Cruciate ligament repair is an invasive procedure aimed at restoring the cruciate ligament. It involves arthroscopic surgery on the joint, which involves removing the damaged ligament and replacing it with a graft. Plasty of the cruciate ligament of the knee joint is also called reconstruction or transplantation.
At CELT you can consult an orthopedic traumatologist.
- Initial consultation – 3,000
- Repeated consultation – 2,000
Make an appointment for
Arthroscopic plastic surgery of the posterior cruciate ligament of the knee joint (excluding the cost of consumables) - 130,000 - 170,000 rubles.
Arthroscopic plastic surgery of several ligaments of the knee joint (excluding the cost of consumables) - 140,000 - 180,000 rubles.
Arthroscopic plastic surgery of the anterior cruciate ligament of the knee joint (excluding the cost of consumables) - 115,000 - 150,000 rubles.
Included in the price:
carrying out the operation, consultation with an anesthesiologist, anesthetic care, all dressings, medications, food and hospital stay, postoperative observation by the attending physician.
30-90 minutes
(duration of procedure)
1-2 days in hospital
Indications
- rheumatoid or bacterial arthritis;
- gout;
- pyrophosphate arthropathy;
- ochronosis;
- synovial chondromatosis;
- villous-nodular synovitis;
- hemangioma;
- synoviome.
Contraindications
- severe somatic condition;
- high risk of complications;
- purulent-inflammatory diseases of the skin and subcutaneous tissue of the leg;
- bony or fibrous ankylosis of the knee joint.
Information: Cruciate ligament reconstruction
- Duration of stay in the clinic: 3 days
- Outpatient rehabilitation: within 4 weeks
- Earliest time to fly home: 10 days after surgery
- Recommended time to fly home: 14 days after surgery
- Showering possible: after 7 days
- Duration of incapacity for work: 6 weeks (depending on the type of activity)
- Stitch removal: 7-12 days
- Driving a car is possible: after 6 weeks
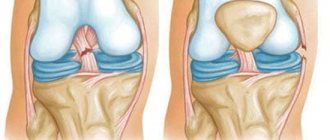
The anterior and posterior cruciate ligaments are the central supports of the knee and its main stabilizers. The damage to the anterior cruciate ligament is clearly visible. When the ACL ruptures, the lateral ligaments of the knee joint can also be damaged. © Istockphoto.com/MedicalArtInc A ligament tear causes joint instability, which leads to significant wear and tear in the future. In Germany, 350,000 knee injuries involving cruciate ligament rupture occur every year. 80% of cases are treated with cruciate ligament reconstruction (ACL reconstruction). Clinical and experimental studies show that spontaneous healing of cruciate ligament ruptures does not occur. On the contrary, existing instability entails the development of secondary damage such as meniscus tear and the development of knee arthrosis.
If the cruciate ligament is torn, it is not necessary to perform an immediate cruciate ligament transplant. It is often possible to stitch (reconstruct) a partially torn cruciate ligament. In this way, cruciate ligaments that are torn from the bone at their attachment points in the femur or tibia can be reattached.
It is very important for us, depending on the mechanism of injury, to offer the patient a suitable method of treating a cruciate ligament rupture.
The effectiveness of surgical treatment of ACL rupture
When a patient is faced with the task of returning to sports, the only effective treatment option is anterior cruciate ligament surgery. A satisfactory result is achieved in 85-93% of surgical interventions (Hofbauer V., Valentine P., 2010; Mihelic R., Jurdana H. 2011). At the same time, a return to sports to the previous level occurs in 50-70% of cases.
Reasons why maximum results and the return of physical activity to the previous level are not achieved:
- Incorrect assessment of the instability option means underestimation of rotational stability. Often, an ACL tear occurs along with other injuries to the knee joint. Without their restoration, its full functioning is impossible.
- Incorrect reconstruction technique - technical errors of the surgeon or technology: the main one - individual anatomy is not taken into account (technological errors, “guides”, incorrect interpretation of the anatomical structure or ignorance), etc.
- Violation of the biological conditions for the restored graft: bone tunnels, features of graft formation for subsequent accretion and ligamentization, features of its fixation (design features of fixators).
- Lack of individual adequate rehabilitation or its inconsistency with the capabilities of the joint and graft.
- Lack of medical monitoring of the condition of the knee and graft until the completion of rehabilitation (until its growth and full blood supply).
Priorities for successful ACL reconstruction surgery.
