Ultrasound of the shoulder joint is a technique for diagnosing pathology of the shoulder joint using ultrasonic waves. The study is carried out in real time - the image is immediately displayed on the monitor. Ultrasound images visualize fiber, cartilage, ligamentous-muscular apparatus and other structures.
Using ultrasound, pathologies are detected in the early stages: traumatic injury, arthrosis, inflammation, tumors. Doctors can give a referral for research: therapist, pediatrician, surgeon, orthopedist, rheumatologist.
Who is indicated for ultrasound of the shoulder joint?
In most cases, the following factors are direct indications for diagnosis:
- Injury to the shoulder area;
- History of musculoskeletal diseases;
- Pain in the shoulder area;
- Restricted mobility of the shoulder joint;
- Swelling of the area;
- Upcoming joint surgery.
In addition, diagnostics is used to assess the dynamics of treatment.
The shoulder joint has a complex anatomical structure, so its diagnosis must be carried out by competent specialists using high-quality equipment. Contact only trusted medical centers to get the most reliable information.
Differences and common principles of operation
The difference between ultrasound and MRI lies in the differences in the principles of their effects. In the first case, the ability of high-frequency sound waves to penetrate through body tissues and be reflected from them is used. Magnetic resonance imaging is based on the creation of resonance by a magnetic field.
The resulting image in the scale required for study is transmitted to the monitor screen during the examination using both methods.
Make an appointment now!
Who should not have an ultrasound?
Anyone can take the study, regardless of age and other characteristics. This procedure is completely painless, does not cause discomfort and has no negative effect on the body. However, if the patient experiences limited joint motion, this can complicate the diagnosis. Before manipulation, make sure that there is no allergic reaction to the silicone that is included in the gel for ultrasound examination.
If there are fresh burns or severe injuries in the shoulder area, then it is worth postponing the examination until the wounds have healed.
Principle of ultrasound examination
The ultrasound mechanism is based on the same principle as the sonar system used by a bat or used on a ship, submarine, or weather station. When a sound wave collides with an obstacle, an echo is formed when it is reflected. A detailed analysis of the reflected wave evaluates the location of objects, their size, shape and consistency, which can be dense, mixed or liquid.
In medical practice, the use of ultrasound makes it possible to accurately determine changes in an organ, tissue, vessel, and detect pathological formations, for example, malignant or benign tumors.
During an ultrasound examination, sound waves are sent by a transducer and received back as reflected vibrations. The received data is recorded by the device and converted for visualization in the form of images. When the doctor presses the sensor on the shoulder, small pulses of inaudible, high-frequency sound waves are generated that penetrate the patient's body. The collision of the wave with the joint structures being examined is noted by a sensitive microphone that detects:
- height and direction of sound;
- changes in sound wave parameters.
A computer program measures the values of the resulting characteristic vibrations, which are reflected on the monitor in the form of images. The purpose of ultrasonography is to obtain an image of the movement of joint elements and fluids. Small video fragments are also recorded in real time.
How the research works
Before starting the diagnosis, the patient is asked to sit or lie on a special flat couch. It is necessary to remove clothing above the waist so that the area being examined is completely free. You will also most likely need to remove jewelry from your neck and pull your hair into a ponytail if it is too long.
A small amount of a special product is applied to the skin to improve contact between the sensor and tissues. During the examination, the doctor may ask you to change your body position. During the diagnosis, the doctor also pays attention to the condition of the muscles, tendons and nearby tissues.
The manipulation lasts no more than half an hour. At the end of the study, the patient is given a transcript with a transcript. The interpretation is carried out by the doctor who referred for this procedure.
Procedure
During an ultrasound examination of the shoulder joint, the patient is asked to sit or lie on a couch that can be moved or tilted. A newborn or small child is examined in a lying position in the presence of one of the parents. The skin of the shoulder is lubricated with a special gel to ensure tight contact of the sensor with the skin and eliminate air pockets that serve as an obstacle to the free passage of sound waves through the tissue. The doctor examining the patient begins to press the sensor at the desired point, gradually moving it along the entire shoulder joint. This ensures the penetration of sound waves into structures at a certain angle for targeted examination of the required area with the probable presence of destructive and degenerative damage. What a person may feel during ultrasonography:
- when applying the gel to the skin, you may only experience a feeling of coolness, since the product does not have therapeutic properties;
- when pressing with a sensor, pain of varying severity may appear when affecting the area of the shoulder where an acute or chronic inflammatory process occurs;
- discomfort may occur if the doctor asks the patient to make a movement to assess the pathology in dynamics.
