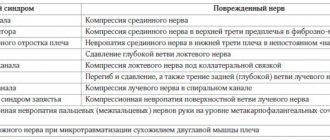
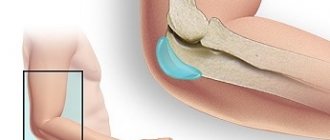
Ulnar nerve compression (UCN) can occur in two places: at the elbow and at the wrist. SLN at the elbow joint occurs in the cubital tunnel (cubital tunnel syndrome). Ulnar nerve neuropathy in the cubital tunnel is the second most common compression neuropathy (the first most common neuropathy is associated with entrapment of the median nerve in the carpal tunnel). Ulnar neuropathy is less commonly seen in Guyon's canal (Guyon's canal syndrome/ulnar carpal syndrome).
Causes
SLN in the cubital and Guyon's canals occurs due to repetitive compression due to support on the elbows or wrists (cyclist's palsy) or prolonged flexion of the elbow. It can also occur due to trauma, swelling, fracture, vascular and bone pathologies/disorders.
Ulnar carpal syndrome occurs when the ulnar nerve becomes compressed between the hook of the hamate bone and the transverse carpal ligament. Guyon's canal syndrome is considered an overuse injury that is typically caused by direct pressure on the handlebars (eg, bicycle handlebars, weight lifting, heavy equipment) and is thus sometimes referred to as "steering wheel palsy." This syndrome may also result from intense gripping, rotation, or repetitive movements of the wrist and hand. Impingement can develop if the hand is flexed and the elbow is abducted for an extended period of time.
The incidence of injuries leading to ulnar nerve compression is unknown; however, ulnar neuropathy has been documented after distal humerus fractures, of which up to 10% are associated with elbow dislocation, and can also develop following any complex trauma to the elbow or wrist.
If left untreated, danger
When a person does not address such a problem for a long time, the numbness becomes persistent. There is a disturbance in the movements of 1 finger of the hand when grasping and holding a large object. Precise movements with all fingers become rough, which greatly affects the work of those people who are engaged, for example, in engraving, jewelry making, manicure, etc., that is, where the required smooth, controlled movements of the fingers and brush are needed
The article was written by orthopedist-traumatologist Alexander Konstantinovich Silaev.
Clinical picture
Symptoms of ulnar nerve compression include tingling in the 4th and 5th fingers, weakness when grasping objects with the hand, pain and tenderness in the ulnar aspect of the wrist, forearm and hand, muscle atrophy, and inability to straighten the 4th and 5th fingers (a sign of blessing).
Cubital tunnel syndrome can manifest itself in varying degrees of severity:
Grade I: Mild symptoms such as:
- Periodically occurring paresthesia.
- Some decrease in sensitivity of the dorsal and palmar surfaces of the fifth and medial parts of the fourth fingers.
- No movement disorders.
Grade II: Moderate and persistent symptoms such as:
- Paresthesia.
- Hypesthesia of the dorsal and palmar surfaces of the fifth and medial parts of the fourth fingers.
- Mild weakness in the muscles innervated by the ulnar nerve.
- Early signs of muscle atrophy.
Grade III: Severe symptoms such as:
- Paresthesia.
- There is obvious loss of sensation on the dorsal and palmar surfaces of the fifth and medial aspects of the fourth fingers.
- Significant functional and motor impairments.
- Muscular atrophy of the deep muscles of the hand.
- Inability to straighten the fourth and fifth fingers (a sign of blessing).
Symptoms of Guyon's canal syndrome include:
- Muscle atrophy - mainly in the hypothenar and interosseous muscles, without affecting the palmar muscles:
- weakness when abducting and adducting the fingers (interosseous muscles);
- weakness in adduction of the thumb (abductor pollicis muscle).
- Sensation loss and pain that may involve the palmar aspect of the fifth finger and the medial aspect of the fourth finger, but the dorsal and medial aspect of the fourth finger and the dorsal aspect of the fifth finger do not lose sensation.
- The symptom of a “clawed” hand (a sign of blessing) may be present.
Symptoms of ulnar nerve neuropathy
- the elbow and arm become weak;
- obvious motor impairments, when it is impossible to move the elbow or the whole arm;
- decreased hand sensitivity;
- the little finger and ring finger go numb;
- when a person makes a fist, the fingers do not touch the palms;
- when the patient puts his hand on the table, it becomes difficult for him to lift or even move his little finger;
- the shape of the hand becomes similar to a “bird’s paw” due to developing atrophic processes.
To confirm the diagnosis against the background of these symptoms, the neurologist performs tests. MRI diagnostics may also be needed to determine the level and nature of the lesion.
Physiotherapeutic examination
Elbow carpal syndrome: It is important to rule out other diagnoses that may be related to the elbow joint. Physical examination includes:
- Assessment of range of motion of the wrist and fingers.
