Reactive or allergic arthritis occurs as a manifestation of the body’s general reaction to a pathogen. The disease affects the joints (acute, subacute inflammation), being benign.
The risk group includes children prone to allergies, or those who have suffered food poisoning or infectious diseases. Common allergens include medications, food, pollen, and animal dander.
But not all children, even those at risk, develop reactive arthritis. An additional important factor is genetic predisposition.
The main distinguishing feature of this arthritis is that it is reversible. However, relapses are possible, and when the body is repeatedly exposed to the same allergen, the severity of the symptoms increases.
What is allergic arthritis
Allergic arthritis is an inflammation of the joints caused by an allergy to various particles entering the body. This disease develops especially often in children. Minor disruptions in the process of formation of the immune system lead, as a rule, to the development of an acute inflammatory process, which is easily treatable and ends without any consequences.
If the disease is based on complicated heredity, then sometimes the disease can become chronic with slow destruction of the joints.
The most common clinical form of this disease is infectious-allergic arthritis, which today is more often called reactive arthritis. According to statistics in our country, among rheumatic diseases, infectious-allergic arthritis in children under 14 years of age is more than 50%.
The code for allergic arthritis according to the International Classification of Diseases, 10th revision (ICD-10) is M13.8.
Allergic diseases can also include rheumatoid arthritis, which is based on an allergy to the patient’s own tissues. The ICD code for seropositive rheumatoid arthritis is M05.8; seronegative – M06.0.
Expert opinion
Rheumatologists emphasize that arthritis in children is a very insidious disease that can lead to disability of the child. Persistent joint deformities can remain for life and thereby reduce the patient’s ability to work. That is why you need to contact a rheumatologist in time for specialized help aimed exactly at the target. Early initiation of therapy helps reduce the risk of complications. In addition, the duration of treatment in the initial stages of the disease is significantly shorter than in advanced cases.
Causes of allergic arthritis
The cause of allergic arthritis is the body's increased sensitivity to various environmental factors - allergens. Allergens can be various particles that enter the body - food, particles of skin or animal hair, fish scales, medications, infectious agents, etc. The disease can also develop in response to the introduction of a vaccine or serum.
The introduction of an allergen into the body causes sensitization - increased sensitivity of the body to a certain substance - antigen. In response to the introduction of this substance, the body produces antibodies that neutralize it. When this allergen enters the body again, antigen (allergen)-antibody complexes are formed, deposited on the walls of target organs and causing an inflammatory process. In case of allergic inflammation of the joints, the target organ is the internal synovial membrane lining its cavity.
Allergic arthritis in children in most cases is of an infectious-allergic nature. Its onset is associated with a bacterial or viral infection. Most often it is a streptococcal, staphylococcal, intestinal or chlamydial infection. The disease is acute, benign in nature and with proper treatment of arthritis ends in complete recovery.
In some cases, in the presence of a hereditary burden (close relatives suffering from allergic diseases), an allergy to the infection first develops, and then an allergy to the patient’s own tissues joins it. In arthritis, it is an allergy to intra-articular tissue. As a result, a long-term, recurrent autoimmune inflammatory process develops that destroys the affected joint - rheumatoid arthritis.
In addition to children, persons suffering from diabetes mellitus, cancer, AIDS, sexually transmitted infections, other allergic diseases and chronic arthritis of various etiologies are prone to the development of infectious-inflammatory arthritis.
Symptoms of arthritis in children
The main symptom of all types of arthritis is pain in the affected joint. Its characteristics may differ depending on the cause of the disease and the individual characteristics of the body. However, each disease has its own characteristics, such as its favorite location, intensity of pain, presence of joint deformities, etc. The table shows the differential diagnosis of articular syndrome in various arthritis. This will help parents navigate the variety of symptoms and, without missing anything, contact a pediatric rheumatologist in a timely manner.
| Characteristics / Disease | YURA | Rheumatoid arthritis | Juvenile ankylosing spondylitis | Reactive arthritis |
| Localization | Small joints (hand, foot) | Large joints (shoulder, elbow, knee) | Leg joints involving the back | Knees, feet |
| Intensity | Expressed | Expressed | Moderate | Expressed |
| Peculiarities | Symmetrical lesion, morning stiffness for more than 30 minutes | Asymmetrical lesion, migrating nature of pain | Decreased spinal mobility | Combination with inflammation of the conjunctiva, genital organs, asymmetric damage |
| Joint deformities | Deformations such as “swan neck”, “walrus flipper” | Formation of deformations is not typical | Ossification of the joints of the spine with loss of mobility | Deformations are extremely rare |
In addition to articular syndrome, various arthritis may be accompanied by other symptoms:
- classic symptoms of inflammation - redness, swelling, decreased functional activity, increased local skin temperature over the lesion;
- fever up to 38-39oC;
- muscle pain;
- morning stiffness – the need to work out the affected joints after waking up;
- an increase in the size of nearby lymph nodes.
Decreased joint function can be manifested by lameness, inability to hold a pen, pencil, or perform household activities.
Symptoms
In most cases, allergic arthritis is acute. However, in the presence of constantly influencing internal or external predisposing factors, the process can become chronic.
First signs
The onset of the disease is acute or subacute, associated with the reintroduction of the allergen into the body. Inflammation can develop immediately or 1 to 2 weeks after repeated contact with the allergen. The joints swell, become inflamed, and moderate pain appears, intensifying with movement. Asymmetrical damage to joints involving small, medium and large (for example, knee) joints is also characteristic. Sometimes the patient’s general condition suffers: malaise, weakness, body temperature rises, and other manifestations of allergies appear in the form of a rash and Quincke’s edema. There is also a mild course of the disease with the absence of pronounced symptoms.
