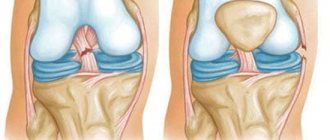
Causes and symptoms of ulnar collateral ligament injuries
The above ligament is commonly injured during certain sports
such as javelin throwing, baseball, football, rugby, tennis and volleyball, after elbow dislocation or during surgery. During sports, a person violates the correct throwing mechanics and gets injured.
Pain occurs on the inside of the elbow, especially with movements simulating an attempt to throw a ball. During an injury, a characteristic click
or crackling. After about a day, swelling and hematomas appear on the inside of the forearm. The elbow feels stiff and cannot be fully straightened. The fingers become numb and it is difficult to perform small movements.
Diagnostics
The diagnosis is made on the basis of: examination, anamnesis, instrumental diagnostics and tests.
First, the doctor performs a physical examination of the patient to make a preliminary diagnosis. He needs to assess the location of the injury, determine whether there is pain, swelling, hyperthermia, deformation and hematoma. And if symptoms are diagnosed, their severity is assessed. The traumatologist must clarify the circumstances and time of injury, there were similar cases in the past, whether therapy was taken, and if so, what kind.
Functional tests are also required to determine the mobility of the joint. The inability to move in any direction will indicate damage, and its excessive mobility will indicate a complete rupture.
Basic diagnostic methods:
- X-ray examination is informative only in case of a complete rupture.
- MRI will help assess the condition of soft tissues.
- Arthroscopy – by inserting an endoscope, the condition of the injury can be assessed and treatment can be carried out immediately.
- Ultrasound is the most effective option for assessing the condition of the ligamentous apparatus.
To clarify the details of the course of the pathology, the doctor may prescribe: a general blood and urine test, biochemical analysis and rheumatic tests.
Treatment of ulnar collateral ligament injury
Treatment options will depend on the severity of the injury
. If the tissue is slightly damaged, it can heal itself.
Conservative treatment methods
will include: the use of NSAIDs (ibuprofen and aspirin), analgesics, exposure to the injury area with cold. It is imperative to limit serious loads on the elbow, apply a splint according to indications, and apply physiotherapeutic treatment methods.
Surgical intervention
In case of injury to the collateral ulnar ligament, it is usually necessary only for those patients who have been diagnosed with a complete rupture of the ligament and have severe pain, impaired limb function, or there is a threat of rupture.
Surgical reconstruction is recommended for patients with acute ligament rupture, as well as those for whom conservative treatment has not helped or who need to return to sports activities at any cost.
when the ligament is repaired using other tissues. This intervention is called “Tommy John surgery” (named after the athlete whose career was successfully saved by Dr. Frank Job).
Ligament reconstruction is performed using various soft tissue grafts, but the most common option is taking tissue from the forearm palmaris
, this is an almost ideal replacement for a damaged ligament.
Elbow injuries in athletes
As a result of repeated throws, a variety of injuries can develop. The problem is most often associated with the inside of the elbow joint, where the most significant loads are concentrated at the moment of throwing.
Flexor tendinitis
Repetitive throwing can cause irritation and inflammation of the flexor/pronator tendons, which attach to the humerus on the inside of the elbow joint. Athletes complain of pain along the inner surface of the elbow joint when throwing, and in the most severe cases the pain persists at rest.
Ulnar collateral ligament (UCL) injury
Most often, this ligament is damaged in throwing athletes. Injuries to the UCL can vary in severity from minimal damage and inflammation to complete rupture. An athlete with a UCL injury will complain of pain along the inner surface of the elbow joint and notice a decrease in throwing speed.
Valgus-extensor overload (VRO)
At the moment of throwing, the olecranon and humerus rotate relative to each other. Over time, this leads to valgus-extensor overload - a condition in which the protective cartilaginous cover of the olecranon process wears out and bone growths - osteophytes - form along the periphery of the articular surface. Athletes with VRP report pain and swelling in the area of maximum bone-to-bone contact.
Shown here are pathological bone growths on the posterior and inner surface of the olecranon in VRP.
Stress fracture of the olecranon
Stress fractures occur when muscles become fatigued and become unable to absorb the stress placed on them. This leads to increased stress on the joints and bones, which can gradually lead to a non-traumatic bone fracture - a stress fracture.
The most common type of stress fracture in throwing athletes is an olecranon fracture. Athletes complain of acute pain in the olecranon area, which intensifies with throwing or other intense physical activity, and sometimes persists at rest.
Ulnar nerve neuritis
When the elbow is in flexion, the ulnar nerve is pulled around the bony prominence of the articular end of the humerus where it resides. In throwing athletes, this overstretch of the nerve occurs constantly, as a result of which it can be displaced from its normal position, which is accompanied by a painful click. This leads to inflammation of the nerve, a condition called neuritis.
Athletes with ulnar nerve neuritis complain of pain that has the nature of electric jabs from the inner surface of the elbow joint and spreads along the ulnar nerve to the forearm. During the throw or immediately after it, the athlete may notice numbness, paresthesia or pain in the area of the ring and little fingers, which may persist during the rest period.
Ulnar nerve neuritis occurs not only in athletes. Similar sensations may occur when you wake up in the morning or hold your elbow in a flexed position for a long time.
Complications of treatment
Possible complications include the inability to return to sports. In addition, there may be a loss of the ability to throw the ball at full strength, pain during an active swing and a reduction in the range of motion, and stiffness in the elbow area.
Complications such as bleeding and infections may occur during surgery. Also, in some cases, it is impossible to restore the physiological stability of the damaged joint. Damage to the ulnar nerve and skin irritation after graft collection are also likely.
