How does a torn ankle ligament manifest?
Ankle ligament rupture, symptoms of injury are characterized by patient complaints of pain in the ankle while walking.
Upon examination, a tumor and hematoma are discovered; touching the damaged area is very sensitive.
Orthopedic surgeon Eduard Viktorovich Zhezherya comments:
When a sprain occurs, the victim may be able to lean on his foot. With more severe damage, if the ligaments are torn, it is difficult and painful to move, the entire foot swells, you need to make an effort even just to lean on your leg.
Damage to the talofibular ligament of the ankle joint usually occurs when a person makes an unnatural movement - twisted or sharply twisted the leg, twisted too much. The sharper the movement, the more likely it is that the ligaments may become injured or damaged. At such an unfortunate moment, the balance is lost, the person falls, and it even hurts to get back on his feet. It happens that a crunching sound is even heard at this time.
Treatment of ankle ligament injuries
The use of platelet-derived growth factors in the treatment of grade 1-2 injuries of the lateral ligaments of the ankle joint
E.N.Bezuglov 2, E.E.Achkasov 1, E.M.Usmanova 3, 1. Department of Physical Therapy and Sports Medicine 2. Continental Hockey League 3. PFC CSKA
SUMMARY
In our clinic, doctor Bezuglov E.N. conducts consultations. Performs: - conservative treatment of musculoskeletal joint injuries; -groin pain; - damage to the muscles and capsular-ligamentous apparatus of large joints; -rehabilitation after surgical interventions on the musculoskeletal system
The article presents the results of treatment of damage to the lateral ligaments of the ankle joint in 40 male football players (average age - 24.0±1.3 years), who were divided into two groups of 25 athletes depending on the treatment methods used.
The timing of treatment and the duration of pain persistence depending on the treatment method were analyzed. A new method for treating the ligaments of large joints using platelet-derived growth factors has been proposed, which can significantly reduce treatment time, reduce the severity of pain and reduce the number of recurrent injuries. It has been shown that the effectiveness of using platelet-derived growth factors is equally high in the treatment of both first and second degree injuries.
Introduction.
Introduction. Injuries become an indispensable attribute of the career of almost any athlete.
According to European experts, up to 50% of all sports injuries, as well as 3.5-10% of all injuries treated in hospitals, are associated with playing football [7]. Among all sports injuries, the most common are injuries to the ligamentous apparatus of large joints, and that is why the full treatment of these injuries, as well as the fastest possible rehabilitation with a return to the previous level of activity, becomes of utmost importance [9].
The maximum number of injuries occurs in the capsular-ligamentous apparatus of the ankle joint—up to 17% of all sports injuries. Most often he is injured when playing football, which is one of the most traumatic sports [3]. Ankle joint injuries account for 15% of all emergency sports injuries, of which 85% are inversion injuries [5].
According to a study conducted by the UEFA Medical Committee, more than 12% of all injuries to football players of leading European clubs were injuries to the ankle joint, of which about 38% were injuries to the lateral lateral ligaments, which, in turn, significantly prevail in the structure of all injuries to the ankle ligaments - more than 80% of all cases.
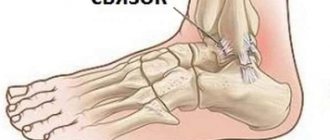
The lateral group of ligaments of the ankle joint is represented by the anterior talofibular ligament (ATFL), posterior talofibular ligament (PTFL) and calcaneofibular ligament (CFL).
The severity of damage to the PTMS and PMS is the basis of functional tests that determine the extent of injury. There are several classifications of damage to the capsular-ligamentous apparatus of the ankle joint, which are based on assessing the degree of damage to certain anatomical structures [2].
In our opinion, the most revealing is Hamilton’s classification [4]. Since it better displays the relationship between diagnosis and anatomical structure, as well as the mechanism of injury:
- Grade I – sprain of any ligament
- grade II – PTMS rupture, PMS is not damaged
- degree III – rupture of the PTMS and PMS.
A very important aspect in the treatment of damage to the capsular-ligamentous apparatus specifically in highly qualified athletes is an adequate assessment of the pain syndrome immediately after injury, as well as during treatment, since in some cases it is the pain syndrome, and not the degree verified using instrumental research methods. Ligament damage becomes the main limiting factor for starting full-fledged training.
