Varus and valgus deformities of the knee joints are pathologies of the development of the lower extremities that require timely treatment.
It is important to contact a pediatric orthopedist as soon as possible so that the doctor examines the child, conducts an examination, and does everything necessary to correct the defect. With early initiation of therapy, it is possible to correct limb deformities and avoid serious complications in the future.
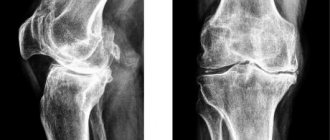
The varus form of the disease is more favorable than the valgus deformity, in which the knee joints are bent to the side. Bilateral lesions result in X-shaped legs. Varus deformity is accompanied by a pathological change in the shape of the legs, which take on an O-shaped appearance. This leads to sprained ligaments, increased load on the joint tissues of the lower extremities, and an increased risk of developing arthrosis, osteochondrosis, and flat feet.
When the first signs of deformation of the knee joints appear, you should contact a pediatric orthopedic traumatologist. Using X-ray diagnostic methods, it is possible to assess the condition of the skeletal system and determine further treatment tactics.
At an early stage of the disease, the effectiveness of conservative and surgical methods is quite high. The qualifications of the doctor play a huge role in the effectiveness of treatment procedures. At the CONSTANTA Clinic in Yaroslavl, consultations are conducted by pediatric orthopedists with many years of practical experience - MD. Vavilov M.A. and Ph.D. Gromov I.V. The specialists skillfully find an approach to each small patient and their loved ones, clearly and clearly explain the peculiarities of the course of the disease and the importance of timely initiation of treatment.
Clinic Constant. Information for parents of young patients.
Consultation
At the first appointment, the orthopedist assesses the degree of deformation of the knee joints, determines the form of the disease, and prescribes a comprehensive examination. After receiving all the necessary information about the child’s health status, the doctor selects a further treatment regimen. An accurate diagnosis can be made and varus or valgus deformity of the knee joints can be identified using X-ray diagnostics.
For out-of-town patients
Skype or email. a photo of the child’s feet and a short video that clearly demonstrates walking
to [email protected]
Symptoms and course of the disease
Varus deformity is characterized by uneven development of the knee joints. In this case, the external condyle of the femur increases, and the internal one decreases. This leads to the compression of the internal meniscus, and the joint space becomes wider on the outside and narrower on the inside. The ligaments that strengthen the knee joint are stretched, especially on the outside. The lower leg is curved with a convexity outward. In advanced cases, the hip rotates outward and the shin rotates inward. The feet acquire a flat-varus position: the heels and forefoot are deviated inward. At the same time, clubfoot develops. The child cannot fully extend his knees, this is especially noticeable when viewed from the side. Correction of such curvature of the legs is mandatory, since with further progression a gait disturbance occurs, the child often falls and gets tired quickly. In addition, in this situation the spine suffers: various posture disorders and even scoliosis occur
Features of treatment
Depending on the age of the small patient and the stage of varus or valgus placement of knee joints, the following is carried out:
Conservative therapy
Used at an early stage of the disease. Massage, physical therapy, custom orthoses and the use of orthopedic insoles are the main methods of non-surgical treatment and correction of crooked joints. Using conservative methods, it is possible to partially restore the functionality of the tissues of the limbs, strengthen the ligaments, and form a muscle corset using special exercises. It is important to identify concomitant diseases (rickets) and predisposing factors in order to solve the problem comprehensively.
Surgical intervention
Before 4 years of age, they try not to use surgical methods. Upon reaching this age, if conservative methods are ineffective, hemiepiphysiodesis is used - a surgical correction in which a minimally invasive temporary blocking of the bone growth zone is performed.
For varus and valgus deformities of the knee joints, this method is most effective. It does not affect the child’s quality of life, but at the same time, in a few years it allows you to completely restore the correct shape of the knee joints.
, , . . . .
How does a child develop? Smooth legs (X- and O-shaped) - when? What should parents know about flat feet, club feet, bowed legs and shoes? (great article for everyone!)