First of all, this is taking into account biological processes, namely:
- Anatomy, i.e. individual features of the anatomical structure of the joint - i.e. correct placement of the graft. Although the knee joint is roughly similar, each person is different and the correct location for each is how the ligament was positioned before the injury.
- Selection of the shape and characteristics of grafts. The graft must be anatomically correct in shape with a high degree of strength and engraftment.
- Creation of biological conditions for graft growth to the bone base.
- During the rehabilitation process, it is important to provide it with an active blood supply so that the ligament gains strength and ligamentizes.
- With the beginning of active movements, it is necessary to create such conditions so that the graft does not have any negative preconditions for mechanical damage and maintains the tension created during the operation.
Read more about knee arthroscopy: "".
Reconstruction of the cruciate ligament using the ACL method
Currently, this method is used as a standard treatment procedure if the anterior cruciate ligament tear is more than 50% of its diameter.
There are several variations of this method. But the principle is the same everywhere: with plastic surgery of both the posterior and anterior cruciate ligaments, the patient’s own tendon is an autologous graft replacing the torn cruciate ligament.
The tendon is pulled through a tunnel drilled into the thigh and lower leg. The cruciate ligament graft is then secured in the tunnel.
The difference between the options is as follows:
1. Graft selection
- semitendinosus tendon / Gracilis tendon, or patellar tendon (Patelladrittelsehne)
2. Material selection
to secure the implant (threads, screws, polyethylene pins).
Which method will be used is decided individually, before the operation begins.
Where does the cruciate ligament graft come from?
If the semitendinosus tendon/Gracilis tendon is used, it is removed approximately 25 cm long through a short incision on the inside of the leg. During the postoperative period, the remaining parts of the tendon heal so that there is no significant loss of strength.
Cruciate ligament reconstruction: During the preparatory stage, part of the semitendinosus tendon is removed. The graft is then processed and stretched to achieve maximum tensile strength. The location of the fence is selected individually in each case. But we prefer to harvest the patellar tendon or semitendinosus tendon © FH Orthopedics
If one-third of the patellar tendon is used, a short incision in the front of the knee below the kneecap removes the middle third of the patellar tendon at the edges, along with small bone fragments from the patella and tibia.
To perform a minimally invasive cruciate ligament repair, we usually use a third of the tendon from the front of the knee joint, because compared to other methods (for example, Hamstring tendon repair), the patient experiences less pain.
Especially using a third of the patellar tendon has clear advantages. The graft is removed with a small piece of bone from the kneecap, which makes it much easier to anchor the graft in the knee. These bone fragments grow into the graft attachment sites and stabilize the cruciate ligament graft. A graft from a third of the patellar tendon can withstand loads of up to 1800-2000 kg, which is not much lower than the maximum possible load of 2400 kg for a natural cruciate ligament. therefore, this tendon is very close in its properties to the natural cruciate ligament.
There is less postoperative pain when using the hamstring for cruciate ligament reconstruction. But it takes longer to heal because the hamstring cannot be removed with bone fragments. The length of the hamstring allows it to be folded into four, which greatly increases its strength. The graft can withstand a load of 2400 kg and thus matches the strength and stiffness of the natural cruciate ligament.
“Mistakes” when plasticizing the anterior cruciate ligament with artificial grafts
Introduction . Injury to the anterior cruciate ligament (ACL) of the knee is one of the most common ligament injuries. According to foreign literature, in the United States every year there are about 200,000 ACL injuries [1], mainly among athletes involved in sports such as football, rugby, and skiing. They are 10 times more likely to suffer an ACL injury than athletes in other sports. Moreover, women who play football, basketball, and rugby suffered ACL injuries 4 times more often than men who play these same sports [2]. The mechanism of ACL injury includes neuromuscular and biomechanical disorders, transformation of collagen fibers, hormonal factors, anatomical and structural factors [3].
Due to the high incidence of ACL injuries, approximately 100,000 ACL reconstructions are performed each year in the United States [4].
ACL plastic surgery is performed by two groups of grafts: autologous tissue (fragment of the quadriceps tendon, patellar ligament, semitendinosus tendon, etc.) and synthetic implants (LARS ligaments, DONA-M, lavsan, etc.). The reconstruction technique for both types of grafts is identical, with the exception of the material sampling techniques. However, it is not always possible to obtain the ideal location of the tunnels for the transplant, as well as its fixation with interference screws. Therefore, the results of the operation vary even among the same surgeon.
Purpose of the study: to analyze errors and complications during ACL reconstruction.
