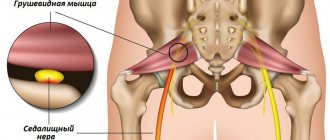
Inflammations of the soft tissues of the leg can occur in various forms and be localized in a variety of places. The clinical picture, however, has general manifestations. The course of treatment must be prescribed by a doctor, one of the stages is shock wave therapy.
With a small depth of the process, painful swelling develops with redness and increased skin temperature. If the inflammation goes deeper, the patient experiences attacks of fever, and signs of intoxication appear. This indicates the beginning of the purulent-necrotic stage.
If you suspect inflammation of the soft tissues of the leg, you should immediately consult a doctor, since a rapidly developing inflammatory process may ultimately lead to the need for amputation.
Types of leg inflammation
It is very easy to get inflammation even in everyday life. Broken knees, abrasions, scratches are typical causes of the development of various inflammations of the leg. Penetration of microbes into the soft tissues of the legs can also occur:
- with skin scratching - for example, with an allergy to insect bites;
- for fungal diseases accompanied by cracks in the skin;
- for diabetic ulcers;
- with varicose veins;
- when injecting in unsanitary conditions - for example, in cases of drug addiction;
- for injuries and wounds - for example, in athletes or military personnel;
- when microflora is introduced from primary inflammatory foci with blood or lymph.
The causative agents of purulent inflammation of soft tissues are pyogenic bacteria, mainly staphylococcal bacteria. At the initial stage, blood microcirculation is disrupted, which is associated with damage to the tissue structure. If you do not immediately begin to treat inflammation of the soft tissues of the leg, swelling begins, which already causes pain when the muscle tissue is bursting with accumulated fluid, and they signal this through the neuromuscular junction. In the vast majority of situations, the patient takes pain medication and forgets about the problem. Meanwhile, the inflammation enters the purulent stage, when the neuromuscular connection is lost, there is no more pain, but pus accumulates. There are two known variants of purulent inflammation:
- Abscess. In common parlance - an abscess. It develops in the muscles and subcutaneous tissue, has clearly defined boundaries within the purulent capsule, which is formed as a protective reaction of the body to infection.
- Phlegmon. Acute diffuse inflammation of the subcutaneous tissue, has no clear boundaries, easily spreads to the entire limb.
Anaerobic infections also pose a great danger to the feet. The most common inflammations of the soft tissues of the leg associated with this type of infection are:
- Erysipelas. Manifests itself in the form of blisters on the skin, redness, and hemorrhages. The causative agent is streptococcus; inflammation can develop upon contact with a person affected by a streptococcal infection, for example, a sore throat. In rare cases, this type of inflammation goes away on its own, but you shouldn’t count on it. Advanced cases of erysipelas will have to be treated for several months.
- Gangrene is tissue death. The causative agent is bacteria of the Clostridia family, “living” in soil and dust. Gangrene can only be treated by amputation, so in case of injuries it is very important to disinfect the wounds and immediately consult a doctor.
Causes of paraproctitis
In most cases, inflammation is caused by opportunistic bacteria and fungi that are normally present in the human intestine; however, if they manage to overcome the mucous membrane and enter the tissue surrounding the rectum, in the absence of oxygen they begin to rapidly multiply and cause an acute inflammatory process. As a rule, paraproctitis is caused immediately by a complex of pathogens, which may include streptococci, staphylococci, and E. coli.
The trigger for the development of paraproctitis can be any damage to the rectal mucosa. Therefore, risk factors for paraproctitis include:
- anal fissures;
- proctitis (inflammation of the rectal mucosa);
- constipation (dense stool can injure the mucous membrane);
- diarrhea (prolonged stool disorder leads to damage to the mucous membrane);
- hemorrhoids (bursted hemorrhoids form open wounds).