Obvious symptoms
Varying degrees of inflammation with swelling, redness of the periarticular tissues, and joint pain last for several weeks. All this time, general symptoms may persist: a slight increase in temperature, decreased performance, weakness, urticaria. Allergic arthritis lasts for 4 to 6 weeks, then complete recovery occurs. Infectious-allergic arthritis also has a similar outcome in most cases.
Swelling in allergic arthritis
When to Seek Medical Help
You should consult a general practitioner or rheumatologist if the following symptoms appear:
- painful sensations in the joints, intensifying after physical activity;
- swelling and redness in the area of one or more joints;
- general malaise, weakness, slight fever due to joint disorders and urticaria.
Persons prone to developing allergic reactions, suffering from other allergic diseases or chronic arthritis should pay special attention to such symptoms.
Symptoms of allergic arthritis in children
In childhood, the cause of the disease is most often infection. These may be untreated chronic ENT infections, intestinal infections, as well as chlamydia.
If the cause of infectious-allergic arthritis is a streptococcal or staphylococcal infection, the disease is acute or subacute, but almost always benign, ending in 1 - 1.5 months with complete recovery. Main symptoms: asymmetrical damage to the joints of both the upper (elbow) and lower (hip, knee) extremities, their inflammation, swelling, redness and pain in combination with general disorders: slight fever, weakness.
After intestinal infections caused by Yersinia, Salmonella, Shigella and some other pathogens, the disease also occurs initially acutely with asymmetric damage to the joints of the lower extremities. Often the hip joints are involved in the process. The process becomes subacute and lasts up to 3–5 months, after which complete recovery occurs.
Prolonged inflammation of the joints is typical when affected by chlamydia. This intracellular infection is difficult to detect and is prone to long-term recurrence, which maintains the inflammatory process in the joints.
Swelling in allergic arthritis in children
How dangerous is the disease?
Allergic arthritis is dangerous because upon further contact with the allergen, acute allergic reactions such as Quincke's edema and anaphylactic shock can occur. Sometimes the disease can take a chronic course with gradual destruction of the joints.
Stages of allergic arthritis
In the typical course of the disease, three stages are distinguished:
- Early
– with an acute course, asymmetrical damage to the joints, increased body temperature, and malaise. In adults, the ankle and foot joints are more often affected, which is often accompanied by damage to the ligamentous apparatus, pain in the foot and heel. In children, in most cases, the hip and knee joints, as well as the joints of the lumbosacral spine, are initially affected. Symptoms: pain in the buttock and sacrum, slight lameness, general malaise, weakness, fever, urticaria. - Expanded
– inflammation of other joints is associated, also asymmetrical. The pain intensifies, the process becomes protracted. Children often develop skin rashes and swollen lymph nodes. The temperature is slightly elevated or normal. There are no changes on the x-ray. - Final
– the disease ends with complete recovery after 4 – 6 weeks.
Possible complications
With infectious-allergic inflammation of the joints against the background of chlamydia, the process can become chronic. The disease occurs with relapses and remissions, and the development of destructive disorders and gradual loss of joint function is possible.
In children, infectious-allergic arthritis can develop into juvenile rheumatoid arthritis (JRA) if there is a hereditary predisposition.
To prevent complications, it is very important to consult a doctor in time: the progression of the disease can be stopped at any stage.
Any form of arthritis has serious complications, so you should not delay treatment.
See how easily the disease can be cured in 10-12 sessions.
Questions
- Which doctor treats arthritis in children?
A pediatric rheumatologist diagnoses and treats arthritis. - Do arthritis always cause deformities?
Persistent deformities are characteristic of juvenile rheumatoid arthritis and ankylosing spondylitis. However, they do not always occur. The basis for preventing deformation is timely consultation with a doctor and targeted treatment. - Is it possible to cure arthritis with folk remedies?
Traditional medicine is not a scientifically proven form of treatment. This means that it is not possible to predict the effect of certain medicinal plants on the child’s body. Using traditional medicine methods, precious time is lost, and the pathological process can take an aggressive course. To effectively combat arthritis, the use of medications aimed at interrupting the vicious circle of changes in the body is required. Traditional medicine can act as an auxiliary therapy, but not a basic one, and only after consultation with your doctor. - Is it always necessary to take “hormones” for arthritis in children?
Hormonal therapy is prescribed to children only with certain forms of arthritis if there are absolute indications.
Classification
Allergic arthritis develops for various reasons and manifests itself in various clinical forms. The most common of them are infectious-allergic, toxic-allergic, and rheumatoid arthritis. Most of them can occur in the form of acute, subacute and chronic arthritis.
Infectious-allergic arthritis
Currently, infectious-allergic arthritis is more often called reactive arthritis, since it is based on an allergic reaction to a specific infection. In children, allergic arthritis of this form develops mainly after intestinal infections and upper respiratory tract infections. Women and children, including small ones, are more often affected; the disease progresses acutely or subacutely and lasts for 4–6 weeks and ends with complete recovery.
The main symptoms: the lesion is asymmetrical, pain appears in the joints, aggravated by movement, swelling and redness of the periarticular tissues. In adults, small (feet and hands) and medium-sized joints are affected, in children, most often large (hip, knee) and medium-sized (elbow) joints are affected.
With chlamydial infection, which is difficult to identify and treat, the disease can have a protracted and even chronic course with gradual destruction of the joints. In adults, the cause of such arthritis is genital infections, in children - chlamydial pneumonia.
