Congenital dysplasia of the hip joint is diagnosed in three newborns out of a thousand children examined. Pathology is indicated by limited hip abduction and asymmetrical position of the femoral and gluteal folds. Treatment of dysplasia in newborns is predominantly conservative using orthopedic devices, physiotherapeutic and massage procedures.
What is hip dysplasia
Hip dysplasia (HJ) is a congenital pathology that causes frequent dislocations or subluxations. At birth, the baby's hip joint is not yet fully formed. The acetabulum is flattened, located almost vertically, and the head of the femur is supported only by the elastic round ligament, acetabular labrum and articular capsule.
At a certain stage of embryogenesis, a malfunction occurs - the development of ligaments, cartilage and bone structures or muscle tissue is disrupted. The femoral head is no longer held in the acetabulum, but periodically shifts or completely slips out of it. Dysplasias differ in the degree of underdevelopment of the hip joint. In newborns, both gross disorders and increased mobility are diagnosed against the background of a weak ligamentous apparatus.
Classification
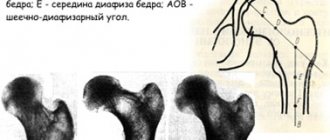
The classification of dysplasia is based on a violation of the development of a certain part of the hip joint. With acetabular pathology, the acetabulum is formed incorrectly - its size is reduced, and the cartilaginous rim is underdeveloped. Femoral dysplasia is characterized by a violation of the angle of articulation of the femoral neck with its body. And rotational pathology is manifested by changes in bone geometry in the horizontal plane.
Pediatric orthopedists also classify newborn dysplasia depending on the severity of hip joint underdevelopment. The degree of pathology always becomes the determining factor when choosing treatment methods.
| Severity of hip dysplasia | Characteristic features of the pathology |
| First (pre-dislocation) | The osteochondral elements are underdeveloped, the muscles and ligaments are not pathologically changed, the head of the femur is not deviated |
| Second (subluxation) | Underdevelopment of the bone and cartilaginous structures of the hip joint caused displacement (dislocation) of the femoral head upward and outward |
| Third (dislocation) | The articular surfaces do not contact each other, which leads to the femoral head slipping out of the acetabulum |
Symptoms of pathology
The characteristic symptoms of hip dysplasia are also the main diagnostic criteria. The pathology can be detected by a pediatric orthopedist when examining a child in the maternity hospital. The doctor assesses the condition of the hip joints by the position and size of the legs, the mutual correspondence of skin folds in the thigh area, muscle tone, and the range of active and passive movements.
In newborns
The most informative symptom in newborns is shortening of the femur. The doctor places the child on his back, bends his hip and knee joints. Dysplastic changes are indicated by the location of one knee lower than the other. It is imperative to identify the Marx-Ortolani symptom with the child lying on his back with his legs bent. Dysplasia is indicated by a characteristic click, clearly audible when the hips are evenly and gradually abducted to the sides.
In infants up to one year old
In children under 12 months, in addition to the above symptoms, pathology can be diagnosed by detecting other specific signs of hip joint underdevelopment. The asymmetrical arrangement of the inguinal, popliteal, and gluteal skin folds is informative only after 2-3 months. In young children, this condition is quite physiological and is a variant of the norm. Dysplasia is also indicated by limited movements when the legs are abducted to 50-60 degrees.
In babies after one year
By the end of the first year of life, the child takes his first steps. If for some reason dysplasia was not detected earlier, now it may be indicated by the child’s gait features. When dislocated, he limps, as if “waddling” from side to side, trying to stabilize the position of the body when moving. Indirect signs of pathology include walking “on tiptoes” and turning the foot inward.
spacers for children with dysplasia
Why would an orthopedist treat a problem that doesn’t exist? Because he must support a huge industry, which includes manufacturers and sellers of supposedly “correct” shoes and insoles, massage therapists.
I warn you right away that my opinion is unprofessional, incompetent, emotional and, apparently, unpopular in Russia. I’m just Masha, who knows how to google, analyze information and observe what kind of shoes foreign children wear. And I want to tell you that, in addition to the domestic school of orthopedics, there are some other points of view and they are very common throughout the civilized world.
You can swear, you can disagree, you can consider me a fool, you can breathe a sigh of relief, you can thank me, I’m still not responsible for my words)
***
Every orthopedist in Varina’s life said: “flat-valgus placement of the feet. The right shoes, massage, exercise therapy.” Particularly sophisticated ones recommended paraffin, electrical stimulation, standing on peas, cutting off the soles of sandals on an incline.