Often the infection enters through the anal glands. These glands are designed to secrete enzymes that help digest food and mucus that facilitates the passage of feces. The anal glands enter the rectum in crypts - tissue pockets open to the movement of feces. If the process of emptying the rectum is disrupted or if the crypt is injured (even minor), the crypt may become blocked. As a result, an inflammatory process develops in the gland, and the infection enters the cellular spaces through its duct.
Sometimes the infection can enter the peri-rectal tissues through the bloodstream. In this case, the source of infection may be inflammatory processes in other organs.
Treatment methods for leg inflammation
Inflammatory processes are treated in several stages. If the disease has progressed to a purulent stage, surgical removal of the pus and treatment of the wound are necessary. Further, and in milder stages, anti-inflammatory drug therapy is prescribed - a course of antibiotics in the form of tablets or injections, depending on the origin and severity of the infection. It is very important to choose the right drugs; for this, bacterial culture is done. The patient is prescribed to drink plenty of fluids to quickly remove toxins from the body.
At the recovery stage, physiotherapy is prescribed, aimed at regenerating the circulatory system and lymph flow. This can be successfully dealt with by a course of shock wave therapy, which promotes rapid restoration of soft tissues. You can take it at our Medcenter-Plus clinic.
Symptoms of paraproctitis
The onset of the inflammatory process can be marked by a slight increase in temperature (up to 37°C). When inflammation moves into the cellular space, i.e. In the development of acute paraproctitis itself, a complex of symptoms simultaneously appears. First of all, this is:
- temperature rise to 38°C (or higher);
- chills;
- pain in the rectal area not associated with bowel movements.
Subcutaneous paraproctitis has its own pronounced symptoms: the area of inflammation located next to the anus is distinguished by redness, swelling and thickening of the tissue. When palpated, a sharp pain is experienced.
With other types of paraproctitis, urination disorder, stool retention, and false urge to defecate may be observed.
Inflammation leads to the melting of cellular tissue and the accumulation of pus. In the absence of timely treatment, the resulting abscess breaks through and a fistula opening is formed - either outward (in the perineum, on the anterior abdominal wall or thigh), or into the intestinal lumen. In women, the abscess can open, forming a fistula in the vagina. The most dangerous option is the opening of a fistula into the abdominal cavity.
After the formation of a fistula, the bulk of the pus comes out, and the severity of the symptoms decreases. However, purulent processes continue, the disease becomes chronic.
Symptoms of chronic paraproctitis
With chronic paraproctitis, pain and discomfort are felt only if the exit of pus through the fistula is difficult for any reason. Usually pain is observed only with an internal fistula. The pain intensifies during bowel movements, and then subsides, since stretching of the intestines during the passage of stool promotes the release of pus. Pus or ichor is constantly secreted. With a rectal fistula, which has an external opening in the perineal area, the discharge irritates the skin, causing itching.
Chronic paraproctitis is characterized by a wave-like course of the disease. From time to time, the fistula canal becomes blocked by granulations and becomes clogged with dead tissue, as a result, pus again begins to accumulate in the area of inflammation and the symptoms of acute paraproctitis return. Then the abscess breaks out again and the severity of the symptoms disappears.
Types and forms of necrosis
There are 2 main forms of pathology:
- Dry necrosis. In medicine it is also called coagulation. With it, the protein coagulates, which soon becomes like a curd mass. The skin in problem areas will turn yellow-gray. With this form, ulcers appear in the place where dead tissue is rejected, which quickly turn into ulcers. After opening them, a fistula is formed. At the initial stages of the development of the disease, the following symptoms may be noted: increased body temperature, problems with the functioning of the problem organ.
- Wet necrosis. The medical term is liquefaction necrosis. It manifests itself as an active increase in soft tissues. In areas of dead tissue, they liquefy and a putrefactive environment is formed for the spread of harmful microorganisms. In addition, a rotten smell appears, with which nothing can be done, even if treatment is carried out. This form of the disease most often affects the skin, brain and other organs in which a lot of fluid accumulates. With the active development of the disease, complications may appear. If necrosis affects the brain, it is possible that the patient may lose memory.