Author: Lynn T. Staheli "Practice of Pediatric Orthopedics"
Terminology
Version - a normal version of limb rotation. The rotation of the tibia is the angle between the axis of the knee joint and the transmaleolar axis (the axis drawn through the ankles of the tibia). Normally, the shin is turned outward. The rotation of the femur is the angular value between the axis drawn through the femoral neck and the transcondylar axis (axis drawn through the femoral condyles). Normally there is anteversion of the femoral neck. Torsion is described as being greater than two standard deviations from the mean and is considered abnormal and is described as a deformity. Torsion deformity can be simple, involving one level, or complex, involving many segments. Complex deformations can be additive (several deformations reinforcing each other) or compensating (reducing each other). For example, internal calf torsion and internal thigh torsion are additive. On the contrary, the external torsion of the lower leg and the internal torsion of the thigh are compensatory.
Normal development
The lower limb rotates medially during the seventh week of gestation, rotating the big toe toward the midline of the body. As the fetus develops, femoral anteversion decreases from 30° at birth to 10° during maturation. The magnitude of anteversion is higher in females and in some families. With growth, the tibia rotates outward from 5° at birth to 15° by the period of maturation. Because both the femur and tibia rotate externally as the limb grows, internal tibial torsion and femoral antetorsion improve over time in children. In contrast, lateral (outer) torsion of the lower leg usually worsens over time.
Fig. 1 The lower limb rotates outward with age. Both the femur and the lower leg (tibia) rotate outwardly with age.
Survey
Although the diagnosis of torsion deformity can be made simply by external examination, the history of the development of the deformity helps to rule out other problems and understand the extent of the disorder.
HISTORY OF DEVELOPMENT
Ask about the onset, severity, impairment, and previous treatment of the problem. Find out how the patient developed. A delay in the onset of walking may raise suspicion for a neuromuscular disorder. Do you have any similar rotational disorders in your family? Often rotational deformities are hereditary and the current condition of the parents can predict the future of the child.
Fig. 2 Internal torsion of the hip, which is present in both mother and child. Examination of parents often reveals deformities similar to those present in their child.
ROTARY PROFILE
The rotation profile provides the information needed to determine the level and severity of any torsion problem. Note the degrees for both sides.
Examine in 4 stages: Examine how the child walks and runs.
Estimate the foot progression angle (FPA) when walking. FPA is the angle between the axis of the foot and the direction of movement. This value is usually determined while the child is walking along the clinic corridor. Determine the average amount of inward or outward deviation of the fingers. Negative values are assigned to inward deviation of the toes. Inward rotation of the fingers (Intoeing) from -5° to -10° mild, -10°-15° moderate, more than -15° severe. Ask your child to run. A child with hip antetorsion “rakes” with his legs (“eggbeater” running pattern), deviating his feet outward during the swing phase.
Fig.3 Angle of foot deflection when walking. Determined by observing the child's gait. Normal values are shown in green.
Determine hip rotation (femoral version)
by measuring rotational movements in the hip joint. Measure external and internal rotation with the child in the prone position with the knees bent to a right angle and the pelvis level. Detect movements from both sides simultaneously. Internal rotation is normally less than 60°-70°. If rotation is asymmetrical, order x-rays.
Fig.4 Rotation in the hip joints (HJ). Rotation in the hip joint is determined by the child's position on his stomach. Internal and external rotation are measured. Normal range of motion is shown in green.
Calculate tibial rotation
by measuring the hip-foot angle (TFA). TFA is defined in a prone child as the angle between the intermalleolar axis and the femoral axis. In this way, tibia rotation is measured. The difference between TMA and TFA shows rearfoot rotation. The range of normal values is wide, and the average values increase with increasing age. Foot placement is very important for these measurements. Allow the foot to settle into its natural position, do not position the foot yourself as this will cause measurement errors.
Fig.5 Study of the rotational status of the lower leg and foot. The rotational status of the leg and foot is best determined by examining the child in the prone position, allowing the foot to move into its natural position. In this position, it is easy to determine the hip-foot angle and the shape of the foot. Normal values are shown in green.
