Such a complex shoulder and its injuries
The 4 joints that make up the shoulder girdle are stressed all day long, and not only during training. This happens both when you hold down the computer mouse at work, and when in your free time you enthusiastically point your finger at the smartphone screen.
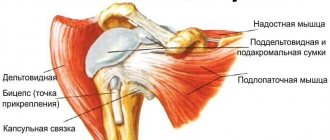
The shoulder girdle is an incredibly complex complex of soft tissues that comprises several joints that work together to produce smooth and powerful movements in coordination with the rest of the body.
Next, Dr. Raskin explains (and shows in the video below) how to self-assess your shoulder mobility and joint motion with a few simple tests. And this assessment can greatly influence your future training. All you need is your own body and a mirror.
Post-traumatic rehabilitation
Recovery from a shoulder injury is not a quick process. Rehabilitation, on average, can begin a month after injury. Again, this is an individual question and requires consultation with specialists in traumatology and sports medicine.
The simplest equipment is a rubber band. In principle, you don’t have to buy anything else besides it. The following set of exercises must be performed 3-5 times a week, each movement is performed for 15-20 repetitions, as slowly and under control as possible, clearly feeling the work of the muscles. In addition, you will need a place where you can attach the above-mentioned rubber band, so that you can change its position - at waist level, above and below it.
- Starting position – standing facing the place where the expander (or rubber band) is attached. The latter is secured below waist level. There is an espader in the injured hand, it is stretched, creating an initial tension in the muscles of the shoulder joint. Due to the combined movement of the shoulder and shoulder blade, we pull the rubber band towards the belt; we return to the starting position.
© natapetrovich — stock.adobe.com
- The exercise is similar to the previous one, but the expander should be at waist level, the starting position in this case is sitting. This way, the expander is approximately in line with the shoulder joint. Deadlifts are performed according to the same rules.
- The starting position is similar to that described in paragraph 2. The expander is fixed above the level of the shoulder joint. We also perform the expander pull towards ourselves.
- Rotator Cuff Stretch: You will need a dumbbell for this exercise. We bend the arm at the elbow, press the elbow joint to the edge of the iliac wing, and the shoulder is fixed in this position. The forearm is positioned at 09 degrees to the body. Smooth movements of the forearm are performed left and right, in a small amplitude, until a burning sensation is felt inside the joint.
© pololia — stock.adobe.com
Multiaxial shoulder movements
Testing internal and external functional rotation of the shoulder joint can play a huge role in not only identifying mobility deficits, but also in identifying painful areas in the shoulder girdle.
Functional internal and external rotation can be described as a combination of 3 shoulder movements that flow smoothly into each other in a specific sequence and rhythm within this range of motion.
Here are the components of each functional movement:
Functional internal rotation = internal rotation + extension + adduction
Functional external rotation = external rotation + flexion + abduction.
When surgery won't help
Any procedure has its own situations when it is powerless. It is not recommended to resort to this method of treatment and diagnosis if:
- fibrous or bone ankylosis;
- presence of an infected wound;
- purulent-inflammatory processes in the periarticular tissues;
- liver, kidney, cardiovascular failure;
- deforming osteoarthritis stage III-IV.
In some cases, at the discretion of the specialist, the operation can be performed:
- extensive damage (torn ligaments and joint capsules, loss of joint tightness);br>
- profuse hemorrhage into the joint cavity.
In cases of ankylosis and arthrosis of the shoulder joint, it is recommended to perform endoprosthetics (replacement of the affected articular surfaces with a prosthesis).
Shoulder Mobility Testing
The Apley's Scratch Test can show how both shoulder girdles work in coordination with each other and can also determine the capabilities of each shoulder joint individually.
Here the right arm moves, performing functional internal rotation, and the left one, at the same time, performing functional external rotation. The goal is to bring your fingers together enough that they touch behind your back. Then the hands change and you check the other side. During the test, you can slightly change the position of the spine (bend, for example) or gradually raise your lower arm up.
Pay attention to the distance between the palms during simultaneous functional internal and external rotation. Also note whether you experience pain and whether there is a difference between the range of motion on both sides.
What you feel is the most important aspect of this test, while hand coordination takes a back seat.
What kind of anesthesia
There are several types and tactics of anesthesia based on the characteristics of the injury to the shoulder joint.
- Conduction anesthesia using interscalene blockade. The injected anesthetic reaches the caudal portion of the cervical plexus (C3, C4), the upper and middle sections of the brachial plexus (C5, C6, C7); the drug reaches the lower trunk later and in much lower concentrations, so blockade of the median and ulnar nerves most often does not occur. This type of anesthesia is used for osteosynthesis of the clavicle, elimination of habitual shoulder dislocation (RHD), reduction of shoulder dislocation, and during operations on the upper third of the shoulder.
- Conduction anesthesia through supraclavicular access. The local anesthetic interacts well with all trunks of the brachial plexus, but in 80% of cases it does not reach the ulnar nerve. This anesthesia is indicated for operations on the upper limb and elbow joint. Used for osteosynthesis of the humerus.
- Endotracheal (inhalation) anesthesia. Such anesthesia immerses the patient in a state of deep medicated sleep, close to physiological.
- Combined anesthesia. The most common choice of surgeons. Endotracheal anesthesia is used together with conduction anesthesia. This allows you to potentiate the effectiveness of the methods and increase the analgesic effect after surgery.
Unilateral testing of functional internal and external rotation
If you find asymmetrical movements, pain, or noticeable mobility deficits (fingers not close to touching) during the Epley Scratch Test, it's time to try other tests to help find the source of the problem.