In addition to forms, there are several types:
- bedsores - appear in patients with a bedridden lifestyle who are not provided with proper care;
- gangrene - appears after actively developing necrosis. Accompanied by necrosis of the skin, mucous membranes, muscle tissue;
- heart attack - detected when blood suddenly stops flowing to a certain organ;
- aseptic – appears when the head of the femur is injured. Its symptoms are unbearable pain in the affected area and the inability to move independently. Appear 2-3 days after the onset of the disease;
- fibrinoid - detected in the walls of blood vessels.
Introduction
Soft tissue sarcomas account for 15% of all malignant neoplasms in children and only 1-2.5% in adults. They occur with equal frequency in people of both sexes, predominantly affecting people aged 20 to 40 years. In 50% of patients, tumors are localized in the extremities, in 40% - on the trunk, and in 10% - in the head and neck [1, 2, 10].
In Russia in 2008, the incidence of soft tissue sarcomas was 1.2 per 100,000 population per year [3].
According to the international morphological classification of soft tissue sarcomas, there are more than 40 histological forms of malignant soft tissue tumors [3]. Developing from different germ layers, the group of soft tissue sarcomas appears to be extremely heterogeneous in clinical course, prognosis, treatment approaches and response. According to the authors, 42% are tumors of mesenchymal histogenesis, 32% are tumors of ectodermal histogenesis, 22% are tumors of mesodermal histogenesis, 4% are tumors of endodermal and unclear histogenesis. According to the frequency of morphological forms, malignant tumors of soft tissues are distributed as follows: malignant fibrous histiocytomas, liposarcomas, leiomyosarcomas, unclassified sarcomas, synovial sarcomas, rhabdomyosarcomas and malignant tumors of peripheral nerve sheaths, fibrosarcomas, angiosarcomas [3, 4, 8, 12].
Soft tissue sarcomas at the present stage of development of oncology represent a poorly studied group of human malignant neoplasms. Despite the fact that these tumors often have an “external” localization, a significant number of errors are made in their diagnosis and treatment [3, 6, 7].
Early diagnosis of soft tissue sarcomas is one of a number of rather complex issues in oncological practice. There are objective factors contributing to this. Appearing in the form of a painless, round or oval-shaped node in the thickness of the muscles, especially in the proximal limbs, malignant neoplasms of soft tissues in the early stages do not manifest themselves clinically. The absence of pain and dysfunction of the affected segment leads to the fact that the patient does not attach importance to the self-identified tumor, regarding it as a benign or inflammatory process, often resorting to self-medication. The reasons for seeking medical help are the large size of the tumor, deformation of the contours or dysfunction of a nearby joint, pain syndrome that develops when the tumor compresses the nerve trunks. When the distal parts of the extremities are affected, where physiologically the volume of soft tissue is small, the tumor appears even at small sizes. Pain is often associated. In these situations, the patient seeks medical help early.
The rarity of the disease, the lack of oncological alertness on the part of both the patient and doctors, the small size of the formation, painlessness and apparent benignity of the process lead to the fact that in 90% of cases diagnoses such as cyst, lipoma, myositis ossificans, hematoma, fibromatosis, abscess are made , traumatic injuries of soft tissues, osteochondrosis, etc. In this case, the diagnosis is based only on anamnestic data and local status, and instrumental examination methods are not used. Sometimes a standard X-ray of the tumor area is performed, which is usually uninformative. This leads to the fact that only a few patients are referred for consultation to an oncologist.
An incorrect diagnosis leads to incorrect treatment: physiotherapy, massage, anti-inflammatory therapy. An “abscess” or “hematoma” is opened, often without morphological examination. All of these manipulations stimulate tumor growth and delay the timing of special therapy.