Pain syndrome is most often assessed based on the patient’s subjective sensations using developed pain scales.
To assess the intensity of acute pain in clinical practice, the Visual Analog Scale (VAS), the Numerical Rating Scale (NRS) and the categorical Verbal Rating Scale (VRS) are widely used.
The main drawback of all the described scales is the assessment of pain at rest or during the usual load for the patient being interviewed. At the same time, the absence of pain at rest or during routine exercise is not an indicator for athletes of the positive dynamics of the healing process, or even more so of recovery, since limiting pain can appear during or after a specific load. Taking into account the above disadvantages, we developed and for the first time introduced into practice a scoring system for assessing pain specifically among highly qualified football players.
Classification of pain syndrome in football players
- there is no pain when performing physical exercises of any intensity and does not appear after it
- there is minor discomfort, appearing only after exercise and spontaneously stopping
- does not interfere with exercise of any intensity and does not intensify after it
- limiting pain appears only at the peak of a specific load
- limiting pain appears when performing a specific load of moderate intensity
- pain appears during clinical tests
- pain occurs when running
- pain occurs when walking fast or doing other similar activities
- pain occurs with any movement
- -pain at rest
A method for selecting diagnostics of damage to the ligamentous apparatus, which can be used both for and for assessing the course of the process.
In addition to the mandatory methods (ultrasound and radiography) of examination for damage to the ankle ligaments, computed tomography can be used to exclude osteochondral damage and help diagnose concomitant bone contusion and swelling, the presence of which affects the duration of recovery[18].
Over the past decades, in the world practice of treating injuries to the ligamentous apparatus of the ankle joint, the opinion has been established about the need for minimal immobilization of the joint in order to quickly stop the accompanying inflammation and accelerate repair 8].
Treatment of ankle ligament injuries is 14].
Damage to the ligaments of the ankle joint is accompanied by Therefore, all initial treatment tactics should be based on the elimination of pain.
RICE therapy is used as a starting therapy, which includes resting the joint through partial immobilization, accompanied by cooling, compression and elevation [17].
The end of the treatment of all types of ligament injuries in athletes is the absence of pain in the absence of pain.
One of the simplest and at the same time safest and -ligamentous apparatus in athletes is infiltration of the place obtained from.
This technique has been used for quite a long time in leading European and American clinics, and in the CIS it is most actively used in Donetsk [1].
In recent years, numerous studies have proven the important regulatory role of various growth factors in the healing processes of damaged tissues[6].
The use of platelet-derived growth factors in clinical practice can significantly accelerate tissue healing processes while simultaneously improving the quality of the scar) [13].
The pathogenetic basis of this method is the presence in platelets of alpha granules containing a large number of growth factors, which are stimulators of regeneration processes [16]
For athletes or professional athletes, the impact of musculoskeletal injuries on life and work is much greater than for ordinary people, so rapid restoration of full performance and return to competition is of paramount importance [15].
Optimal treatment of injuries in this group of patients should be aimed at returning to the previous functional level of activity as quickly as possible in the safest and most cost-effective manner [12].
The purpose of this study was to comparatively evaluate the effectiveness of treatment of grade 1-2 injuries of the lateral ligaments of the ankle joint using TFR and the standard method of treating such injuries.
Materials and methods. This paper summarizes the results of examination and treatment of 40 patients aged from 18 to 32 years (average age - 24.0±1.3 years) with injuries to the lateral ligaments of the ankle joint, who were treated at the medical center of the Luzhniki Olympic complex. Moscow in the period from 2009 to 2012. The degree of damage to the ligamentous apparatus was assessed according to the Hamilton classification. The duration of injury in all cases was 1-3 days.
All patients were male football players playing for clubs in the Russian Premier League and the National Football League.
In this study, only primary isolated injuries of the lateral ankle ligaments were analyzed.
At the time of the initial examination and functional tests for joint stability (“anterior” and “lateral” drawers), all patients underwent ultrasound examination (US) and radiography of the ankle joint, thus all diagnoses were verified.
The indication for the use of TGF injections was the desire of the patients.