Toxic-allergic arthritis
Toxic-allergic arthritis
This form of the disease occurs with prolonged repeated exposure to the body of toxins released by an infection or formed during a long-term metabolic disorder due to an infection. Examples of such damage can be toxic-allergic inflammatory processes in tuberculosis (Poncet tuberculous arthritis), gonorrhea and sepsis.
Ponce's tuberculous arthritis is quite rare and develops when tuberculosis occurs unnoticed. In contrast to infectious tuberculous arthritis with damage to the joints by the tuberculosis bacillus, the toxic-allergic process develops with prolonged intoxication of the body and exposure of the joints to toxins. The inflammatory process in the joints (often in the knee and elbow) is sometimes benign in nature and goes away during treatment and the development of remission of tuberculosis. But in some cases it has a course similar to rheumatoid arthritis: small joints of the hands are affected, followed by their destruction, change in shape and dysfunction.
Gonorrheal arthritis can also be purely infectious and toxic-allergic. In the latter case, 2-3 large joints are affected (almost always the knee), the disease is acute and, with properly prescribed treatment, ends in complete recovery. If left untreated, the process can become chronic with gradual loss of joint function.
With the generalization of an inflammatory nonspecific infectious process (sepsis), joint damage can be infectious (bacterial-metastatic) and toxic-allergic in nature. In the latter case, acute polyarthritis develops with migrating (moving) joint damage, which after treatment ends in complete recovery.
Chondroprotectors: what are they, how to choose, how effective are they?
Joint pain at rest
Rheumatoid allergic arthritis
This clinical form is classified as an autoimmune disease, however, allergies in this case play an important role. Predisposition to the disease (including allergic processes) is inherited. First, an allergy to a previous infection develops, and then an allergy to the patient’s own tissues develops (autoimmune inflammatory process).
Rheumatoid arthritis affects the small joints of the hands and feet with an initially chronic course of inflammation and its slow progression. Gradually, the destruction of the joints occurs, their deformation and complete loss of function.
Arthritis requires timely treatment, which is why it is so important to consult a doctor at the first signs of the disease.
Children's arthritis. Causes, treatment, prevention.
The first symptoms of a health problem are pain and swelling in the knee. Their causes are bacteria, viruses, genetic and autoimmune diseases. In this case, the body temperature may not increase. Therefore, parents often do not pay attention to complaints and are in no hurry to take their child to the doctor.
However, advanced stages of the disease are more difficult to diagnose, and the prognosis becomes less favorable.
Types of arthritis
There are several types of childhood arthritis:
- Arthritis of the hip joint.
Caused by viruses, bacteria, fungus, parasites. In rare cases, this condition is caused by Lyme disease. The infection enters the joint cavity along with blood and lymph. This usually occurs after an injury. Treatment should be started immediately. Otherwise, the little patient’s condition will rapidly deteriorate.
- Ankylosing spondylitis.
Or juvenile ankylosing spondylitis. This is a chronic disease that affects the sacroiliac joints, spinal joints and paravertebral soft tissues. This disease is characterized by complaints of pain in the back and lower back, as well as stiffness of movement. However, the same disease can also affect the joints. Mainly elbows, knees and ankles.
- Juvenile rheumatoid form
This is a chronic disease that affects the joints. Develops in children under 16 years of age. When it appears, an inflammatory process is observed, and the disease itself progresses quickly and, if it starts, can affect not only the joints, but also spread to the internal organs. As a result, this disease takes on a systemic form.
- Reactive arthritis.
Appears after extra-articular infectious diseases. Reactive arthritis is an inflammation, the focus of which is located in the bone joints. The disease can be either postenterocolitic, that is, occur after an intestinal infection, or urogenital, that is, sexually transmitted.
- Rheumatoid arthritis.
Develops after an infection, such as a sore throat or pharyngitis. At the onset of the disease, a high temperature is noted, as well as symptoms of intoxication - weakness, headache, chills. At the first signs of illness, the child should be immediately taken to the doctor and treatment should begin as soon as possible.
Causes of arthritis in children
There are several reasons for the appearance of this disease in a child. This:
- Osteomyelitis.
A purulent-necrotic process that occurs in the bones, bone marrow and surrounding soft tissues. Osteomyelitis is caused by pyogenic bacteria and microbacteria. They enter the body in two ways: through the bloodstream and after injury.
- Osteosarcoma.
A tumor arising from bone tissue. This pathology is extremely rare. It is characterized by an aggressive course and extremely rapid growth. Its cells can produce bone tissue, but it does not calcify, that is, it does not harden. With this disease, the bones of the lower jaw and pelvis are affected, and in rare cases the spine is affected. Osteosarcoma typically affects older people, but cases have been reported in children.
- Vegetovascular disorders.
This disorder is accompanied by pain in all joints.
- Degenerative changes.
Degenerative changes in the musculoskeletal system (MSA) appear as a result of increased physical activity and during heavy sports, for example, weightlifting.
- Hemophilia.
This is a hereditary blood disease that disrupts the blood clotting factor. With this pathology, hemorrhage into the joint cavity is observed.
- Bacterial.
The causative agents of arthritis are streptococci, staphylococci and tuberculosis. Streptococcal infection is the causative agent of rheumatism.
- Autoimmune arthritis.
Caused by disruption of the cells of the immune system. This type of pathogen provokes infection with juvenile rheumatoid arthritis.
- Viral.
Viruses cause reactive arthritis. These include all types of herpes, rubella, enteroviruses, measles, hepatitis and influenza. The disease can go into an acute phase and become more complicated after the illness.
treatment of arthritis in children
To determine the type of disease, a number of studies are carried out. Diagnostics includes biochemical and serological studies. In addition, doctors determine the tolerability of certain medications.