- Manual muscle testing of the ulnar nerve muscles innervated distal to Guyon's canal.
- Sensory examination of the cutaneous branches of the ulnar nerve distal to Guyon's canal
- Assessment of atrophy of the deep muscles of the hand.
Friends, on April 11-12 in Moscow there will be a seminar by Anna Ovsyannikova “Fundamentals of anatomy and biomechanics of the hand. Diseases and injuries of the hand and fingers." Find out more...
Special tests
- "Card" test.
- Froment's sign
- Tinnel's sign in Guyon's canal.
- The Ulnar Nerve Neurodynamic Test (ULTT3) may increase the patient's symptoms.
Diagnostic tests to determine ulnar nerve compression
- Visualization of osteoarthritis, osteophytes or bone cysts.
- Nerve conduction studies (EMG).
- If there is a suspicion of a fracture/dislocation, a plain X-ray.
Arthroscopy of the elbow joint
Postoperative period
After surgery, you will spend 1-2 hours in the recovery room before being discharged home. Nurses will monitor your condition and provide pain relief if necessary. When you are discharged, you will receive instructions on what to do next, what medications to take, whether you need to use ice or an elevated position on your elbow, and how to care for your cast. Then it is advisable to have someone drive you home (you are not allowed to drive yourself) and stay at home with you for at least one night.
At home
The recovery period after arthroscopic procedures is usually shorter than after open surgery, but you still should not expect full recovery before a few weeks.
You will experience some degree of pain or discomfort for at least the first week after surgery. With more or less extensive interventions, even arthroscopic ones, the pain will completely disappear only after a few weeks. Your doctor will likely prescribe pain medications for you to take regularly for the first few days after surgery. Additionally, you may be prescribed other medications, such as stool softeners or anti-inflammatory drugs.
For the first 48 hours after surgery, it is recommended to apply ice to the elbow joint and keep the arm in an elevated position. This will reduce the severity of swelling and reduce pain. An elevated position means that your hand should be above the level of your heart when you lie down. Depending on the specifics of the surgery, your doctor may recommend ice and elevation for a longer period.
You will most likely be advised to regularly exercise your fingers and wrist joint to improve blood circulation in the limb and reduce swelling. To prevent contracture of the elbow joint, the doctor may recommend starting to restore movement in the elbow joint as early as possible. When you can begin these exercises, and when you can return to normal daily activities, depends on the nature of your surgery.
Care of the dressing is also determined by the nature of the intervention performed, as well as the preferences of the surgeon. In most cases, the postoperative bandage and/or splint is removed 2-3 days after surgery. During this period, you should not touch the bandage and keep it dry. In some cases, you will only be advised to change the dressing at your first post-operative office visit.
Rehabilitation
Rehabilitation is a critical component of your return to daily life as quickly as possible. Special exercises will help you restore muscle strength and mobility of the elbow joint as quickly as possible. Depending on the specifics of the intervention performed, you will be offered an individual rehabilitation plan.
In some cases, your doctor will teach you or someone in your family basic exercises to do at home in the first days after surgery. In more complex situations, rehabilitation treatment is prescribed in a specialized center to speed up the recovery of movements, muscle strength and function of the elbow joint. The nature and duration of treatment depends on the nature of your problem and the type of surgery performed.
Returning to driving, basic daily activities and work will also depend on the nature of your surgery and should be discussed with your doctor before surgery.
Possible complications
Most patients who undergo elbow arthroscopy do not experience any complications, however, as with any other surgery, arthroscopy is associated with certain risks. If complications do occur, they are usually minor and respond well to treatment. However, many studies have reported that the risks of infection and nerve damage are higher with elbow arthroscopy compared to arthroscopy of, for example, the shoulder and knee joints. Possible problems with arthroscopy include infection, bleeding, thrombosis, and injury to blood vessels and nerves.
Before surgery, be sure to discuss with your surgeon the risks of possible complications in your particular case.
Criteria for evaluation
- Disabilities of the Arm, Shoulder, and Hand (DASH) is a 30-question questionnaire designed to assess patient function and symptoms.
- The Patient Specific Functional Scale (PSFS) is a questionnaire used to assess a patient's activity limitations and functional outcomes.
- The DASH assessment criteria are a questionnaire that assesses a patient's functional ability and symptom severity.
- The Upper Extremity Functional Inventory (UEFI) is a 20-question questionnaire designed to measure the severity of complex tasks performed throughout the day.
Physical therapy
- An impairment assessment approach may be used to identify strength deficits, decreased range of motion, and problems in achieving functional goals.
- The source of pain must be treated in conjunction with the disorder.
- After treatment, re-evaluate the functional tasks that caused pain to determine the effect of treatment.
- Create an exercise program to do at home to treat impairments and perform functional tasks.