Materials and methods . In the period from 2009 to 2012, more than 200 patients were treated at the Saratov Research Institute of Traumatology and Orthopedics who underwent ACL reconstruction using the Dona-M synthetic graft. Of these, 78 patients (58 men and 21 women) were selected for this study and could undergo a follow-up examination at least 8 months after surgery (mean 16 months, range 8 to 24). The average age of the patients was 28±2 years. The mechanism of ACL injury in 58 patients (75%) was a domestic injury, in 15 patients - a sports injury, 20%, and in 5% of cases (5 patients) - an injury resulting from a road traffic accident.
All patients underwent surgical interventions by two surgeons using the same technique.
The research methods included an objective (x-ray) assessment of the results of plastic surgery; X-ray images in two standard projections were taken immediately after surgery and within a period of 8 months to 1.5 years after surgery.
ACL reconstruction was performed according to the manufacturer's instructions LARS (France). According to the technique, the tunnel in the tibia in the frontal plane relative to the axis of the bone should be 45-55º, and in the sagittal plane 25º. The exit point of the tibial tunnel on the tibial plateau should be 1/3 from its anterior edge or 7 mm from the anterior fibers of the PCL, which corresponds to the middle of the anatomical attachment of the ACL. On the lateral femoral condyle, the topical point for the channel should correspond to the anatomical attachment of the ACL. The tunnel in the femur in the frontal plane relative to the axis of the bone should be 45-55º, and in the sagittal plane 10-25º (Fig. 1). The graft is fixed with a titanium interference screw extra-articularly. In this case, the ideal position of the screw is considered to be as close as possible to the articular surface, which eliminates the occurrence of “wiper syndrome”. All patients underwent X-ray monitoring in the postoperative period.
The following indicators were studied:
- Location of tunnels in the femur and tibia in direct and lateral projections.
- The angle of the tunnels relative to the axis of the limb.
- Depth of insertion of interference screws.
Rice. 1. The angles of the tunnels and the insertion of screws correspond to the manufacturer's recommendations.
Results and discussion . The results of plastic surgery were assessed using radiography in standard projections (frontal and lateral).
Table 1. Deviation of the location of tunnels from the norm
From the table 1 it follows that when tunneling in the thigh on photographs in the frontal projection, the displacement of the tunnels from the norm by 5-8 mm was in 57% of patients, and in the lateral projection - in the majority of patients (75.9%), the deviation from the norm was 3-5 mm. On X-ray photographs of the lower leg in direct and lateral projections, the tunnels were displaced by 5-8 mm. In Fig. Figure 2 shows an x-ray of a patient with a deviation in the location of the tunnels by 8 mm or more.
Rice. 2. The tunnels are located with a deviation from the norm of more than 8 mm.
Table 2. Tunnel angles
In table 2 indicates that the angle of the tunnel in the femur on the direct projection was shifted by 10-20° in 55.7% of patients, and in the lateral projection up to 10° in 79.7%. The angle of the tunnel in the lower leg, as well as the thigh, was shifted by 10-20° in the direct projection, and up to 10° in the lateral view. In Fig. Figure 3 shows an x-ray of a patient whose tunnel angles are shifted by 20-30°.
Rice. 3. Shift of tunnel angles from the norm by 20-30°.
Table 3. Screw position in the tunnel
From the table 3 it follows that insufficient screw insertion in the femur was 3-5 mm on the straight and lateral sides in 48.1% and 50.6%, respectively. In the lower leg it was also 3-5 mm in both projections in 69.6% of patients.
As follows from the results obtained, most surgical interventions had deviations from the standard technique within acceptable values. In Fig. 4 provides radiographs of a patient with insufficient screw insertion of >8 mm.c
Rice. 4. Insufficient screw insertion >8 mm.
The results of treatment of 78 patients were assessed after 12 months. The majority of patients, 85%, returned to their previous level of sports activity and work activity. In this case, intra-articular effusion was observed in 3 (3.8%) patients, and in all cases the amount of aspirated clear synovial fluid did not exceed 10-20 ml. A limitation in the range of motion of more than 30° was noted by 9 patients (11.5%). Physical and instrumental assessment of the capsular-ligamentous apparatus of the operated knee joint showed that the difference in the anterior displacement of the tibia did not exceed 1-2 mm in the majority of patients 69 (88.4%), anterior displacement of 3-5 mm was diagnosed in 3 (3.8 %) of patients, a displacement of 5 mm or more was observed in 1 patient (1.2%).