To treat childhood arthritis, complex therapy is carried out, divided into several stages. It includes both modern and conservative methods.
For relapses and acute phases, a gentle motor regimen is indicated. Wearing bondages is also recommended. In acute cases, fixation with plaster or orthosis.
Drug therapy uses antibiotics and muscle relaxants, as well as non-steroidal anti-inflammatory drugs. In addition to them, doctors also use glucocorticosteroids and immunosuppressive therapy.
Massage and physiotherapy (magnetic therapy, laser therapy, ultraviolet irradiation, UHF therapy, ultrasound) are recommended as auxiliary means. For acute conditions, painkillers creams and ointments are used.
In case of deterioration, surgical operations are resorted to.
Prevention of arthritis in children
The most reliable prevention of arthritis is complete and timely treatment of infectious diseases.
You cannot leave a child untreated just because his condition has improved. Rheumatologists also recommend strengthening the child’s immunity by hardening and using complexes of vitamins and microelements. Author: K.M.N., Academician of the Russian Academy of Medical Sciences M.A. Bobyr
Localization
The inflammatory process most often develops in large joints - the hip and knee.
Allergic arthritis of the hip joint
Allergic arthritis of the hip joint in children and adults appears after severe hypothermia and as a reaction to certain medications. It can occur in a purulent or reactive aseptic form with severe symptoms: high fever, sharp and acute pain, hyperemia.
To exclude the development of sepsis, you should consult a doctor after the first symptoms appear. Inflammation is eliminated with a comprehensive course of medications; in difficult cases, surgical intervention is indicated.
Allergic arthritis of the knee joint
The main symptoms of allergic knee arthritis are swelling, redness and pain in the knee area. Consult a doctor immediately; in the early stages, inflammation responds well to treatment without causing complications or becoming chronic.
Diagnostics
In order to prescribe adequate treatment, it is necessary to establish the correct diagnosis and, if possible, find out the cause of the allergy. For this purpose, the following studies are prescribed:
- Laboratory:
- general clinical
- a general blood test reveals signs of inflammation; - biochemical
– metabolic disorders and signs of inflammation are detected (high levels of C-reactive protein); - immunological
– detection of antibodies to certain allergens, including those of infectious origin; They also determine the presence of rheumatoid factor – autoantibodies to the body’s own tissues; - microbiological
– inoculation of biological media (blood, joint fluid) on nutrient media in order to detect infection and its sensitivity to antibiotics. - Instrumental studies of joints:
- Ultrasound
– reveals signs of inflammation; - radiography
- possible changes in bone structures; - arthroscopy
– performed according to indications; this is an examination of the inner surface of the joint with the possible collection of synovial fluid for examination; helps to distinguish an infectious process from a toxic-allergic one.
It is impossible to diagnose and properly treat allergic arthritis at home. This can only be done in a clinic equipped with modern equipment.
Difficulty of diagnosis
It lies in the fact that the general symptoms are very similar to those of other types of arthritis. And at an appointment with a rheumatologist at our clinic, many patients and their parents forget to say that shortly before they suffered an infectious disease or had an allergy. Therefore, the primary task of our specialists is to find out a complete and accurate picture of the diseases that the child has been suffering from for 1-2 months in order to prescribe the correct tests and carry out treatment.
The main diagnostic methods are:
- Visual inspection of the affected joint.
- Blood and urine analysis. The disease is determined by leukocytes, antibodies to urogenital infections, the number of which exceeds the norm.
- Stool analysis is necessary to identify/exclude infections in the intestines.
- In some cases, an analysis of synovial fluid and a biopsy of the synovial membrane of the joint are prescribed.
- To confirm the diagnosis, the doctor may prescribe an X-ray examination or magnetic resonance imaging.
Treatment of allergic arthritis
After identifying the causes of the disease, treatment is prescribed, including:
- eliminating the entry of the allergen into the body that caused the disease;
- if an infectious-inflammatory process is suspected, identification of the infectious agent and its complete removal from the body;
- suppression of an allergic reaction;
- elimination of the inflammatory process;
- prevention of chronic disease.
Treatment of allergic arthritis is comprehensive and individually selected
Drug therapy
The following groups of drugs are prescribed:
- Anti-inflammatory drugs
- prescribed orally or intramuscularly, as well as externally (Voltaren, Fastum-gel). Popular 1st generation NSAIDs (Diclofenac, Ibuprofen) perfectly relieve inflammation, but have a negative effect on the stomach. The latest generation NSAIDs (Nise, Movalis) act more mildly and have almost no side effects. Children are more often prescribed Paracetamol, which does not give side effects. - Glucocorticoid hormones
are prescribed for severe joint swelling and severe pain. They quickly relieve these symptoms, but have many side effects, so they are prescribed in short courses orally, intramuscularly or as intra-articular injections. - Antihistamines
are prescribed to suppress the secretion of histamine, which supports inflammation. Drugs in this group include Suprastin, Tavegil - they also promote sleep, so they are prescribed at night. The latest generation drugs (Claritin, Erius) do not cause drowsiness and can be taken during the day. - Antibiotics
are prescribed based on the results of laboratory tests to determine the sensitivity of the identified infection to them. - A course of antirheumatic basic drugs
- when there is a risk of chronic arthritis (Metatrexate, Sulfasalazine) or combines their administration with a group of biological agents (MabThera, Enbrel, etc.). This contributes to long-term suppression of inflammation and prevention of relapses.
If toxic-allergic inflammation of the joints is detected, treatment is prescribed for the underlying disease that caused the complication. Sanitation (improvement) of identified foci of infection is also carried out - carious teeth, chronic diseases of the ENT organs, etc.