A study conducted by Swernlov compared three types of treatment for patients with elbow tunnel syndrome. All three groups showed positive results; the control group showed similar improvement as the intervention groups.
- Splint group protocol —patients wore an elbow splint every night for 3 months to prevent elbow flexion greater than 45 degrees.
- Neural glide protocol – patients did neurodynamic exercises twice a day in six different positions, which were held for 30 seconds (three sets); the break between repetitions was 1 minute. Patients were instructed how to perform these exercises until their next follow-up visit, which was 1–2 weeks later. If no symptoms were found at the next visit to the doctor, the frequency of exercise was increased to three times a day with the position held for 1 minute (every day for 3 months).
- Control Group Protocol – The control group received only educational recommendations.
According to a study report by Coppieters, administration of elbow joint mobilization, thoracic spine and rib thrust manipulation, and ulnar nerve glide/tension techniques for 6 sets was associated with a reduction in elbow pain and a significant improvement in scores on a self-assessment questionnaire. cervical spine for at least ten months of observation. Patients reported a history of symptoms in the two months prior to physical therapy.
Treatment of ulnar nerve neuritis
Treatment of ulnar neuritis is carried out in several directions:
- If the disease is caused by a bacterial infection, antibiotics are prescribed; if it is caused by viruses, antiviral drugs are prescribed.
- If the underlying cause is vascular disorders (the nerve does not receive enough oxygen and nutrients due to impaired blood flow), vasodilators are used.
- If the neuritis is associated with injury, you need to unload the affected arm. For this purpose special tires are used.
- To combat pain and inflammation, the neurologist prescribes drugs from the group of non-steroidal anti-inflammatory drugs (diclofenac, ibuprofen).
- To reduce nerve swelling, diuretics are prescribed: diacarb, furosemide.
- Physiotherapeutic procedures are usually prescribed towards the end of the second week of the disease. Pulse currents, UHF, ultraphonophoresis with hydrocortisone, electrophoresis with novocaine are used.
The best results are obtained if treatment is started in the early stages, as soon as the first symptoms appear. If, despite the therapy, there is no improvement after 1-2 months, the neurologist may raise the question of surgery.
When the first symptoms occur, do not delay visiting a doctor. The earlier treatment is started, the better the result can be achieved. Book a consultation with a neurologist now. At the medical center International Clinic Medica24, this can be done at any time of the day by phone.
Take care of yourself, book a consultation now
Message sent!
expect a call, we will contact you shortly
The ulnar nerve has a mixed structure: it consists of motor, sensory, autonomic (responsible for the regulation of blood circulation, the work of the sweat and sebaceous glands, and other functions) fibers. It performs the following functions:
- Bending the hand.
- Flexion of the little finger and ring finger, partly the middle finger.
- Spreading and closing the fingers.
- Adduction of the thumb.
- Sensitivity of the inner (ulnar) part of the hand, little finger, partly ring finger, sometimes middle finger.
Accordingly, with ulnar nerve neuritis, symptoms are associated with a violation of these functions. They can be identified and correctly assessed by a doctor during a neurological examination.
Differential diagnosis
The cervical spine and shoulder girdle should be examined to rule out diagnoses that may relate to the elbow joint. There are many differential diagnoses for ulnar nerve entrapment.
- Elbow fracture/dislocation.
- Cervical radiculopathy.
- Thoracic outlet syndrome.
- Peripheral vascular disease.
- Damage to the collateral ligament of the elbow joint.
- Rheumatoid arthritis.
- Medial epicondylitis.
- Acute polyradiculoneuritis (Guillain-Barré syndrome).
- Neuropathy associated with alcohol (ethanol) consumption.
- Amyotrophic lateral sclerosis.
- Tumor of the apex of the lung.
- Primary bone tumors.
- Peripheral polyneuropathy.
Key Points of Physical Therapy
- Special tests used in diagnosing ulnar nerve entrapment have very high sensitivity - 0.98 or higher - and are therefore very useful in making the diagnosis.
- Conservative treatment is effective in approximately 50% of cases, while surgery is effective in 60-95% of cases.
- Conservative treatment has been shown to be effective when introducing the use of orthoses and manual therapy, including neurodynamics and joint mobilization; however, a recent study highlighted that more research is needed to know when conservative versus surgical treatment is needed.
- A patient who begins conservative treatment earlier has a 30% higher chance of avoiding surgery.
Effective treatment for ulnar nerve neuropathy
It is important! Treatment is selected based on the causes of the disease. Basically, the following methods are used:
- hand fixation to limit mobility;
- physiotherapeutic procedures;
- massotherapy;
- manual therapy;
- physical therapy for recovery;
- taking medications.
You will always be provided with comprehensive assistance at Medical. You can make an appointment with a specialist by phone. Do not tolerate pain, which with the right approach can always be eliminated by determining the exact cause of the disease and undergoing comprehensive treatment.