Examine the foot
for adduction of the anterior section. The outer edge of the foot is normally straight. Curvature of the outer contour of the foot and adduction of the forefoot are usually symptoms of adducted foot (metatarsus adductus). An everted (outwardly turned) foot or a flat foot is usually the cause of outward turning of the toes. Include this data in your rotation profile. Based on the screening study and compilation of the rotational profile, establish the level and degree of torsion deformation.
Fig. 6 Diagram for determining the reasons for turning the toes inward or outward. Using a screening study and a rotational profile, it facilitates diagnosis.
SPECIAL METHODS OF INVESTIGATION
Perform additional examinations if hip rotation is asymmetrical or if rotation problems are so severe that surgical correction is considered. Before surgical treatment, take photographs to determine the degree of antetorsion in order to exclude hip dysplasia and measure the antetorsion of the hip (this means, apparently, antetorsion of the femoral neck - translator's note). Measurements are carried out according to CT or radiography in 2 projections. Typically, antetorsion exceeds 50 degrees in patients requiring surgical treatment.
Fig. 7 Asymmetrical range of rotational movements in the hip joints (HJ) requires further examination. This 12-year-old girl complained of inward turning of her toes. The rotational profile was abnormal, showing asymmetry of rotational movements in the hip joint. X-ray of the pelvis showed severe bilateral hip dysplasia (arrows). Surgical treatment of hip dysplasia was performed.
Principles of treatment
The first step is to make a correct diagnosis. When treating rotational limb problems, the most difficult part is finding good communication with the patient's family. Because the lower extremities rotate outward (laterally) over time, inward rotation of the toes spontaneously corrects in most children. Attempts to control the child's gait, sitting, or sleeping position are impossible. Such attempts only create tension in the relationship and conflict between the child and parents. Slanted insoles or inserts are ineffective.
Fig.8 Ineffectiveness of oblique insoles. Slanting insoles of various shapes were placed in the shoes (shown in black). Shown are the average values of inward rotation of the toes in children who wore insoles and in the control group who did not wear insoles. Reproduced with permission from Knittle and Staheli (1976).
By analogy, daytime braces with twister cables only limit the child’s ability to walk and run. Night splints that laterally rotate the feet are better tolerated and do not interfere with the child's play, although they probably have little long-term benefit. Thus, follow-up is best. Parents need to be convinced that observational treatment is sufficient. Observation of the child includes a thorough study, collection of information, repeated checks of the correctness of the diagnosis and examinations over time. Parents should be informed that cases where the deformity does not go away are quite rare. Less than 1% of torsion deformities of the hip and tibia do not resolve on their own and may require surgical correction in late childhood. There is rarely a need for derotational osteotomy, which is quite effective.
Fig. 9 Lack of effectiveness of braces with twisting elastic inserts (twister cables). The chart compares the effectiveness of “treated” results compared to those of untreated children with antetorsion. Treatment attempts have no effect on pre- and post-treatment femoral neck anteversion measurements. From Fabry et al. (1973).
INFANT (BEFORE WALKING - INFANT)
Turning the toes outward
may be a consequence of planovalgus foot or, more often, due to external rotation contracture of the hip joints or a combination of both factors. Inward rotation of the toes occurs due to adducted big toe, adducted forefoot, or internal torsion of the shin.
External rotation contracture of the hip joint
Due to the fact that the hips are rotated (expanded) outwards while the fetus is in the uterus, lateral rotation of the hips is normal. When a child is in an upright position, his feet may turn outward. This may worry parents. Often only one foot is turned outward, usually the right one. Of the two feet, the one that is turned outward is usually normal. The opposite leg, which parents consider normal, often has forefoot adduction or internal tibia torsion.
Fig. 10 Physiological infantile outward rotation of fingers. Outward rotation of the fingers in early infancy occurs due to external rotation contracture of the hip joints. In this infant, internal rotation is limited to 30° (top photo), while external rotation is limited to 80° (bottom photo). It is the result of external rotation of the limbs, which resolves spontaneously over time.