Of course, I bought supposedly correct orthopedic shoes with high, hard heels, arch support, heels and other crap. We had a massage once every six months. I haven't seen any improvement.
As usually happens, the truth was born from doubt
Varina's last correct sandals ran out when we were getting ready to go abroad. I didn’t have time to order ortho shoes in Russia and left on our long trip with the hope of buying shoes there. “There’s probably a larger selection of good shoes abroad,” I thought.
I came to a shopping mall in Hong Kong and there were no proper shoes in either the first mall, or the second, or the third. I only found the Dr Kong store, but even these shoes did not fully meet the precepts of domestic orthopedics.
Meanwhile, 70% of Hong Kong children were wearing Crocs, another 20% were wearing New Balance, and the rest were wearing unidentified Chinese shoes.
In Bali, I also did not see a single child wearing preventative or orthopedic shoes. Not from locals, not from foreign tourists.
There is such a cool joke that is actually not a joke at all: children from Russia abroad can be recognized by their shoes. Indeed, if a child walks towards you in socks and high sandals with a backdrop, arch support and other conditions, then this is a Russian-speaking kid. In Hong Kong, Indonesia, Singapore and Thailand, all foreign children wear random shoes.
Again, if you order clothes from European or American online stores, you have probably noticed that their entire range of shoes completely contradicts the logic of domestic orthopedics.
And here I finally come to an explanation of my position. There are two schools of orthopedics, roughly speaking, ours and not ours. True, if you read the Medservice forum, you can conclude that some orthopedists are finally emerging from the darkness and are leaning toward Western orthopedic thought. Which is what I'm trying to convey in this post.
Overdiagnosis
Why would an orthopedist treat a problem that doesn’t exist? Because he must support a huge industry, which includes manufacturers and sellers of supposedly “correct” shoes and insoles, massage therapists. Because if flat feet or valgus does not go away with age, no one will be able to say that they did nothing. Because mothers are often not satisfied with the recommendation “don’t do anything - everything will go away on its own.”
Most children have no problems with their feet (and below I will tell you that neither flat feet, nor valgus, nor club feet are something that needs to be corrected), and the tradition of taking a child to an orthopedist before the age of 3 can be abolished.
Okay, not all children are equally healthy. But if the child really has something, then the doctor does not write down “correct shoes, massage” on the card, but undertakes a real therapeutic attack, gives directions for x-rays, examinations, a prescription for making shoes, etc. If your child was not sent along this route, then you can relax: everything is normal with him.
When an orthopedist tells some abstract mother (actually, me) that the child has hallux valgus, her world collapses, she comes home and begins to monitor the Internet for this terrible diagnosis.
There are a lot of articles on the Internet, written in beautiful and incomprehensible semi-medical language, which explain in detail why children from birth need to wear orthopedic (even not prophylactic) shoes. (For example). But for some reason all these articles are posted on the websites of stores of orthopedic shoes, insoles and other gadgets. Even I, a person without a medical education, am perplexed by the following words:
In the absence of rational shoes - with a rigid sole and a bend line at the level of the metatarsophalangeal joint, fixation of the talocalcaneal joint due to the rigid rear part with lateral tibia and alignment of the longitudinal-transverse arch of the foot with the help of an instep support - flat feet are formed, and subsequently - planovalgus deformity stop.
It turns out that flat feet happen when a parent does not buy orthopedic shoes for their child.
Orthopedic, preventive, correct shoes
Let me start with the fact that orthopedic shoes are not orthopedic shoes at all :) For some reason, many parents believe (not without the marketing efforts of sellers of children's shoes) that a) any shoes that look orthopedic are orthopedic, b) orthopedic shoes are useful.
Although, by the way, ortho shoes are therapeutic shoes, the insoles for which are made according to an individual impression or scan of the foot and the purpose of wearing them is to treat various deviations from the normal development of the foot.
Everything that is mass-produced and sold in stores is ordinary shoes that want to look like orthopedic ones. For some reason they call it preventative. These shoes are supposedly a guarantee that the child who wears them will not develop flat feet or valgus.
And these shoes seem to work, because by adulthood, children really become ok with their feet. Although this happens not thanks to the shoes, but in spite of them. Despite the rigid, inflexible sole, which prevents the leg from bending. Contrary to the anatomically incorrectly positioned arch support. Contrary to the boot that constrains the leg. Because a normal active child will in any case overcome parental care for his legs.