All patients gave informed consent to treatment. All patients were divided into two groups depending on whether injections of platelet-derived growth factors were used or not.
Group I included 20 patients (50.0%) who received TGF injections as part of standard treatment. A blood sample of 36 ml (4 tubes of 9 ml each) was taken from the cubital vein. Platelet-rich plasma was obtained using a centrifuge from BTI (Spain), using a standard protocol of 1800 rpm for 8 minutes. The minimum platelet content in the plasma concentrate injected into the injury site was 800,000 per milliliter. TGF injection was performed once in a volume of 4 ml, injected into the injury site.
Group II included 20 patients (50.0%) who did not undergo TGF injections. Before starting therapy, all patients were assessed for the severity of pain using a developed scale. In both groups it was 7-10 points. All patients, regardless of the timing of the injury, received conservative therapy aimed at eliminating existing symptoms. Correction of existing pathological changes was carried out by intramuscular injection of Voltaren at a dosage of 3.0 ml once a day for three days, as well as by local treatment in the form of compresses with Lyoton and Voltaren gels. In both groups, physiotherapeutic treatment was carried out according to a standard regimen (cryotherapy 30 minutes 5 times a day for the first three days, magnetic therapy 30 minutes 1 time a day for the first 7 days). Considering that grades 1 and 2 injuries are stable and that functional tests did not reveal joint instability, joint immobilization was not performed [18].
The results obtained were assessed based on the number of days from the moment of injury to the start of full testing training and the number of relapses of injury over the next 6 months. The criterion for admission to the testing training, which included football-specific exercises of maximum intensity (Table 3), was a reduction in pain to 2-3 points on the developed scale.
Results and discussion: References: 1. Bezuglov E.N., Glushchenko A.L., Achkasov E.E., Yardoshvili A.E., Karkishchenko N.N. The first experience of using platelet-derived growth factors in the treatment of injuries to the musculoskeletal system of highly qualified athletes……………. 2. Renstrom P. Sports injuries. Clinical practice of prevention and treatment. - Kyiv: Olympic literature, 2003. - 93-94 p. 3. Ekstrand J. Soccer injuries and their prevention. // Linkoping University Medical Dissertations. 1982.- N.130. 4. Hamilton W. Stenosing tenosynovitis of the flexor hallucis longus tendon and posterior impingement upon the os trigonum in ballet dancers. Foot Ankle. // International SportMed Journal. 1982.-N.3.-P.74-80. 5. Henry J. Lateral ligament tears of the ankle, 1-6 years follow-up: study of 202 ankles//Orhop.Rew.1983.- Vol.10.- P.31-39. 6. Kasemkijwattana C., Menetrey J., Bosch P., Somogyi G., Moreland M., Fu F., Buranapanitkit B., Watkins S., Huard J. Use of growth factors to improve muscle healing after strain Injury// . Clin Orthop Relat Res.2000.- P.272–285. 7. Keller S., F. Noyes F., Buncher C. The medical aspects of soccer injury epidemiology // AM. J.SPORTS MED. 1987.-N.15.- P. 5-12. 8. Kerkhoffs G., Rowe B., Assendelft W. Immobilization for acute ankle sprain.//A systematic review. Arch Orthop Trauma Surg. 2001.- N.8.- P.46. 9. Kon E., Filardo G., Di Martino M., Marcacci M. Platelet-rich plasma (PRP) to treat sports injuries: evidence to support its use Knee // Surg Sports Traumatol Arthrosc.2007/-N.10. - DOI 10.1007/s00167-010-1306-y 10. Langer H. (2010) Platelets in regeneration.// Semin Thromb Hemost.2010.-N. 36.-P.175–184. 11. Lopez-Vidriero E., Goulding K., Simon D., Sanchez M., Johnson D. The use of platelet-rich plasma in arthroscopy and sports medicine: optimizing the healing environment // Arthroscopy.2010.-N. 26.-P.269–278. 12. Molloy T., Wang Y., Murrell G. (2003) The roles of growth factors in tendon and ligament healing// Sports Med.2003.- N. 33.-P.381–394. 13. Nagumo A., Yasuda K., Numazaki H., Azuma H., Tanabe Y., Kikuchi S., Harata S., Tohyama H. Effects of separate application of three growth factors (TGF-beta1, EGF, and PDGF -BB) on mechanical properties of the in situ frozenthawed anterior cruciate ligament // Clin Biomech.2005.-N. 20.-P.283–290 14. P. Renstrom. Persistently painful sprained ancle // J Am Acad Orthop Surg. 1994.-N.2.-P.270. 15. Sampson S., Gerhardt M., Mandelbaum B. Platelet rich plasma injection grafts for musculoskeletal injuries // A review. Curr Rev Musculoskelet Med.2008.- N. 1-P.-165–174. 16. Stellos K., Kopf S., Paul A., Marquardt J., Gawaz M., Huard J., Foster T., Puskas B., Mandelbaum B., Gerhardt M., Rodeo S. Platelet-rich plasma: from basic science to clinical applications// Am J Sports Med.2009.- N.-37.-P.-59–72. 17. Wedmore J. Emergency department evalution end treatment of ankle and foot injuries // Emerg Med Clin North Am. 2000.-N.18(1).-P.127. 18. Wolfe M., Uhl T., Mattacol C. Management of ankle sprains // Am Fain Physician. 2001.-N.63(1).-P.93.