Adducted first toe
usually described as both a spastic contracture of the abductor hallucis muscle and a “searching toe”. It is a dynamic deformity due to relatively excessive tension in the abductor hallucis muscle that occurs during the stance phase. This deformity may be associated with adduction of the metatarsals. This condition goes away on its own during the maturation of the nervous system, when a more precise balance of the foot muscles is established. Does not require treatment.
Fig. 11 “Searching finger” (“serchin toe”). Dynamic deformation due to excess stress adductor hallucis
Forefoot adduction
– a spectrum of various deformities, characterized by medial deviation of the forefoot of varying degrees. The prognosis is closely related to foot rigidity.
Fig. 12 Severity of forefoot adduction. Draw a line that divides the heel in half. Normally it crosses the 2nd finger. This line passes through the 3rd finger for mild, between the 3rd and 4th for moderate, and between the 4th and 5th fingers for severe deformity. From a study by Bleck (1983)
Metatarsal adduction (Metatarsus adductus)
It is a flexible deformity and occurs due to the constrained position of the fetus in the uterus. Like other deformities, it resolves spontaneously over time. Most deformities are corrected during the first year of life, the rest in the subsequent period of childhood. Requires regular monitoring and repeated checks of the condition of the foot. No braces, casting, special shoes or exercises are required.
Varus adduction of the foot (Metatarsus varus)
Rigid forefoot adduction with a tendency toward no improvement. This rigid foot shape is uncommon compared to the normal adducted foot (metatarsus adductus). Varus adduction of the foot is characterized by rigidity with the presence of a fold on the plantar part of the foot. Foot development is often accompanied by incomplete spontaneous correction. The deformity does not cause functional impairment and is not the cause of corns. This pathology creates a cosmetic defect and, if severe, difficulties in choosing shoes. Don't forget about the deformity known as skewfoot. “Sickle foot” occurs in children with weakened ligaments of the joints and is characterized by pronounced adduction of the forefoot in combination with valgus of the hindfoot. Most parents want the deformity to be corrected. The deformity is corrected by staged casting of the leg to the groin area, starting at approximately 6 months. Plaster casts are applied at intervals of 1-2 weeks until the foot is corrected. In children over 2 years of age, correction with plaster casting is sometimes effective, but is more difficult for the child and parents to accept. Surgical treatment is very rarely necessary, since varus adduction of the foot (metatarsus varus) does not cause functional impairment or secondary deformities.
AGE AFTER STARTING WALKING (TODDLER)
Internal rotation of the toes is more common in the second year of life and is usually detected when the infant begins to walk. This deformity occurs due to internal torsion of the lower leg, adducted foot (metatarsus adductus) or adducted big toe.
Internal torsion of the leg (ITT).
VTG is the most common cause of inward rotation of the fingers. Often it is two-sided. If the VTG is unilateral, then it is more often on the left. Dynamic observation is the best treatment option. Fillauer or Denis Browne night splints are widely prescribed, but they do not matter in the long-term prognosis of treatment. Recovery occurs both with and without treatment.
Fig. 13 Bilateral internal torsion of the lower leg. Hip-foot angle is negative (red line) for both legs
Fig. 14 Unilateral internal torsion of the lower leg. Internal torsion of the lower leg is often asymmetrical and is usually worse on the left side
Avoid daytime braces and special shoes because they slow your child's movements and can damage their self-esteem. Correction occurs spontaneously, but often takes 1-2 years. Warn parents that the time required for correction is calculated in years and not weeks or months.
AGE AFTER 2 YEARS. (CHILD)
Inward rotation of the toes in childhood after the start of walking (after 2 years) most often occurs due to antetorsion of the thigh (femoral neck) and rarely due to persistent internal torsion of the lower leg. In late childhood, outward rotation of the toes may be due to external torsion of the thigh or external torsion of the lower leg. The natural development of the femur is an outward rotation of the femur as the child grows, which often leads to correction of the internal torsion of the tibia and worsening of the external torsion of the tibia.