The clinical course of soft tissue sarcomas is characterized by early hematogenous (up to 60%) and to a lesser extent lymphogenous (5-15%) dissemination, a high frequency of locoregional relapses (10-30%), multicentric tumor growth (15-25%). All this determines the unfavorable development and course of the disease. Treatment can be adequately planned only after a thorough examination of the patient, determining the full clinical picture and the extent of the tumor process. Therefore, in all observations, in addition to the use of local research methods (ultrasound, CT, MRI of the affected area), it is necessary to conduct radiography (preferably CT) of the chest organs, ultrasound of the abdominal organs and regional lymph nodes, and osteoscintigraphy [1, 8, 9].
Material for morphological diagnosis is obtained by puncture biopsy (aspiration or trepanobiopsy), as well as by making impression smears from the ulcerated surface of the tumor. The accuracy of cytological diagnosis for soft tissue sarcomas reaches 83-85% [7]. However, given the heterogeneity of the tumor structure, the presence of zones with varying degrees of differentiation and the wide variety of morphological types of tumor, open biopsy is preferable. It allows you to obtain a sufficient amount of material for research, more accurately establish the histological identity of the neoplasm, determine the degree of its differentiation and adequately plan further treatment tactics for the patient. The choice of access for open biopsy should correspond to further plans for the management of a particular patient and be performed by an oncologist, since the biopsy area should be located at the site of subsequent surgery and removed en bloc with the tumor.
Tactics, scope of treatment and prognosis of the disease for soft tissue sarcomas are determined by the stage of the process, degree of tumor differentiation, histological form, location, age of the patient, and the presence of concomitant diseases. Thus, the use of only the surgical method is considered adequate for highly differentiated tumors. In patients with moderately and poorly differentiated sarcomas, a combined approach should be used (surgical, drug and radiation treatment methods and their combinations). This makes it possible to reliably reduce the frequency of local relapses and tumor metastasis and thereby increase the percentage of favorable outcomes. Taking into account the above, the tactics of patient management should be discussed in each specific observation at a consultation with the participation of oncological surgeons, chemotherapists and radiologists [5, 10].
Material and methods
In the Department of Oncological Orthopedics, Moscow Research Institute of Orthopedics. P.A. Herzen from 1995 to 2010 treated 120 patients with primary or recurrent soft tissue sarcomas. Analysis of this clinical material allowed us to identify the most common errors in diagnosis and treatment, which were made in 52 (43%) patients.
Results and discussion
Errors at the stage of active identification of patients.
Most of these errors occurred at the stage of patients applying to institutions of the general medical network. This may be due to a number of objective reasons. The relative rarity of the disease determines the lack of sufficient experience in diagnosing soft tissue sarcomas by outpatient healthcare providers. Most patients with soft tissue sarcomas first turn to traumatologists, surgeons, therapists, pediatricians, neurologists and doctors of other specialties, who prescribe the treatment options listed above. It takes a long time before the patient is referred to an oncologist. We present a clinical observation.
Patient B.,
21 years old, entered the department of oncological orthopedics of the Moscow Oncology Institute named after. P.A. Herzen in October 2007. In March 2007, she noted the appearance of pain in the right iliac region, radiating to the right half of the groin area and the right thigh, but did not consult a doctor. Subsequently, the pain syndrome intensified; in addition, the patient noticed a decrease in the volume of tissue in the right thigh (muscle atrophy), weakness in the right lower limb. She contacted doctors at her place of residence in May 2007. Based on X-ray examination of the lumbar spine, a diagnosis was made: osteochondrosis with severe radicular neurological symptoms. She was sent to a city hospital, where conservative treatment (massage, anti-inflammatory, analgesic therapy) was carried out without effect. She was subsequently referred for treatment to the All-Russian Myasthenic Center, where, for isolated myasthenia of the right thigh muscles, she was treated with glucocorticosteroids and electrical muscle stimulation without effect. Due to deterioration of the condition and a sharp increase in pain, progression of the right lower monoparesis, a computed tomographic examination of the lumbar spine and abdominal cavity was performed in September 2007; a soft tissue tumor of the right iliac region was suspected. The patient was sent to the Moscow Scientific Research Institute, where, during examination, according to ultrasound of the abdominal cavity and magnetic resonance imaging, it was determined that the entire right iliac region was occupied by a volumetric formation measuring 10.5×9.8 cm, 12.6 cm in length, heterogeneous in structure, with lumpy contours. The upper border of the tumor is at the L3 level, the tumor spreads to the perinephric tissue and prolapses into the pelvic cavity. An open biopsy of the tumor was performed. Morphological conclusion: malignant paraganglioma. After establishing the diagnosis and determining the extent of the process, special treatment was started.