Drugs for the treatment of allergic arthritis
Non-drug treatments
At different stages of the disease, the following therapeutic measures are prescribed:
- Physiotherapeutic procedures - electrophoresis with hydrocortisone, UHF, paraffin or ozokerite, magnetic or laser therapy.
- Therapeutic massage is prescribed after eliminating severe symptoms of inflammation to improve blood circulation and metabolism, prevent chronicity of the process and muscle atrophy.
- Therapeutic exercises – prescribed depending on the activity of the inflammatory process to accelerate recovery processes in the joints and muscle strength.
- Reflexology (RT) is an effect on active points on the surface of the body, reflexively associated with joint tissues. Inflammation and pain are eliminated, tissue restoration is stimulated.
Crunching in joints - when to worry
Intra-articular injections of hyaluronic acid
Traditional methods
Experts resort to traditional methods quite often in order to reduce the drug burden on the patient. But it is not recommended to use these remedies on your own: without a doctor’s prescription, this can aggravate the course of the disease. Popular folk remedies include:
- saline applications
- carried out with a hypertonic salt solution (a heaped teaspoon of salt per 100 ml of water - approximately a 9% solution is obtained); moisten a napkin with saline solution, wring it out lightly and bandage it to the affected joint; the application can be left for 1 – 3 hours; perfectly eliminate swelling and pain; - ointment from poplar buds
– grind dried poplar buds, grind into powder and combine with an equal volume of butter; store in the refrigerator and use as a rub overnight; relieves unpleasant symptoms well.
How allergic arthritis is treated at the Paramita clinic
Our specialists treat each patient with allergic arthritis very carefully. He is carefully examined to exclude other clinical forms of the disease and to establish the presence or absence of degenerative changes in the joint. Only after this is treatment prescribed, including:
- methods based on the achievements of modern medicine, developed in leading clinics around the world; the latest medications and non-drug treatment methods are used;
- traditional oriental techniques that came to us from China and Tibet; they have been successfully used for centuries to treat various types of allergies; These techniques are based on restoring the patient’s energy potential, which leads to stimulation of the patient’s vitality, normalization of the function of the immune system and elimination of foci of inflammation.
This approach to treating the disease allows us to completely eliminate the threat of chronic inflammation and joint destruction. But even in advanced stages of the disease, we can stop the progression of the disease. Contact us!
We combine proven techniques of the East and innovative methods of Western medicine.
Read more about our unique method of treating arthritis
Recommendations for those who have been ill
Allergic and infectious-allergic arthritis usually ends in complete recovery. But there is always a risk of relapse upon repeated contact with the allergen that caused the disease. Therefore, it is recommended for a recovering person to:
- avoid contact with allergens;
- follow a hypoallergenic diet, excluding from the diet foods that have an allergenic effect: honey, nuts, chocolate, eggs, as well as sweets and baked goods;
- do therapeutic exercises, swimming and feasible sports, move more;
- eliminate heavy physical activity, monitor your weight, avoiding its excessive increase;
- promptly treat all acute diseases and sanitize foci of infection.
Prevention of allergic arthritis
This should be especially taken care of by persons suffering from allergic diseases (atopic dermatitis, bronchial asthma) or a tendency to develop allergic reactions (urticaria, Quincke's edema, anaphylactic shock). Prevention should include: a hypoallergenic diet, elimination of exposure to allergens and timely treatment of all acute and chronic diseases.
Frequently asked questions about the disease
Allergic arthritis is dangerous because it can be complicated by severe allergic reactions or give rise to the development of an autoimmune progressive disease with loss of ability to work. This is why timely treatment of allergic arthritis is so important. All this can be treated, specialists in Moscow are waiting for their patients!
Is it possible to get disability?
Allergic arthritis rarely leads to disability. The exception is rheumatoid arthritis, which is often a cause of disability.
Who should I contact with this disease?
See a rheumatologist. You will also need to consult an allergist.
What is the prognosis of the disease?
Favorable. Most patients make a complete recovery. If left untreated, the process sometimes becomes chronic, in which case joint dysfunction may occur. But even with rheumatoid arthritis, it is possible to stop the progression of the disease.
Bibliography:
- Alieva D.M., Akbarov S.V. Clinical variants of reactive arthritis in children. Scientific and practical rheumatology, 2001, No. 4, p. 74-79.
- Rheumatology. Clinical recommendations, ed. E.L. Nasonova, M., 2005, p. 86-90.
- JT, Petty RE Textbook of Pediatric Rheumatology. Noronto, W. B. Saunders Company 2001; 819.
- Kingsly G., Sieper J. Third International Workshop on Reactive Arthritis: an overview. Ann Rheum Dis 1996; 55: 564-570.
Themes
Arthritis, Joints, Pain, Treatment without surgery Date of publication: 02/25/2021 Date of update: 04/03/2021
Reader rating
Rating: 5 / 5 (1)
Reactive arthritis in children
About the article
25784
0
Regular issues of "RMZh" No. 5 dated March 18, 2006 p. 381
Category: General articles
Authors: Tvorogova T.M. , Korovina N.A. , Gavryushova L.P.
For quotation:
Tvorogova T.M., Korovina N.A., Gavryushova L.P. Reactive arthritis in children. RMJ. 2006;5:381.
Inflammatory joint diseases are one of the pressing problems of modern pediatric rheumatology. Among them, for many years, the leading role belonged to juvenile rheumatoid arthritis (JRA). However, in recent years there has been a tendency towards an increase in reactive arthritis (ReA) in children. The frequency of ReA in the structure of rheumatic diseases in various countries of the world ranges from 8 to 41% [1].