The situation with ortho shoes is as if wheelchairs or crutches became fashionable and all healthy people began to buy themselves something similar to a wheelchair or crutches.
In our country, people like to buy orthopedic shoes for children just in case, just in case. Ortho shoes for the first step, ortho shoes for walking, ortho shoes for the home. It’s good if these pseudo-orthopedic shoes are just a marketing scam.
Our first orthopedist named Gabisonia (St. Petersburg, clinic No. 112) looked at Varya at the age of 1. He really looked, without getting up from his chair, without touching the child with a finger. Varya did not walk on her own then, only by hand.
With his golden eye, he diagnosed flat-valgus feet (and I do not dispute this fact) and prescribed sandals with high tops, arch supports, and heels. Wear at home all day. (The same orthopedist found dysplasia in my friend’s daughter, prescribed a cast and some kind of spacers. At the Research Institute of Orthopedics and Traumatology, the doctors pointed a finger at this matter and sent my friends home).
Orthopedist Gabisonia showed me an example of “correct” shoes (it seems to me that in hell they give out something like this):
Our whole family goes barefoot at home. And the news that Varya has to walk around in uncomfortable sandals all day upset me. I also didn’t understand why a child who had just gotten to his feet and was still tentatively taking his first steps needed to be shackled in shoes. I still don't understand this logic.
The experiment with wearing “orthopedic” shoes at home lasted a couple of days. Varya was uncomfortable, I decided not to torture the child. Shoes were worn only where they were supposed to be worn - on the street.
The most common orthopedic “diagnoses”
Flat feet
Well, everything is clear here. 100% of children have physiological flat feet. The feet of a child under 3 years of age seem flat, because... the recess of the arch is filled with a soft fat pad. This form of flatfoot does not require treatment, since the arch of the foot, with proper development, normalizes on its own by the age of 5-6 years of a child’s life.
Some people believe that shoes with arch supports are a good prevention for flat feet. This is a lie and a provocation from shoe sellers, more on that below.
Plano-valgus placement of feet
I will dwell in more detail on the flat-valgus position of the foot, because Varya’s chart says exactly that. I deliberately do not call this a diagnosis, because it is not a diagnosis at all, but simply a statement of fact. It’s the same as if an ophthalmologist wrote “the child has brown eyes.”
If an orthopedist writes in the chart of a child who is 1 (2, 3, 4 years old) “flat valgus feet,” then he is Captain Obvious. Because up to 5 years old, flat-valgus feet are a normal variant and do not require treatment or adjustment. For a child who leads an active lifestyle, everything will correct itself. If at the age of 5 it has not yet improved, then you need to do something, attack orthopedists, tear out your hair, gouge out your eyes.
Valgus (and varus) occurs when some muscles are not sufficiently developed. In Varin's case, this is the inner part of the calves. Will shoes fix this situation? Has any person you know pumped up any muscle simply because they wore some special clothes or shoes? Only active activities and physical exercise, only hardcore!
What to do?
Buy shoes that don't hurt. (More on this below).
Allow the child to run, jump, crawl on climbing frames, and climb stairs.
Jump - on mats, on a trampoline, on a bed.
Climb the wall bars, stand on the crossbar.
Ride a bike.
From a certain age, you can send your child to choreography or dancing. Or go swimming. Or everywhere.
Please don't waste your money on "orthopedic" or "prevention" shoes. Use the money you save to buy a wall bars, mat or trampoline.
Buy special massage mats with uneven surfaces and place them at home in your child’s favorite hangout spots.
Allow your child to walk barefoot on grass, sand, stones - over any uneven surfaces.
Collect stones and pebbles from the street and take baths by walking on these stones (you can add sea salt to the water).
Contrast shower for feet.
Massage for very small children.
Meanwhile, paraffin and electrical stimulation have not proven their effectiveness.
What shoes should I buy?
Just comfortable, beautiful shoes made from natural materials with a flat insole and flexible sole, without instep support.
What specific brands can I recommend? Based on this opinion, I’ll name Little blue lamb, Jack&Lily, Pediped, See Kai Run. On my own behalf I’ll add Birkenstock and Ecco. Now I bought Varya Little blue lamb sandals and they are very cool:
Without arch support
Everyday children's shoes should not have an instep support. For some reason, everyone thinks that an instep support is a thing that will “press” the foot in the right place and there will be no flat feet. Bullshield! An instep support is a thing that cushions during physical activity.
If a child is prescribed shoes or insoles with arch support, then these must be custom-made insoles/shoes based on a cast or photograph. Because the arch support must be positioned correctly. In short, for a specific child - a specific instep support. But! Most children do not need an arch support at all.