What types of damage are there?
Injuries and ruptures of the ankle ligaments are classified into three types:
- ruptures of several fibers, which are more often called sprains, but this is incorrect, because ligamentous tissues are not capable of stretching at all.
- tears of most of the ankle ligaments. A patient with such an injury will be able to move independently.
- rupture of the ligaments of the leg joint or their complete separation from the place of attachment;
- rupture of the deltoid ligament of the ankle joint
Damage to the lateral ankle ligaments
Injury to the lateral ankle ligaments (sprain) occurs when the foot and ankle are subjected to stress beyond their physiological strength and range of motion, causing the ligaments to become overstretched or torn.
The mechanism of injury is usually ankle inversion (rolling or inward rotation) with or without elements of twisting along the vertical axis.
Damage can occur when walking on uneven surfaces or while running or playing sports.
Joint stability is ensured by two mechanisms:
- Dynamic stability - contraction of the muscles located around the joint and stabilizing it
- Static stability – provided by ligaments and the shape of the bones that form the joint
Dynamic stability is considered the most important of these two mechanisms for the normal functioning of the joint and the full performance of all movements familiar to us. If this mechanism is insufficient, the main load falls on the ligaments. Poor muscle function—weakness of the trunk, gluteus medius, quadriceps, hamstrings, and peroneus muscles—can predispose to ankle instability.
Proprioceptive sensitivity—the sense of position, location, orientation, and movement of a joint—is also critical to joint stability.
Patients with ligament hypermobility are also at risk for ankle ligament injury. The ligaments in such patients are not strong enough and provide a wider range of motion in the joint than usual.
A factor predisposing to damage to the lateral lateral ligaments of the ankle joint is also the specific shape of the patient’s foot. When the hindfoot is positioned varus (turned inward), as occurs in patients with pes cavus, the lateral lateral ligaments of the ankle joint are in a state of chronic hyperextension and lose their strength over time.
In summary, risk factors for injury to the lateral collateral ligaments of the ankle include:
- Walking on uneven surfaces
- Previously suffered ankle sprains (i.e. when the ligaments are already damaged)
- Insufficient dynamic stability
- Joint hypermobility syndrome
- Hindfoot varus (pes cavus)
- Diseases of the peroneal tendons
Appearance of hindfoot varus deformity predisposing to injury to the lateral collateral ligaments of the ankle joint
Ankle tendon rupture
If the ankle ligaments are completely torn, this is unmistakably and simply determined by the appearance of the sore foot and leg. There are clearly visible signs: the dorsum and lower surfaces of the foot with hemarthrosis, bruising, swelling spreading almost throughout the entire foot. The patient experiences pain with every step.
Damage to the ankle ligaments is confirmed, as a rule, after an x-ray examination, which at the same time makes it possible to exclude a fracture, which results in the same symptoms - swelling, severe pain when walking.