The duration of the ultrasound examination is 20-30 minutes, but if a structure is detected that requires additional examination, the duration of the diagnostic procedure will increase slightly. At the end of the examination, the patient wipes the gel with a napkin and waits for the results to be deciphered. The doctor will analyze the images obtained and draw up a report to present to a rheumatologist, vertebrologist or neurologist.
Unlike other diagnostic procedures, an ultrasound scan of the shoulder joint does not require any preparation. For the examination, the patient only needs to bring with him a referral from the doctor, a sheet or diaper, and a towel for wiping the gel from the skin.
What does an ultrasound of the shoulder joint show?
If you go to a good clinic with high-quality equipment and get an appointment with an experienced specialist with many years of experience, you can identify even minor defects of the shoulder joint or pathological changes in the early stages.
In the absence of pathological processes, normal values vary within the following limits. Lack of fixation of violations of the muscle, cartilage, connective tissue of the joint and its capsule. The width of the brachial nerve reaches 4.6 mm, its length is 2.3 mm, the presence of a small amount of intra-articular fluid in the lateral membrane of the biceps brachii muscle is allowed. Echogenicity is within normal limits, the structure is homogeneous.
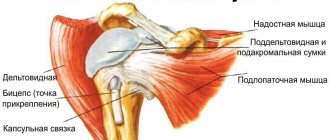
Ultrasonography of rotator cuff injuries
Ultrasound scanner HS60
Professional diagnostic tools.
Assessment of tissue elasticity, advanced 3D/4D/5D scanning capabilities, BI-RADS classifier, options for expert cardiological studies.
Introduction
Pain in the shoulder joint, like pain in the knee joint, is quite common among orthopedic diseases not associated with trauma. Many specific syndromes have been described that can be distinguished with careful history taking and examination. One of them, pain in the anterior shoulder joint, is detected with lateral abduction of the shoulder from 45° to 135°. This distinguishes impingement syndrome from pathology of the rotator cuff and coracoacromial region. Clinically, it is necessary to exclude the pathology of the so-called “frozen” shoulder, in which pain occurs with multidirectional movements in the shoulder joint.
Pathological processes that cause pain in the coracoacromial angle include subacromial-subdeltoid bursitis and tendinopathy of the supraspinatus tendon. Long-term tendonopathy is accompanied by damage to the supraspinatus muscle with the involvement of the tendons of the subscapularis and infraspinatus muscles in the pathological process. One should also not exclude bone changes in the head of the humerus, including enthesopathy of the coracoacromial ligament, a newly formed bone bed for the tendons of the supraspinatus and biceps muscles in the area of the greater tubercle after their traumatic injury. Chronic inflammation of the biceps tendon can lead to tendinopathy or rupture. Sometimes subluxation of the biceps tendon is detected due to rupture of the subscapularis tendon or the transverse ligament of the intertubercular groove of the head of the humerus.
The first studies, published in the mid-1980s, comparing sonographic findings with surgical findings, showed high accuracy (92-94% in series of 51 and 47 patients) [1, 2] for detecting rotator cuff tears. In more recent studies, this accuracy was lower: 60-84% (in series of 38, 10 and 49 patients) [3-5]. In addition, only a few studies have compared the accuracy of sonography with arthroscopy in identifying rotator cuff tears [6–9], and few studies have correlated the size of the rotator cuff tear with surgical findings [6, 9]. In [6], when examining 61 patients, it was found that when diagnosing full-thickness tears, sonography has a sensitivity of 95% and a specificity of 93%. In addition, the accuracy of sonography in predicting the extent of damage for complete rotator cuff tears greater than 4 cm is 89%, for tears of 2-4 cm it is 43%, and for tears less than 2 cm it is 70%. In a study of 225 patients, Wienner and Seitz found that sonography had a sensitivity of 95% and a specificity of 94% for detecting complete tears. For gap size determination, sensitivity and specificity were 91 and 94%, respectively.