Almost all domestic children's shoes already have an instep support. In most cases, however, this is only its appearance and a dummy. In fact, it breaks down after a week, does not absorb shock, and is a marketing bait for lovers of “ortho” shoes.
An instep support is needed when the foot cannot cope with shock absorption on its own. Then the instep support helps relieve the load on the leg. So, arch support is necessary in sports shoes for children and adults. At the same time, in children's everyday shoes, a really effective arch support can cause harm because:
- the area of the foot where the shock-absorbing arch should be formed is not trained and developed properly (since the arch support is in the shoe),
- when buying shoes for growth, the instep ends up in the wrong place and, instead of cushioning, interferes with the development of the longitudinal arches of the foot.
No rigid sole, the sole should bend.
Shoes should be made from natural materials (crocs are an exception wow).
Wide toe cap to prevent your toes from being squeezed.
The heel should be stable, securely fixing the heel.
Ideally, shoes should look as if they are not there and the child is walking barefoot.
So, brief conclusions of this huge post
- There are two diametrically opposed directions in orthopedics. Whom to believe is your choice.
- There is no need to “treat” with shoes and wear arch supports; this can stop the process of arch formation and flat feet will remain for life.
- Any correction must be individual. Fixing it incorrectly or unprofessionally can lead to even bigger problems. Here is a review from a mother who treated her child with shoes and instep supports.
- Arch supports in the form of soft “pillows” in ordinary shoes are not effective, because... they are too soft (hence they cannot support anything).
- Most “foot problems” noticed by parents are part of the natural development of a child’s foot, which ends by age 6.
- The “improvements” noticed by parents are not the result of wearing the “right shoes”, but only the natural development of the child’s foot.
- The need for mandatory instep supports in children's shoes (unless they are individually recommended by an orthopedic doctor) is nothing more than a myth, unconfirmed by official medicine, and is used by shoe manufacturers to increase shoe sales.
PS. Varyulya is 2 years old, and the valgus has become significantly less. I attribute this to the beginning of an active period of running and jumping, walking on uneven surfaces and refusing to wear the “right” shoes.
Masha Buzanova
Source
How to diagnose
The primary diagnosis is made on the basis of an external examination of the newborn and a series of functional tests to assess muscle strength, sensitivity, and range of motion. But even if characteristic signs of hip dysplasia are detected, additional diagnostic measures are required.
Instrumental
The diagnosis is clarified using radiography and (or) ultrasound examination of the hip joint. Ultrasound is informative in detecting joint underdevelopment in children from the first days of life. X-rays are carried out only after they reach 2-3 months, since the resulting images do not visualize non-ossified cartilaginous structures.
Differential
Symptoms of hip dysplasia may mask other diseases of the musculoskeletal system. X-ray and ultrasound examinations are also carried out as a differential diagnosis to exclude pathological and paralytic hip dislocation, metaphyseal fracture, arthrogryposis, rickets, and epiphyseal osteodysplasia.
Hip dysplasia in children - degrees, symptoms and treatment
Hip dysplasia in children is a fairly frequently diagnosed pathology, which in most cases is detected in newborns.
Such dysfunctions of the hip joints can lead to very serious consequences, including disability. The causes of this pathology may be genetic predisposition, hormonal influence and disruption of tissue formation during intrauterine development. Parents should know not only the treatment methods, but also the symptoms of the disease, because the consequences of hip dysplasia affect a person’s entire life.
Treatment methods
Therapy is aimed at the correct further formation of the hip joint in newborns. Only an integrated approach is used using all conservative methods of treating dysplasia. They complement each other, enhance and prolong the therapeutic effect.
Plastering
If dysplasia of high severity is detected, treatment is carried out by simultaneous reduction of the dislocation with further immobilization of the limb by casting. Orthopedists perform such manipulation only when the child reaches 2 years of age. Treatment can also be supplemented with skeletal traction.
Orthopedic devices
Orthopedic correction is the most effective method of treating underdevelopment of the hip joint of any severity. Long-term, often constant use of devices contributes to the correct formation of the hip joint, a gradual increase in range of motion, and restoration of all its functions.
Pavlik stirrups
Pavlik stirrups are the first soft orthopedic structure that began to be used in the treatment of pathology. It is still in demand today, as it does not unduly restrict freedom of movement in the hip joints. Pavlik stirrups consist of a chest bandage attached to the body with straps, small soft pads on the knees and straps connecting all parts of the product into one. Depending on the severity of the pathology, the device is worn for a period of 2 to 12 hours a day.