The patient may feel pain during the examination, as the doctor needs to turn the foot in different directions to accurately determine the location of the injury. Joint instability indicates that the ligaments are completely torn.
| Injection in the ankle joint for rupture of the talus ligament |
Sign up for treatment
Chronic lateral ankle ligament instability
Lateral ankle ligament sprains usually occur during walking or jumping (the foot undergoes supination and internal rotation while simultaneously externally rotating the tibia). The likelihood of injury increases with additional plantar flexion of the foot.
The anterior talofibular ligament is most often affected , followed by the calcaneofibular ligament . When the talofibular ligament ruptures, the mobility of the ankle joint in the horizontal plane increases, contributing to damage to the remaining ligaments. Damage to the lateral ligaments may be accompanied by damage to the ankle capsule and subtalar .
The most common injuries to the ligamentous apparatus of the ankle joint are injuries to the lateral complex, which in most cases can be treated conservatively. Repeated injuries to the lateral compartment ligaments can lead to chronic lateral instability.
Clinical picture
The main symptoms are complaints of instability, recurrent episodes of foot inversion, and pain, predominantly in the lateral malleolus .
Diagnostics
Anterior drawer test of the distal tibia (testing the integrity of the anterior tibiofibular ligament) and vagus test to assess instability. Anterolateral tenderness is often present and may indicate lateral impingement .
Standard X-rays may show calcifications (including round bony formations distal to the lateral malleolus), which is a sign of chronic lateral ankle ligament damage . osteochondral lesions may be identified on the lateral or medial edge of the talus .
The degree of pathological mobility in chronic instability can be assessed using comparative stress radiography.
Arthroscopic findings
When the joint is stretched, a significant expansion of the lateral joint space is noted. Sometimes the joint cavity can be explored down to the posterior capsule, which is always a sign of lateral instability or congenital weakness of the ligamentous apparatus. osteochondral damage is also identified . Local synovitis or adhesions are often found anterior to the fibula (lateral impingement) and in the area of the syndesmosis (syndesmosis impingement).
Treatment
Conservative treatment includes:
- Peace,
- Cold,
- Tight bandaging
- Elevated leg position.
Additionally, electrical stimulation and electrophoresis help reduce pain and swelling. If there are no fractures or damage to the syndesmosis, then rehabilitation begins immediately after the pain subsides. Rehabilitation is aimed at restoring range of motion, strength and proprioceptive sensitivity.
When a positive result is achieved, they begin to restore special skills: running, jumping, etc. To prevent recurrent injuries, wear lace-up ankle
Surgical treatment is indicated for:
- Repeated injuries
- Prolonged pain
- Persistent swelling or instability of the ankle joint.
In patients with repeated inversion injuries and widening of the lateral joint space, lateral stabilization of the ankle joint is recommended to prevent further injury from repeated subluxations. Both open and arthroscopic techniques .
Open surgery involves repairing the lateral ligaments using the captive peroneus tendon (peroneus brevis tendon transposition).
Arthroscopic stabilization was first described by Hawkins in 1987, who recommended practicing the arthroscopic technique on cadaveric models or joints.
Operation technique
Lateral stabilization:
Inspection
The anterolateral joint area is examined under distraction and varus loading, and ligamentous instability is assessed and documented. Chondral and osteochondral lesions of the talus are often detected.
Debridement
The anterolateral area of the joint is sanitized, removing local growths of synovial and scar tissue (causes of impingement).
Treatment
Approximately 1 cm anterior to the apex of the fibula, an area of the talus with a diameter of 6-8 mm is treated until a bleeding area of cancellous bone appears. A staple must be placed in this area to secure the anterolateral ligaments. Obstructing soft tissues are removed with a synovial resector.
Installing the bracket
To fix the anterior talotibial ligament and the lateral capsule area to the treated area of bone, a 5.5 mm staple is inserted through the auxiliary lower anterolateral port. The foot must be in a neutral position to provide sufficient tension to the lateral ligaments.
Checking the position of the bracket
The position of the staple is assessed by arthroscopy and under radiographic guidance. Instead of staples, a technique using anchor clamps (Mitek) can be used.
Possible problems:
- Loosening of staples
- Broken staples
- Possibility of injury when removing staples.
Hawkins, when removing staples after 3 months, often found that they were tightly fixed to the bone and could not be removed without additional trauma to the lateral capsule.