When studying the pivot-shift symptom 12 months after surgery, the absence of rotational displacement of the tibia on the side of the operated joint was detected in 69 (88.5%) patients. Smooth sliding of the lateral condyle of the tibia was found in 7 (8.9%) patients, a noticeable jump in 1 (1.3%). Rough posterior movement of the lateral condyle of the tibia was diagnosed in 1 (1.3%) patient.
Overall, 71 (91%) patients were able to return to their previous level of physical activity.
Discussion . Arthroscopic ACL repair is one of the most complex endoscopic interventions on the knee joint. This is facilitated by the traumatic nature of the operation itself (by the standards of minimally invasive operations) and the need for precise installation of the implant. The outcome of treatment is influenced by many factors, the most important of which are the anatomical placement of the implant and the peculiarity of its fixation. As the results of the study show, even for one operating surgeon, the probability of different insertion of interference screws when placing an implant is quite high. However, in the world literature there is no exact data on the boundaries of the “permissible norm”, within which one or another position of the screws is possible. Although it is the position of the fixators that can have a critical impact on the results of treatment. First of all, this is the most common complication - “wiper” syndrome, in which the implant loosens and the canal in the tibia or femur expands. Windshield wiper syndrome occurs when the screws are not inserted close enough to the articular surface. Most often this occurs on the side of the lower leg.
The angle of the canals also plays a big role in the postoperative functioning of the knee joint. In this case, both its position in the frontal and sagittal planes is important. The most common “mistake” in this case is placing the canal in the thigh anterior to its normal location. It leads to the fact that at maximum flexion in the knee joint, excessive tension occurs on the implant, and it slips between the interference screws, which leads to relapse of instability. The angle of the canals in the frontal plane influences the treatment outcome to a lesser extent.
conclusions
- When performing arthroscopic ACL repair, one of the key points is the correct formation of tunnels, maintaining the angles when making tunnels, and placing the interference screws as close as possible to the articular surface.
- When the same surgeon performs ACL reconstruction without the use of intraoperative X-ray control, deviations from the standard technique are possible in up to 23.8% of cases.
Graft preparation for cruciate ligament reconstruction
After collection, the tendon is prepared for transplantation in accordance with the standards and requirements for grafts. After harvesting, the hamstring tendon is folded into 4 layers, cleaned and pre-stretched © FH Orthopedics. Before implantation, the tendon is folded, cleaned and pre-stretched. If a third of the patellar tendon is removed, the angular edges of the bone are smoothed and shaped to ensure optimal placement of the graft in the tunnel through the femur and tibia.
Preparing the knee joint for cruciate ligament reconstruction
At the same time, the knee is also prepared for transplantation. The cruciate ligament implant must, like the natural cruciate ligament, be firmly anchored in the femur and tibia. For this purpose, anatomically corresponding channels are drilled in both bones. In these channels, the ends of the graft are securely fixed. At the attachment points, the implant grows into the bone over several months.
Image during knee arthroscopy: cruciate ligament implant transplantation. © Gelenk-Klinik.de
Treatment of associated knee injuries
Successful cruciate ligament reconstruction surgery includes treatment of associated injuries to the injury. When you twist (twist) the knee joint, other structures in the knee can be damaged. An experienced orthopedic surgeon will always check the knee for meniscus tears and cartilage damage during ACL surgery. Once treatment is complete, the cruciate ligament implant is inserted through an arthroscopically (minimally invasive) tunnel into the knee. The anchorage of the cruciate ligament implant, its position, as well as its functions are checked several times in direct line of sight.
Be attentive to yourself!
If people who suffered a knee injury had the opportunity to look inside their joint, they would lose the desire to put off treatment. When an essential item breaks, what do you do? Of course, you immediately take it to the workshop. With the knee joint, alas, this is not always the case: often we do not take care of it in the first place, and when we lose it we cry. Remember that if you do not consult a doctor in a timely manner, damage to one element of the knee joint will certainly lead to others, and some elements (for example, articular cartilage) may not be restored at all.
Fixation of the cruciate ligament implant
To secure the ligament in a stable manner, the graft is secured into the canal in a minimally invasive manner using absorbable (i.e., biodegradable) screws.
In case of poor quality bone tissue (Osteoprose), titanium screws are used. © FH Orthopedics. For stability, the graft is fixed in the tunnel with special screws. These screws are made of self-absorbable material and dissolve in approximately 2 years. Only in cases of poor bone quality are titanium screws used. In other methods of cruciate ligament reconstruction, loops are used for fixation, which are attached to the tunnel on one side and to the graft on the other.