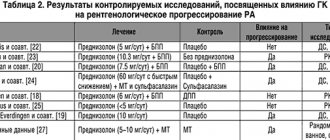
In Russia, among rheumatic diseases, ReA in children under 14 years of age is 56%, in adolescents 37% [2]. The data presented indicate the importance of ReA in childhood and dictate the need for a differentiated diagnostic and therapeutic approach to various variants of this joint pathology in children. Reactive arthritis is an aseptic (non-purulent) joint disease that develops in response to an extra-articular infection in which the causative agent cannot be isolated from the joint. The term “reactive arthritis” was proposed by Finnish researchers Ahvonen et al. in 1969, who first described arthritis that developed after yersinia infection. Subsequently, “reactive arthritis” completely replaced the one proposed by A.I. Nesterov in 1959 coined the term “infectious-allergic arthritis”. Previously, it was believed that ReA was “sterile”, since neither the living causative agent nor its antigens could be isolated from the joint cavity. Subsequently, as methodological techniques improved, individual microbial antigens and even microorganisms themselves capable of reproduction were isolated from joint tissues and synovial fluid [2]. During our long-term observations of children with ReA, we were repeatedly able to isolate chlamydial DNA from the synovial fluid, and in one case, E. coli. In this regard, there are indications in the literature that the term “reactive arthritis” should be used with caution [2,3,4]. However, it is still widespread both in the literature and in international classifications of rheumatic diseases. In the working classification of rheumatic diseases of 1985, three groups of ReA were distinguished: • post-enterocolitic • urogenital • after nasopharyngeal infection At the IV International Workshop on Reactive Arthritis (Berlin, 1999), an agreement was reached on the definition of reactive arthritis. It is recommended to call inflammatory (non-purulent) joint diseases that develop shortly (usually no later than 4 weeks) after an acute intestinal or urogenital infection as reactive arthritis. The etiological factors of postenterocolitic ReA should be considered Yersinia, Salmonella, Shigella, Helicobacter; urogenic - chlamydia, ureaplasma. Other forms of arthritis - post-streptococcal, post-viral, Lyme arthritis, according to the conclusion of the experts of the International Meeting, should be combined with the term “arthritis associated with infection”, and this group should not include septic, purulent arthritis. However, a number of issues require further study. In particular, the list of microbial agents that initiate ReA remains incomplete. Possibly, mycoplasma, clostridia and other infectious agents have a trigger effect [4]. Based on the above, it follows that the infectious agent is the leading one in the development of ReA. The immune response is manifested by the production of antibodies circulating in the blood and synovial fluid. A long-lasting elevated level of antibodies indicates the presence of an infectious agent, on the one hand, and the persistence of microbial antigens in tissues and synovial fluid, on the other. In addition, numerous literature data indicate the importance of genetic predisposition [2,4,5,6,7]. The authors note a close relationship between ReA and one of the antigens of the major histocompatibility complex – HLA-B27. Moreover, the association of HLA-B27 with urogenic arthritis is observed in 80-90% of cases, with postenterocolitic arthritis - in 56%. At the same time, the role of HLA-B27 in the development of ReA has not been fully studied. There are only a few hypotheses: – HLA-B27, being a receptor for microbes, promotes their spread in the body, including in the joint cavity; – HLA-B27, participating in cellular immune reactions, is able to present microbial cells to cytotoxic T lymphocytes. In this case, an inadequate immune response and persistence of the microbe are possible. – in recent years there have been many supporters of the theory of microbial mimicry, when there are similar proteins (antigenic determinants) in a microbe and HLA-B27. In this case, the immune response is directed both against the infectious agent and the tissue’s own cells, having a damaging effect on them. Cross-reacting antibodies weaken the immune response against the infectious agent, which prevents complete elimination and contributes to its persistence [1,8]. A common clinical feature of ReA is a previous infection. By the time arthritis develops, clinical signs of infection usually subside. A mild, asymptomatic course of urogenital infections is possible. In some cases, arthritis develops simultaneously with diarrhea, urinary tract infection, and eye damage (conjunctivitis, iritis, iridocyclitis). At the onset of articular syndrome, low-grade fever, weakness, and loss of appetite are often noted. Clinical features of ReA include: • acute nature of the articular syndrome • asymmetry of the articular syndrome • oligo- or monoarthritis of medium and large joints of the lower extremities • the possibility of a torpid course of the articular syndrome Diagnostic criteria adopted at the International Meeting of Rheumatologists (1995) help in making a diagnosis ( Table 1). Postenterocolitic ReA is characterized by an acute onset with a typical localization - in the joints of the lower extremities. However, sometimes the wrist joints may be involved in the process. In this case, general reactions are expressed in the form of fever (380-390), leukocytosis, acceleration of ESR to 40-45 mm/hour. For this variant of ReA, a torpid course of the articular syndrome is typical, averaging 3-5 months. In some cases, transformation into JRA is possible. Urogenic ReA is characterized by a torpid course combined with high laboratory activity. One of the variants of ReA is Reiter's syndrome (according to ICD-10 M02.3 - Reiter's disease). The disease develops in temporary connection with intestinal or urogenital infections. Currently, Reiter's syndrome is considered to be a consequence of chlamydial infection. At the same time, Chlamydia pneumoniae is detected in 90% of children, and Chlamydia trachomatis is detected in