Diagnostic errors.
Objective reasons for diagnostic errors include difficulties in correctly recognizing the process, due to the fact that in the early stages the clinical symptoms are similar to the manifestations of other diseases of the musculoskeletal system (as in the previous example).
Underestimating the patient's complaints and interpreting the symptoms of the disease as not related to the tumor are the most common mistakes. The doctor is disoriented by the patient’s desire to associate the disease with trauma or another previously suffered illness. For these reasons, in most cases, clinical signs, which are interpreted as inflammatory or post-traumatic changes, are underestimated. Thus, based on anamnestic data and analysis of medical documentation, it was established that the most common referral diagnoses from medical institutions of the general medical network to specialized (oncological) dispensaries and hospitals were soft tissue abscess (45%), post-traumatic hematoma (35%), myositis (12 %).
Diagnostic errors include inadequate performance of an oncological search aimed at identifying distant metastases, since tumor dissemination is one of the most unfavorable prognostic factors and radically changes the patient’s treatment tactics. So, according to data from the Moscow Research Institute of Orthopedics. P.A. Herzen, approximately 30% of patients had insufficient examination and underestimation of the stage of the initial tumor process. This is clearly illustrated by the following clinical example.
Patient V.,
25 years old, entered the department of oncological orthopedics of the Moscow Research Institute of Orthopedics named after. P.A. Herzen in June 2006. In May, she noted the appearance of a rapidly growing mass formation in the upper third of the right thigh. I went to the clinic at my place of residence. After an aspiration biopsy, a malignant soft tissue neoplasm was diagnosed. Without performing additional research methods (ultrasound, CT, MRI, chest x-ray, histological verification), surgical treatment was recommended, from which the patient abstained and independently contacted the Moscow Research Institute of Oral Orthopedics. P.A. Herzen. In the clinic, after an open biopsy, a histological diagnosis was made: low-grade rhabdomyosarcoma. A full diagnostic examination, in addition to the local process, revealed multiple metastases in the lungs. In this regard, the patient in the conditions of the Moscow Research Institute named after. P.A. Herzen underwent complex treatment: pre- and postoperative multi-course polychemotherapy with a confirmed clinical and morphological effect, surgical removal of a tumor of the right lower limb and postoperative radiation therapy with a total focal dose of 60 Gy. Next, thoracoscopic atypical resection of the right lung was performed for remaining metastases. Treatment was completed in September 2008. The patient is currently under dynamic observation. There is no evidence of relapse or progression of the disease.
The stage of the process determines the treatment strategy and must be established before the start of special therapy. Without identifying the morphological identity and degree of malignancy of the tumor, staging is impossible. Determining the histological type of soft tissue sarcoma is one of the most difficult areas of modern oncology. Immunohistochemical and morphogenetic studies help in solving these problems, but most oncology clinics and hospitals do not conduct these studies or do not have such an opportunity, and the rarity of the disease and the variety of forms do not allow the morphologist to have sufficient experience in the correct interpretation of the study results. So, according to the Department of Pathomorphology of the Moscow Research Institute named after. P.A. Herzen, in 30% of patients with soft tissue sarcomas, when reviewing histological preparations, the diagnosis and stage change, and in most reports from other institutions the degree of malignancy of the tumor is not indicated, which explains the inadequate approach to treatment. This is confirmed by the following clinical example.