When you move with only one arm, the thoracic spine and rib cage do not provide additional mobility. During the Epley Scratch Test, both arms move toward each other and the thoracic spine is easily tested to see how well it can provide additional range of motion when movement in the shoulder girdle is no longer possible. Doing the movements with just one arm allows you to focus only on the shoulder.
Test each shoulder individually during functional internal and external rotation. During external rotation, you should reach with your fingers to the prominent ridge of the opposite scapula.
As for checking functional internal rotation: touching the inferior angle of the scapula on the opposite side with your fingers indicates normal mobility. The testing positions are the same as for assessing simultaneous functional internal and external rotations.
Features of the operation
The patient's journey before surgery begins with a consultation with an anesthesiologist who will offer possible anesthesia options. Most often, regional anesthesia is given to the arm or just the shoulder area. The substance (anesthesia) is injected into the base of the neck or along the sensory nerves related to the shoulder. In some cases, doctors use combined anesthesia with sedatives or mild general anesthetics, as the patient may experience discomfort during surgery. You will also need to undergo blood tests, ECG and fluorography.
It is important to tell your doctor about any medications and/or dietary supplements you are taking. You may need to stop taking some of them for a time before and after surgery.
The intervention is carried out in two positions: a reclining position and a position lying on one’s side. Each position allows for different operations, so the surgeon chooses the most appropriate approach for each patient.
During the surgical process, a fluid is first injected to increase the size of the joint. This allows you to get a higher quality and clearer image. Then punctures are made (from 1 to 3), into one of which an arthroscope is inserted. After the diagnosis is made, micro-instruments are introduced into other accesses to perform the operation. At the end of the operation, the surgeon applies sutures or adhesive strips to seamlessly close the edges of the wounds, securing them with a soft bandage.
The operation usually does not take more than an hour.
Scapulohumeral rhythm testing
Now that we have some understanding of the movements performed by the shoulders during functional internal rotation with one and two arms, it is time to evaluate rhythm and coordination.
In order for the shoulder to travel its full path without compensatory movements, the scapula and humerus must move synergistically and rhythmically. In sports medicine this is called the scapulohumeral rhythm.
Proper scapulohumeral rhythm means that for every 2 degrees of elevation movement of the humerus, the scapula should rotate upward 1 degree until the limit of motion is reached. However, the numbers won't tell you anything. The point at which the blade stops rotating is more important.
At approximately 120 degrees of arm elevation, the shoulder blade begins to rotate upward. If your shoulder blades become clearly visible on the sides of your body before reaching 120 degrees when you slowly raise your arms, this indicates that the posterior tissues of the shoulder are toned and tense.
In addition, the symmetry of movements on both sides should be assessed. Do your shoulder blades begin to rotate simultaneously or is their rhythm asymmetrical?
If the rhythm is disrupted, your best bet is to start working on soft tissue mobility in the back of the shoulder girdle.
This can be simple movements focusing primarily on the latissimus dorsi and other surrounding muscles using a foam roller or through self-myofascial release techniques. You can also use movements aimed at developing mobility, for example, adding stretching to your training program.
The choice is yours, and the only wrong decision is to do nothing at all.
Indications for arthroscopy
Surgeons suggest using this intervention in the following situations:
- For initial diagnosis of pathology or clarification of the diagnosis;
- Severe pain in the shoulder area after surgery. In this case, arthroscopy is aimed at diagnosis and, if necessary, removal of trigger elements;
- Unstable shoulder joint (Bankart injury, shoulder dislocation, including primary)
A) In case of anterior dislocation of the joint, the intervention is aimed at restoring the articular labrum (Bankart operation). The method is aimed at restoring the integrity of the articular lip by fixing the torn part to the edge of the articular process of the scapula.
B) In case of habitual posterior dislocation, the articular labrum is restored together with suturing of the joint capsule from behind. A study by GW Misamore et WA Facibene showed that after arthroscopy, 13 out of 14 athletes operated on with this method were able to achieve their previous physical condition and results.
C) In the case of a combination of posterior Bankart injury, accompanied by a posterior rupture of the scapular glenoid ligament, arthroscopy allows fixing the torn articular labrum to the edge of the glenoid cavity of the scapula, the posterior part of the shoulder capsule to the posterior part of the humeral head. Bioabsorbable anchor fixatives are used as a fixative.
- Epicondylitis . Used when conservative treatment is ineffective. The operation consists of separating the muscles from the area of attachment to the condyle of the humerus, then removing chronically inflamed and altered tissue. The muscles are then reattached to the bone.
- SLAP syndrome (snapping shoulder syndrome). It is characterized by avulsion of the upper components of the articular labrum of the joint joint associated with the tendon of the long head of the biceps. In the initial stage, arthroscopic debridement of the affected area is recommended. This method makes it possible to remove from the intra-articular space pieces of destroyed cartilage tissue, overgrown fragments of the synovial membrane, and bone protrusions (osteophytes that interfere with the sliding of the articular head and cause additional mechanical damage to the cartilage).
- Capsulitis (“pseudo-frozen shoulder”). The operation is performed only if all conservative methods are ineffective and is aimed at removing the inflamed areas of the joint capsule.
- Rotator cuff injury. During the operation, the torn part of the tendon is stretched to the place of its attachment and then sutured. For this purpose, special materials are used - “anchor clamps”. All necrotic, DDI tissues of the rotator cuff are subject to mandatory removal. Afterwards, the damaged area where damaged cuffs were diagnosed is removed from residual tissue fragments (including soft ones) so that the tendon can be firmly fixed with the help of scar tissue.
- chondromatous bodies in the synovial fluid .
- Overgrowth of bone tissue;
- Osteosynthesis of fractures of the processes of the scapula.
- Bursitis , including removal of the joint capsule of the shoulder joint. In this operation, the surgeon completely removes the inflamed joint capsule.