Internal torsion of the leg (ITT)
less typical than external torsion for older children. In a child over 8 years of age, VTG may require surgical correction if it does not resolve on its own and produces significant functional impairment and cosmetic deformation. Surgical treatment may be indicated when the hip-foot angle is internally rotated by more than 10°.
Fig. 15 Persistent torsion of the lower leg. Rotational deformities do not always go away with time. This girl still has torsion of the lower leg (see arrow), which causes functional impairment and requires surgical correction (derotational osteotomy of the lower leg bones).
External torsion of the tibia (ETT)
Because the tibia rotates laterally (outward) with age, internal tibial torsion (ITT) improves, and external tibial torsion (ETT) worsens. IGT can cause pain in the knee joint. This pain occurs at the patellofemoral joint and is thought to be caused by an imbalance in the relationship between the knee axis and the line of progression. This violation of the ratio is most clearly manifested when the external torsion of the lower leg is combined with the internal torsion of the thigh. The knee joint is rotated inwards, and the ankle joint outwards, both joints are out of alignment with the line of motion, which causes “malalignment syndrome”. This condition leads to gait disturbance and pain in the patellofemoral joint.
Femoral antetorsion
Antetorsion of the femur (more precisely, the neck of the femur) or internal torsion of the femur is usually first detected in the age group of 3 to 5 years and is most common in girls. Often, residual effects of hip antetorsion are observed in the patient’s parents. A child with femoral neck antetorsion sits in the “W” position, stands with his knees turned inward (“kissing patella”) and runs awkwardly with an “egg-beater” gait. Internal rotation in the hip joint exceeds 70°. Internal hip torsion is considered mild if internal rotation in the hip joint is about 70°-80°, moderate at 80°-90°, severe at 90° or more. External rotation in the hip joint decreases accordingly, because the full range of rotational movements in the hip joint is 90-100°. Femoral antetorsion is usually most pronounced between 4 and 6 years of age and then normalizes. Recovery occurs due to a decrease in the angle of anteversion of the femoral neck and lateral rotation of the tibia. In an adult, hip antetorsion does not cause degenerative arthritis (arthrosis) and rarely causes functional impairment. Femoral neck antetorsion cannot be treated conservatively. The persistence of severe antetorsion over the age of 8 years may be an indication for derotational osteotomy of the femur.
Fig. 16 Internal (medial) torsion of the femur. This girl has internal hip torsion. Her patellas are rotated medially in a standing position. External rotation in the hip joint is 0° (top photo). External rotation in the hip joint is 90° (bottom photo).
Retrotorsion of the hip
may be more of a problem than is generally recognized. Retrotorsion is most common in patients with epiphysiolysis of the femoral head. Presumably the “shearing” force acting on the growth zone increases. Retrotorsion is associated with an increased risk of developing degenerative arthritis (arthrosis) and a gait with the toes turned outward. Gait problems are usually not severe enough to require surgical treatment.
Cost of treatment of varus and valgus legs
You can receive qualified medical care in our Clinic:
- for free . Charitable support from Rusfond allows the CONSTANTA Clinic to provide free surgical treatment for children with pathologies of the musculoskeletal system;
- at your own expense . The cost of treatment at your own expense, indicated at the bottom of the page, may vary and depends on the characteristics of the clinical case, the volume and complexity of medical care.
After consultation with a specialist, the exact cost of treatment will be calculated.
Personal manager
Patients of our Clinic can use the “Personal Manager” service free of charge.
A trained employee will be responsible for providing information support to the patient and resolving issues related to the preparatory and rehabilitation stages, consultations and explanations of the progress of the upcoming surgical intervention. Plot in the Good Morning program on Channel One about the treatment of clubfoot at the Constanta Clinic. Guest of the Health program with Elena Malysheva Vavilov Maxim Aleksandrovich Treatment O- and X-shaped legs. Hemiepiphysiodesis. CONSTANTA Clinic through the eyes of a child! Anesthesia for operations in children Treatment of children with the support of the Charitable Foundation