Freyka's pillow
Freika's pillow is a soft orthopedic product that fixes and holds children's legs bent at the knees in an extended position. Its design includes a thick knee roller, straps and fasteners for securely attaching the device to the child’s body. Freyka's pillow can be used in the treatment of dysplasia from 1 month. It is usually worn during the day and removed before bed. But with congenital dislocation, round-the-clock wearing is often indicated.
Vilensky tire
The Vilensky splint is an orthopedic device in the form of a leg spacer, equipped with fixing straps and lacing. The design also includes a regulator, with which the doctor adjusts the angle of hip abduction. The Vilensky splint is more often used in the treatment of severe underdevelopment of the hip joint. The device is designed to be worn around the clock for 3-6 months.
Tübinger tire
The Tübinger splint is an abductor orthopedic mechanism for the treatment of dysplasia in infants from birth to 1 year. The main components of the device are soft shoulder pads, hip pads, an adjustable spacer, white and red fasteners, and threads with beads. The Tübinger splint is used for continuous wear with short breaks for hygiene procedures.
Tire Volkova
The Volkov splint is an orthopedic product made of polyethylene, consisting of a bed for the back, an upper part that fits on the stomach and side elements that fix the legs and hips. The wearing regimen is determined individually depending on the severity of the pathology and the age of the child. The Volkov splint has recently been almost never used due to the lack of a regulating mechanism in the design and severe limitation of movements.
Gymnastic and massage techniques
Therapeutic gymnastics is used from the first days of therapy. Regular exercises help strengthen the muscles, ligamentous-tendon apparatus, and maintain the femoral head in the acetabulum. When choosing exercises, the doctor takes into account the child’s age, his general health, as well as the current stage of therapy - leg extension, hip joint stabilization or rehabilitation. A referral to a professional massage therapist specializing in the treatment of dysplasia to treat the gluteal muscles is required.
Physiotherapy
Throughout the treatment of dysplasia in newborns, physiotherapeutic procedures are carried out - magnetic therapy, laser therapy, hyperbaric oxygenation, amplipulse therapy, ultrasound therapy. Under the influence of physical activity, the blood supply to tissues with nutrients necessary for the proper formation of bone and cartilaginous structures of the hip joint improves.
Surgery
If conservative therapy is ineffective and there is severe deformation of the hip joint elements, surgical treatment is indicated. More often, open reduction of the dislocation is performed - dissection of the articular capsule followed by installation of the femoral head in the acetabulum. Surgical methods for treating dysplasia also include osteotomy, which is performed to give the proximal end of the femur the correct configuration.
Symptoms of hip dysplasia
Signs of hip dysplasia in infants are very characteristic; they are pronounced even in the first year of life. The doctor and parents should be alert to the following factors:
- folds on the popliteal and gluteal cavities are located asymmetrically
- when spreading the legs in a bent position, the baby shows obvious dissatisfaction and cries
- spreading the legs bent at the knees is problematic.
If these signs occur, parents should seek advice from an orthopedist, who will conduct a full examination of the baby and prescribe an ultrasound examination of the hip joint.
The most pronounced symptoms of the third degree of the disease in question are:
- A “clicking symptom” is present. This sound will be heard at the moment of spreading the legs, bent at the knees, to the sides, and the click is heard both at the moment of spreading and at the moment of bringing together.
- Asymmetry of skin folds. The child should be placed on his stomach or back, paying attention to the depth and height of the folds. The number of folds does not play any role in diagnosis, because this indicator is variable even in absolutely healthy children.
- Restriction when spreading the legs to the sides. It is with the help of this symptom that congenital hip dysplasia is diagnosed already on the 5-7th day of a baby’s life.
- Shortening the leg. This sign can be checked in the following way: the child is placed on his back, his legs are bent at the knees and his feet are placed towards the table or other surface on which the baby is lying. If the child is healthy, then his knees will be at the same level, otherwise one knee will be slightly higher than the other.
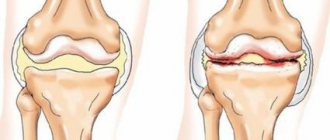
Prognosis and complications
With timely treatment, the prognosis is favorable. If for some reason therapy was carried out late, then there is a possibility of developing coxarthrosis in adults - arthrosis of the hip joint. Unreduced hip dislocations are also dangerous. Over time, a “false” joint forms in combination with shortening of the leg and pathological changes in the muscles.