Patient K.,
37 years old, entered the department of oncological orthopedics of the Moscow Oncology Institute named after. P.A. Herzen in February 2009. In November 2008, he noted the appearance of a tumor formation in the scapular region. I went to the oncology clinic at my place of residence. According to a comprehensive examination (ultrasound, CT), a neoplasm was identified, located deep in the muscles of the scapular region, measuring 8x7x6 cm. After an open biopsy, liposarcoma was diagnosed without specifying the histological type and degree of differentiation of the tumor. In December 2008, a soft tissue tumor was removed. Morphological examination of the surgical material confirmed the diagnosis of myxoid liposarcoma. 3 weeks after surgery, the patient noted the appearance of a node in the area of the postoperative scar. In January 2009, repeated removal of the formation was performed with excision of the postoperative scar. Morphological examination: myxoid liposarcoma. At the beginning of February 2009, due to the continued growth of the tumor, he independently turned to the Moscow Oncology Research Institute named after. P.A. Herzen. Based on examination data (ultrasound, CT, MRI), aspiration biopsy of the tumor and revision of the morphological blocks of previous operations, continued growth of high-grade liposarcoma (G3) was diagnosed. Taking into account the medical history, clinical picture and degree of tumor differentiation, the patient was started on special treatment. After 3 courses of polychemotherapy, regression of the tumor node by 30% was noted. In May 2009, the tumor was removed with a session of intraoperative radiation therapy ROD 15 Gy. Morphological study of the surgical material: G3 liposarcoma with symptoms of therapeutic pathomorphosis of the III degree. At a consultation with the participation of a radiologist, a chemotherapist and an oncological surgeon, taking into account the clinical course of the disease, as well as the combined treatment carried out according to the radical program, it was recommended to leave the patient under dynamic observation. Currently, there is no data indicating relapse and progression of the disease.
Thus, if patients have soft tissue sarcomas, a detailed diagnostic examination is necessary. This allows you to determine the stage of the process and the extent of the disease, plan tactics and the volume of upcoming therapy.
Treatment and tactical errors.
Analysis of treatment and tactical errors shows a direct relationship between incorrect or incomplete diagnosis, underestimation of objective examination data or their complete absence. Also affecting is the lack of knowledge of the main features of the course of the tumor process, modern approaches and the sequence of application of special methods (taking into account the biological properties of soft tissue sarcomas) in the treatment of this category of patients.
So, according to data from the Moscow Research Institute of Orthopedics. P.A. Herzen, 60% of patients are admitted for treatment to a specialized institution with continued tumor growth after inadequate treatment carried out at the place of residence. This is largely due to the fact that doctors, when removing the primary tumor, do not take into account the clinical and morphological features of soft tissue sarcomas, which include: the absence of a true capsule, a tendency to infiltrative growth, multicentricity of tumor primordia, and disruption of intercellular connections. And performing surgical intervention in the amount of extracapsular removal (“husking”) of the tumor without observing the basic principles of oncology (ablasticity, sheathing, blockiness and zonality) further increases the percentage of both local relapse and dissemination of the process and, as a result, worsens the prognosis diseases. At the same time, the intervals between relapses decrease, and the tumor acquires features of greater atypia and an aggressive course [4, 9, 11, 12]. This is well illustrated by the following observation.
Patient I.,
52 years old, in 2007, due to a tumor of the soft tissues of the left elbow area, it was excised at the local clinical hospital under local anesthesia at the place of residence. Morphological conclusion: fibrosarcoma G1. In 2008, due to a relapse, surgical treatment was repeated at the place of residence. 3 months after surgery, continued growth was diagnosed. The patient was sent to the Moscow Scientific Research Institute named after. P.A. Herzen. Review of morphological preparations confirmed the presence of fibrosarcoma. When comparing the presented surgical material, an increase in the number of mitoses and cellular polymorphism of the tumor was noted after surgical treatment for tumor recurrence. In both cases, the tumors were removed within their capsule (“non-radically”). An examination in the clinic confirmed the continued growth of fibrosarcoma in the area of the postoperative scar, in addition, 12 tumor formations were identified in the soft tissues of the lower and middle third of the shoulder and forearm, up to 15 mm in size.