only 10% [10]. The clinical picture is characterized by the presence of urethro-oculo-synovial syndrome. In children, damage to the urogenital tract is manifested by leukocyturia, dysuria, symptoms of vulvitis or vulvovaginitis in girls, balanitis or balanoposthitis in boys. Under our observation, among the patients with Reiter's syndrome, there were three boys aged 12-14 years, in whom balanitis occurred with bright confluent erosions with scalloped edges. Eye damage in the form of conjunctivitis is short-lived and ephemeral, but it may recur. Literary data indicate the possibility of developing iridocyclitis and uveitis [3,5,11]. Articular syndrome in the form of acute asymmetric arthritis occurs with the accumulation of a large amount of synovial fluid (up to 50-70 ml in the knee joints), involving large and small joints of the lower extremities. Damage to the first toe with the formation of a “sausage-shaped” deformity is quite common. The “staircase symptom” is characteristic, in which there is a gradual involvement of the joints from bottom to top. Periarticular lesions in the form of bursitis, tendovaginitis, enthesitis and enthesopathies are typical. The classic triad of symptoms may be joined by skin lesions in the form of keratoderma of the palms and feet, psoriasis-like plaques on the skin of the face, trunk, and limbs. With a prolonged course, onychodystrophy develops (change in nail color, fragility, roughness, tuberosity), which is often regarded as a mycotic lesion. The duration of Reiter's syndrome in an acute course is 2-3 months; in a prolonged course, transformation into JRA is possible. Reactive arthritis is classified as a seronegative spondyloarthropathy. This is explained by the identical clinical symptoms of ReA and the onset of spondyloarthropathy. The latter manifest in childhood and adolescence with reactive asymmetric oligoarthritis of the lower extremities, which is combined with enthesitis. Damage to the hip joints deserves special attention. In 1/3 of children and adolescents, arthritis of the hip joints is the first symptom of spondyloarthropathy. At the onset, other joints are affected only in 10-15% of patients [4,12,15]. Damage to the sacroiliac joints significantly increases the likelihood of spondyloarthropathies. Specific clinical signs that have occurred in the past or are detected at the time of observation allow one to suspect the onset of spondyloarthropathy in children with clinical signs of ReA. These include: • pain in the gluteal muscles (constant or intermittent); • pain in the sacrum or morning stiffness in the lumbar region; • pain in the heel, sole or other enthesopathy; • the presence of a “sausage-shaped” finger on a hand or foot; • diarrhea, dysuria a month before the onset of arthritis. Timely specific nosological diagnosis of spondyloarthropathy in children is possible only through dynamic observation, laboratory and radiation diagnostics. Examination of children with ReA includes: 1. Family history with an emphasis on diseases of the musculoskeletal system, metabolic disorders. 2. Epidemiological history. 3. Clinical blood test. 4. General urine analysis. 5. Biochemical blood test (CRP, protein fractions, fibrinogen, uric acid, kidney and liver function indicators). 6. To identify the infectious agent: – microbiological examination of feces, synovial fluid, scrapings from the conjunctiva, external genitalia; – immunological methods to detect antibodies to antigens of enterobacteria and intracellular pathogens in synovial fluid and blood serum; – study in urine, in the epithelium of the urogenital tract, synovial fluid of DNA and RNA of chlamydia, ureaplasma using polymerase chain reaction; – seeding of synovial fluid, genital secretions onto cellular structures (the cultural method is the “gold standard” for clarifying the trigger role of chlamydia in joint pathology). 7. X-ray examination of joints, spine, sacroiliac joints (according to indications). 8. Electrocardiography (according to indications). When carrying out a differential diagnosis, the following are excluded: – acute rheumatic fever; – infectious arthritis (septic); – other diseases from the category of spondyloarthropathy (juvenile spondyloarthritis, onset of ankylosing spondylitis, etc.); – seronegative JRA; – metabolic arthritis; – synovitis against the background of joint hypermobility syndrome; – other inflammatory diseases of the joints. The goal of treatment for ReA in children is to eliminate the causative factor - the infectious agent, as well as cure or achieve stable clinical and laboratory remission of the articular syndrome. All children with ReA receive drug therapy taking into account age, individual effectiveness, the appropriate trigger agent, as well as the severity and nature of the articular syndrome. 1. Antibacterial therapy is prescribed when an infection is detected. This applies primarily to chlamydial, myco- and uroplasma infections, as well as Helicobacter pylori. The drugs of choice are new generation macrolides that accumulate intracellularly in inflamed tissues (Table 2). It should be noted that with increasing duration of one course of antibacterial therapy, the effectiveness of treatment does not increase [10]. If articular syndrome persists, it is possible to prescribe a second course of antibiotics using one of the above drugs. In this case, the interval between the first and second courses should be at least 5-7 days. It must be remembered that penicillin drugs are not indicated for chlamydial infection due to their transformation into L-forms, which are insensitive to antibiotics. In addition, immunocompetent cells (phagocytes, T-cells) practically do not react to L-forms, which contributes to the persistence of the pathogen and the chronicity of the articular syndrome. According to our observations, a combination of antibacterial therapy with one of the immunocorrective drugs - lycopid, which stimulates the functional activity of phagocytes and increases the synthesis of specific antibodies, is justified. For children aged 1.5 to 15 years, licopid was prescribed at a dose of 1 mg/day. The duration of the course was no more than 15 days. The start of therapy with licopid preceded the prescription of a macrolide (5 days - licopid, then 10 days - macrolide + licopid). In the case of chronic articular syndrome, immunocorrective therapy requires great caution, since the development of an immunoaggressive stage of the inflammatory process cannot be excluded. In postenterocolitic ReA, antibacterial therapy is usually ineffective [16]. 