Treatment of ligamentosis Prevention of atherosclerosis
Clinical picture
Classic symptoms of a sprained elbow:
- pain from the moment of injury;
- swelling of varying degrees;
- redness of the skin over the damaged area;
- local hyperthermia;
- it is possible to increase the general temperature to 37.5 ° C;
- weakness, dizziness, loss of strength.
In severe cases of the disease and complete rupture of the ligament, loss of consciousness, painful shock and inability to move the affected limb are observed.
X-ray diagnosis of tumor lesions of bones
Radiography is the primary method for diagnosing tumor lesions of bone tissue. Therefore, at the first stage, it is important to assess the fact of invasive growth, the destruction of bones that has taken place, or to refute this and find reliable signs of a benign process.
The basis for such an assessment will be several important provisions:
- Boundaries of education:
- a. Clear contours with a sclerotic rim - usually a sign of benignity
- b. Clear contours are usually a sign of benignity
- c. Blurred contours - usually a sign of malignancy
- Periosteal reaction:
Periosteal Reaction, Rich S. Rana, Jim S. Wu, Ronald L. Eisenberg, AJR:193, October 2009
Solid thickening – benign periosteal reaction against the background of osteoma
Bone tumor — Systematic approach and Differential diagnosis, Henk Jan van der Woude and Robin Smithuis, Radiology department of the Onze Lieve Vrouwe Gasthuis, Amsterdam and the Rijnland hospital, Leiderdorp, the Netherland, 2010
Layered (onion-skin-type) periosteal reaction with intermittent contour – an aggressive reaction against the background of Ewing’s sarcoma
Bone tumor — Systematic approach and Differential diagnosis, Henk Jan van der Woude and Robin Smithuis, Radiology department of the Onze Lieve Vrouwe Gasthuis, Amsterdam and the Rijnland hospital, Leiderdorp, the Netherland, 2010
Osteochondroma of the humerus: presents as an exostosis (red arrow) with a cartilaginous cap (blue circle)
Bone tumors
Schematic representation of typical location and morphological characteristics of bone tumors
Bone tumor — Systematic approach and Differential diagnosis, Henk Jan van der Woude and Robin Smithuis, Radiology department of the Onze Lieve Vrouwe Gasthuis, Amsterdam and the Rijnland hospital, Leiderdorp, the Netherlands, www.radiologyassistant.nl 2010
Abbreviations
ABC - aneurysmal bone cyst, CMF - chondromyxoid fibroma, EG - eosinophilic granuloma, GCT - giant cell tumor, FD - fibrous dyspalsia, HPT - hyperparathyroidism with Brown's tumor, NOF - non-ossifying fibroma, SBC - simple bone cyst
Lipoma of the inner surface of the lower third of the shoulder, expansive growth: pushing aside muscle bundles, no invasion of surrounding tissues. Also, the structure of the formation is homogeneous and is represented only by adipose tissue
Metastasis of small cell lung cancer to the distal humerus: invasive growth with bone destruction, invasion of surrounding soft tissues and joint capsule, reactive swelling of adjacent soft tissues
Schwannoma of the radial nerve of the lower third of the shoulder, a “target” sign on MRI
Soft-Tissue Tumors and Tumorlike Lesions: A Systematic Imaging Approach, Jim S. Wu, MD Mary G. Hochman, MD Radiology: Volume 253: Number 2—November 2009
Aneurysmal bone cyst of the distal humerus, expansively spreading along the lateral sections, fluid levels in the cystic cavities (arrows)
Vascular malformations
It is very important to distinguish between the terms “hemangioma” and “vascular malformation”, since specialists not directly involved in the treatment of such pathologies often confuse the terms, which leads to incorrect tactics for examining and treating patients, wasting time and money.
In 1846, the German scientist Robin Virchow coined the term “hemangioma” to describe hypervascular lesions on the skin based on their macroscopic structure, thus describing vascular malformations, vascular tumors, and hyperplasias. Having analyzed the etymology of the term hemangioma, one can understand that the scientific approach from the time of the beginning of knowledge of anomalies in the development of the vascular system classified vascular malformations as tumors. This approach involved treating hemangiomas as tumor formations.
With the development of morphological and clinical diagnostic methods, Virchow's classification underwent constant changes. The approach to the interpretation of vascular malformations was fundamentally changed in 1982, when Mulliken and Glowacki proposed a classification separating the concepts of vascular malformation and hemangioma. Vascular malformation does not imply tumor or primary hyperplastic tissue growth, only abnormal vascular networks with various combinations of vessels. Hemangioma suggests the presence of a tumor or hyperplasia that primarily developed from the tissue of the vessel. (Mulliken JB, Glowacki J: Hemangiomas and vascular malformations in infants and children: A classification based on endothelial characteristics. Plast Reconstr Surg 69:412-422, 1982 2.; Mulliken JB, Glowacki J: Classification of pediatric vascular lesions. Plast Reconstr Surg 70:120-121, 1982).
In 1996, at the Rome Symposium of the International Society for the Study of Vascular Anomalies, the world scientific community officially replaced the term “hemangioma” with “vascular malformation”, adopting a new classification.
The currently publicly accepted ISSVA classification is:
ISSVA classification for vascular anomalies (Approved at the 20th ISSVA Workshop, Melbourne, April 2014) https://www.issva.org/.
Venous malformation of the soft tissues of the ulnar fossa: pathological network of venous vessels (yellow arrow), phleboliths in the lumen of pathological vessels (red arrow), a characteristic sign of venous malformation