Adequate surgical removal of soft tissue sarcomas requires adherence to the principles listed above. After tumor removal, extensive defects may arise that require reconstructive plastic surgery, which is performed only by oncologist surgeons who are constantly dealing with this problem [3].
Patient M.,
30 years old, entered the department of oncological orthopedics of the Moscow Oncology Institute named after. P.A. Herzen in February 2009. In November 2008, she noted the appearance of a formation in the right popliteal fossa. I went to the clinic at my place of residence. With a diagnosis of a soft tissue tumor in the popliteal region, the patient was sent to the regional oncology clinic. In January 2009, the tumor was removed (with a described tumor diameter of 5 cm, the postoperative scar had a length of 7 cm and was transverse). Morphological examination: moderately differentiated sarcoma. The doctors decided: “taking into account the histological conclusion and the radical extent of the surgical intervention, to leave the patient under dynamic observation.” In March 2009, the patient noted repeated growth of the tumor in the area of the postoperative scar. I contacted the Moscow Scientific Research Institute named after. P.A. Herzen. A puncture biopsy was performed and blocks of morphological preparations of the surgical material were reviewed. Continued growth of poorly differentiated synovial sarcoma was diagnosed, and single metastases were identified in the right lung. Combination treatment was started in the clinic. During 8 courses of chemotherapy according to the VAC regimen, positive increasing dynamics were noted during the entire period of drug treatment in the form of regression of the recurrent tumor node by 50%, as well as a stable clinical picture of metastases in the lungs. At a consultation with the participation of a chemotherapist, radiologist and oncologist surgeon, a decision was made to perform simultaneous surgical removal of all tumor foci. In September 2009, a tumor of the right popliteal region was removed with plastic surgery of the soft tissue defect with a displaced medial portion of the gastrocnemius muscle and thoracoscopic atypical resection of the lower and middle lobes of the right lung. Morphological study of surgical material: synovial sarcoma G3 with symptoms of therapeutic pathomorphosis of the III degree. In the lung tissues there are metastases of a malignant tumor of an identical structure with mild symptoms of stage I-II pathomorphosis. The patient was re-discussed at the consultation, taking into account the clinical course of the disease, as well as the treatment provided, it was recommended to continue chemotherapy in the amount of 6 courses with correction of the regimen (IE - etoposide, ifosfamide). Currently, there is no data on relapse and progression of the disease.
Several diagnostic and tactical errors were made in this clinical observation. Inadequate removal of the primary tumor (discrepancy between the size and location of the postoperative scar and the volume of the formation) and the undiagnosed histological type of sarcoma, as well as the incorrectly determined degree of malignancy of the tumor, were the cause of a number of consecutive errors in the treatment of the patient.
As you can see, ignoring modern approaches in the diagnosis and treatment of patients with soft tissue sarcomas inevitably leads to the choice of inadequate treatment tactics, worsening the prognosis of the underlying disease, complicating and increasing the cost of treatment.
Another gross tactical mistake is performing surgery on any soft tissue neoplasm without subsequent planned morphological examination of the removed material.
Treatment and methodological errors.
Most methodological errors in soft tissue sarcomas involve non-compliance with the start dates and treatment intervals. Thus, on average, the duration of the period between the end of preoperative therapy (chemotherapy, radiation treatment) and surgery should not exceed 14-28 days; lengthening this period to 5 weeks or more leads to resumption of tumor growth and an increase in its malignant potential.