2. Non-steroidal anti-inflammatory drugs (NSAIDs). This class of pharmacological agents is a necessary component of the treatment of ReA. NSAIDs quickly reduce pain and reduce the intensity of the inflammatory process by suppressing the activity of the enzyme cyclooxygenase (COX), which is involved in the synthesis of prostaglandins. In the last decade, the understanding of the points of application of NSAIDs in the regulation of prostaglandin synthesis has expanded significantly. Two isoforms of COX have been discovered: COX-1 and COX-2, which play different roles in this regulation. It is COX-2 that takes part in the synthesis of pro-inflammatory prostaglandins, which enhance the processes of inflammation and cell proliferation. The activity of COX-1 determines the production of prostaglandins, which are responsible for normal physiological cellular reactions not associated with inflammation [13]. NSAIDs, acting on both isoforms of COX, reduce the activity of the inflammatory process and at the same time can lead to undesirable reactions from various organs and systems. Currently, NSAIDs that can selectively inhibit COX-2 (meloxicam, nimesulide) have been developed and are widely used. The main NSAIDs used in the treatment of ReA in children are shown in Table 3. From the data in this table it follows that NSAID therapy has age restrictions. The drugs of choice for children under 5 years of age are paracetamol and ibuprofen. However, the minimum effective therapeutic dose of ibuprofen is lower than paracetamol, which significantly reduces the risk of possible adverse reactions. Ibuprofen blocks COX both in the central nervous system and at the site of inflammation, which causes a distinct anti-inflammatory effect. The analgesic effect of the drug is also double (central and peripheral), and therefore it is more pronounced than that of paracetamol [14]. The drug does not form toxic metabolites, is well tolerated and can even be prescribed to infants. 3. Local therapy for ReA includes intra-articular administration of glucocorticosteroids (GC) and local use of NSAIDs in the form of ointments, creams, and gels. Intra-articular administration of HA has a distinct anti-inflammatory and analgesic effect. In combination with the above therapy, as a rule, 1-3 injections are sufficient to relieve articular syndrome. The use of ointment forms of NSAIDs, especially in children of the first years of life, is safer and allows you to reduce the dose of orally taken drugs. Gels are preferred, since the alcohol solution present in their composition contributes to the fastest transcutaneous effect. In this case, NSAIDs suppress the production of inflammatory mediators directly in the tissues surrounding the joint. 4. If ReA is torpid or the process is chronic, sulfasalazine is indicated in a daily dose of 20-30 mg/kg, but not more than 1.5-2 g per day. The initial dose is 125-250 mg per day, the dose is increased to the calculated dose gradually, once every 5-7 days. The clinical effect occurs after 5-6 weeks of treatment. The duration of the course is individual, but not less than 2 months. Thus, when carrying out complex therapy for ReA in children, one should take into account the biological characteristics of the infectious agent, evaluate the nature of its interaction with the macroorganism, and synchronize treatment with the activity and nature of the course, severity, and dynamics of the inflammatory process in the joints. References 1. Cassidy. JT, Petty RE Textbook of Pediatric Rheumatology. Noronto, W. B. Saunders Company 2001; 819. 2. Alekseeva E.I., Zholobova E.S. Reactive arthritis in children. Questions of modern pediatrics, 2003, vol. 2, No. 1, p. 51-56. 3. Guide to internal medicine. Rheumatic diseases, ed. V.A. Naso-nova, N.V. Bunchuk, M. 1997, p. 305-335. 4. Agababova E. R. Some unclear and unresolved issues of seronegative spondyloarthropathies. Scientific and practical rheumatology, 2001, No. 4, p. 10-17. 5. Agababova E. R. Reactive arthritis and Reiter’s syndrome. Rheumatology, 1997, chapter 11, p. 324-331. 6. Alieva D.M., Akbarov S.V. Clinical variants of reactive arthritis in children. Scientific and practical rheumatology, 2001, No. 4, p. 74-79. 7. Zholobova E.S., Chistyakova E.G., Isaeva K.S. Hereditary and infectious factors in the development of juvenile chronic arthritis. Abstracts of the All-Russian Congress “Pediatric Cardiology 2002”, M. 2002; 227. 8. Ikeda V., Yu DT The pathogenesis of HLA B27 arthritis: the role of HLA B27 in bacterial defense. Am J Ved Sci 1998; 316:257. 9. Kingsly G., Sieper J. Third International Workshop on Reactive Arthritis: an overview. Ann Rheum Dis 1996; 55: 564-570. 10. Chistyakova E.G. Chronic joint diseases in children (juvenile rheumatoid arthritis, Reiter's disease, juvenile chronic arthritis) associated with chlamydial infection. features of the clinic and course. Author's abstract. diss. ... Ph.D. Med. Sciences, M. 1998. 11. Molochkov V.A. Reuters Consilium Medicum 2004, v. 6, No. 3, p. 200-202. 12. Drezenko A.A. The possibilities of local therapy for spondylitis. RMG, 2005, t. 13, No. 24, p. 1632-1636. 13. Nasonov E.L. Non -steroidal anti -inflammatory prepes. RMG, 1999, No. 8, p. 392-396. 14. Autret E., et al. Evaluation of Ibuprofen Versus Aspirin and Paracetamol on Efficacy and Comfort in Children with Father. EUR J Clin 1997; 51: 367-71. 15. Agababova E. R. Modern areas of research with spondyl arthropes. Act speech. The first All -Russian Congress of Rheumatologists. Saratov, 2003. 16. Rheumatology. Clinical recommendations, ed. E.L. Nasonova, M., 2005, p. 86-90.
Content is licensed under a Creative Commons Attribution 4.0 International License.
Share the article on social networks
Recommend the article to your colleagues