period of rehabilitation. Physiotherapeutic procedures, including electromyostimulation, magnetic therapy, and electrophoresis, also provide significant assistance. After arthroscopic surgery, recovery is faster and easier than after open knee surgery.
Forecast
The vast majority manage to fully restore the functionality of the limb after treatment and rehabilitation, and athletes are able to return to training. However, this is a rather slow process and takes about six months on average. It is important to adhere to the recommendations of specialists and not to provoke new injuries.
This patient suffered an ACL and collateral ligament injury 2.5 months ago. In this video, he is undergoing conservative treatment for anterior cruciate ligament injury. Subjectively, the knee is stable, but we continue to use various rehabilitation tools, such as flossing.