In the lower leg, where removal of the fixation material is easily accessible, titanium screws or titanium staples can also be used alternatively.
Thanks to the arthroscopic surgical technique, knee injury, compared to open surgery, is insignificant, which has a positive effect on both postoperative recovery and the cosmetic result.
Advantages of ACLplasty.
- Partial weight bearing on the leg is allowed immediately after surgery.
- Almost painless tendon removal.
- No complications
- High graft strength
- Small, cosmetically invisible incisions.
- Rapid healing of the bone canal
- Fast wound healing allows athletes to begin training quickly
- By pre-stretching the cruciate ligament implant, optimal stability of the knee joint is achieved
Plastic surgery using the Legamis method
To perform the operation, specialists use a hypoallergenic steel sleeve and polyethylene thread, which are combined into a single structure. The sleeve is fixed in the bone tissue of the lower leg, and the thread is attached to the thigh bone. Using a thread, the surgeon connects and tightens the torn tissue, and then attaches it to the end of the sleeve. This ensures a strong fixation of the knee joint, which significantly accelerates regeneration after severe injury. Plastic surgery using the Legamis method is prescribed only if the injury occurred recently (no more than 15-20 days ago). The method was created by German surgeons and is used mainly in prestigious medical centers in Germany.
Possible complications after cruciate ligament reconstruction
Tunnel expansion after cruciate ligament repair
Large tunnel diameter is a risk factor, especially during revision surgery, for example after re-rupture of the cruciate ligament. The exact cause of the tunnel's excessive expansion has not been determined. Tunnel expansion can occur regardless of the type of implant and method of cruciate ligament graft attachment.
Mobility limitations and knee stiffness
The cause of limited mobility is usually arthrofibrosis. This is a restriction of joint mobility due to the formation of scar tissue, which leads to a deficiency in knee extension. Infectious diseases are often the cause of this type of scar after cruciate ligament reconstruction, but the exact cause remains controversial. There is reason to believe that too early onset of muscle building after cruciate ligament reconstruction contributes to the onset of arthrofibrosis.
Infections after cruciate ligament repair
After cruciate ligament reconstruction surgery, postoperative infection is rare. If it occurs, it can have catastrophic consequences, including the development of osteoarthritis in young patients. Especially the duration of the operation contributes to the occurrence of infection, so the graft must be processed sterilely and as quickly as possible.
When is it possible to put weight on the leg?
If the healing process is normal, full weight bearing on the leg is possible within two days after surgery. Compared to other methods of cruciate ligament reconstruction surgery, the ACL method has a great advantage because ensures rapid restoration of mobility. For example, with complete immobilization for 7-10 days, 50% of the muscle mass in the operated knee is lost. Muscle recovery on this scale can take up to 1.5 years. Often, balanced muscle recovery after unilateral muscle degradation is never achieved.
During the postoperative period, the focus is on relieving swelling of the knee joint
.
Subsequently, much attention is paid to maintaining and increasing the range of motion of the joint. In the third stage, which begins approximately 3-4 weeks after surgery, more intensive muscle building begins. At this stage of rehabilitation, the patient’s active participation and careful performance of the necessary exercises at home are necessary.
Everything happens much easier than it seems
Athletes are frequent guests at our clinic. They are sometimes surprised that an ACL rupture can happen so easily: with a sudden movement, impact or twisting. But there is nothing surprising here, since the knee joint functions strictly in certain planes and any, especially sudden, displacement or impact can lead to injury. Mila Kochetova has been involved in sports since she was five years old and has been fencing professionally for 12 years. She suffered a knee injury during training while playing football, and a year ago she had surgery with us to replace her ACL. “We had game training that day. Everything happened suddenly: I was standing at the goal, when I rushed for the ball, I felt a sharp pain in my knee. The result is a torn ACL,” Mila recalls now with a smile, having successfully undergone recovery.
When is it possible to play sports?
Since after surgery the graft initially loses strength, resuming sports is allowed no earlier than after 6 months. Until this time, the graft needs time to grow steadily into the joint. After the doctor gives permission to load the knee joint, you can resume all types of exercise. After 1 year, we assume that the strength of the cruciate ligament implant reaches that of the natural ligament. However, it should be noted that the knee joint is usually more susceptible to injury in the future due to the slightly lower coordination ability of the joint. This is especially noticeable in contact sports at high speeds (football, handball).
You can start swimming and cycling four weeks after surgery. Depending on the type of sport and intensity, starting a sport should be discussed with your doctor.