Errors also occur in the dosages of medications used in the treatment of soft tissue sarcomas. As a rule, a deliberate underestimation of the recommended doses of chemotherapy in order to reduce the possible risk of complications and adverse gastrointestinal manifestations (nausea, vomiting, diarrhea) leads to a lack of effect from treatment and the development of tumor resistance (insensitivity) to chemotherapy. According to the Moscow Scientific Research Institute of Oriental Studies. P.A. Herzen, in 15% of patients with soft tissue sarcomas who applied for disease progression, the dose of drugs was underestimated by 30%, and in a number of patients - by 60%. Failure to observe intervals between courses of chemotherapy, inadequate doses of chemotherapy, and continuation of treatment according to previous regimens with negative dynamics are the reasons for further progression of the tumor process, worsening the already unfavorable prognosis of the disease. We present a clinical observation.
Patient K.,
36 years old, entered the department of oncological orthopedics of the Moscow Oncology Institute named after. P.A. Herzen in March 2008. In August 2007, synovial sarcoma G3 of the soft tissues of the left thigh was diagnosed at the place of residence. The patient was sent to the regional oncology clinic. The examination confirmed the presence of a malignant tumor measuring 50×74×24 mm in the soft tissues of the left lower limb. Computed tomography revealed multiple metastatic lesions of the lung tissue, the diameter of the metastases was from 3 to 7 mm. Special treatment has been started. From October 2007 to February 2008, 4 courses of polychemotherapy were carried out according to the VAC regimen. At the same time, the intervals between courses varied for no reason from 24 to 38 days, and the total course doses of administered drugs, taking into account height and weight indicators (S = 1.8 m2), according to official medical documentation (discharge summary from the medical history), were as follows: doxorubicin 50 mg, vincristine 2 mg, cyclophosphamide 1000 mg. During chemotherapy, negative dynamics were noted in the form of further tumor growth. The patient was sent to the Moscow Scientific Research Institute named after. P.A. Herzen. During an examination at the institute’s clinic, according to ultrasound, MRI and CT data, several tumor nodes merging with each other, with a total size of 105×90×38 mm, were identified in the soft tissues of the patient’s left shoulder along the posterolateral surface. In the lungs, the diameter of identified metastatic foci increased to 15-22 mm.
It should be noted that the main active special chemotherapeutic agents in the treatment of soft tissue sarcomas, even when prescribed in monotherapy, are anthracycline drugs, which give a reliably pronounced effect at the maximum permissible therapeutic doses. According to our calculations, the minimum total course dose of doxorubicin in the VAC regimen for this patient should have been at least 90 mg. In this situation, at the first stage, for the purpose of cytoreduction, it was more expedient to start treatment with surgery, supplementing it with intraoperative radiation therapy to achieve local control. 10-14 days after surgery, start systemic chemotherapy.
Another common mistake is ending treatment after tumor removal. The absence of a tumor node and the possible achievement of local control do not exclude the presence of micrometastases and locoregional primordia. Even if all principles of adequate tumor removal are observed, the rate of local recurrence reaches 10-20% [9, 12]. In a number of observations, this dictates the need for postoperative therapy. When planning this treatment, the first place comes to a planned morphological study of the removed material, which should answer a number of fundamental questions: determining the true degree of malignancy of the tumor (index G), the state of the resection margin after surgical treatment (index R) and assessing the degree of therapeutic pathomorphosis. Based on the analysis of these data, tactics and methodological aspects of the necessary additional therapy (chemotherapy, radiation therapy, repeated surgery) are collectively developed.
Thus, the apparent simplicity and accessibility for surgical treatment (especially of small tumor formations) without a preliminary, thorough examination, accurate diagnosis and staging of the process, ignorance of the principles of oncological surgery for soft tissue sarcomas, violation of the sequence and phasing of treatment lead to progression of the disease and worsening prognosis. The high frequency of errors associated with the rarity of the disease, lack of experience, difficulty in diagnosis, development of adequate treatment tactics and acceptable not only in the medical network, but also in regional oncology institutions, dictates the need to concentrate these patients in institutions that purposefully, rather than occasionally, provide treatment patients with soft tissue sarcomas.
In the Russian Federation, the East European Group for the Study of Sarcomas of Bones and Soft Tissues has been created. The analytical, clinical and advisory work carried out should determine priority options in solving existing problems of practical oncology.