The purpose of this study was to compare the diagnostic performance of sonography with that of arthroscopy to determine the degree of accuracy in identifying rotator cuff tears and biceps tendon pathology.
Materials and methods
We examined 100 shoulder joints with pain in 98 patients - 54 women and 44 men, whose ages ranged from 14 to 82 years (average age - 56 years). Standard ultrasonography was performed on patients before surgery, followed by arthroscopy.
In 65 patients, the primary arthroscopic or final clinical diagnosis was a complete rotator cuff tear; 15 patients were diagnosed with an incomplete cuff tear, 12 patients with rotator cuff tendonitis, 4 patients with frozen shoulder, 2 patients with arthrosis of the acromioclavicular joint, 1 patient with a labrum tear, and one patient with calcific bursitis. In 2 patients, complete rupture and incomplete damage were found.
Indications for surgery and arthroscopic examination included pain in the shoulder joint for more than 6 months, failure of conservative treatment, which consisted of physical therapy, the use of non-steroidal anti-inflammatory drugs and at least one corticosteroid injection. For patients with a complete cuff tear, the indication for surgery was intense pain for more than 3 months, despite the above treatment. In patients with grade III rotator cuff injury who were unable to lift their arm or who had a history of recent injury (less than 3 months at the time of examination), surgery was performed early after the injury.
Method of studying the shoulder joint.
All ultrasonograms were acquired in real time on the scanner using a linear variable frequency transducer (5–12 MHz). All patients underwent standard bilateral ultrasonography of the shoulder joints.
When performing sonography, the patient sat in a chair and the examiner stood behind the patient. First, the biceps tendon was examined in a transverse view, starting from the distal end of the acromion to the junction of the tendon and muscle. The probe was then rotated 90° to examine along the tendon. When the upper limb was externally rotated, an image of the subscapularis tendon was obtained; the sensor was located in the transverse plane at the level of the lesser tubercle and shifted to the medial side of the joint.
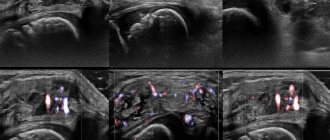
An image of the supraspinatus tendon was obtained with the shoulder extended, the elbow flexed, and the forearm placed on the wing of the ilium. In this position, the supraspinatus tendon is brought out as far as possible from under the acromion. The transducer was oriented parallel to the location of the tendon (approximately 45° between the coronal and sagittal views) to visualize the tendon fibers in the longitudinal view (Fig. 1 a, b), then the transducer was moved from anterior to posterior to visualize the supraspinatus and infraspinatus tendons. To study the tendon in the transverse projection, the sensor was rotated 90° (Fig. 1c-e).
Rice. 1.
Study diagrams and sonograms.
hell)
1 — supraspinatus muscle, 2 — infraspinatus muscle, 3 — with visualization of the biceps tendon.
Ultrasonographic criteria.
Rotator cuff tears can be complete or partial, longitudinal or transverse (Fig. 2). Acute tears have a transverse configuration, while chronic tears are mostly longitudinal and oval or triangular in shape.
Rice. 2.
Sonograms of a complete rotator cuff injury.
A)
Absence of the cuff due to complete avulsion, retraction and displacement under the acromion.
b)
A focal defect formed by varying degrees of contraction of the torn tendon ends.
V)
Hypo- or anechoic inclusions at the site of rotator cuff injury (hematoma).
G)
Anastomosis with an expanded subacromial-subdeltoid bursa, exposed bony contour of the head of the humerus with the deltoid muscle adjacent to it.
d)
Absence of the rotator cuff in the center and hernial protrusion of the deltoid muscle or subacromial-subdeltoid bursa into it.
We considered the following ultrasound criteria for rotator cuff rupture:
- lack of visualization for large tears, when the cuff was torn off from the greater tubercle and retracted under the acromion process. In this case, the deltoid muscle was adjacent to the humeral head, and there was no detectable rotator cuff echo between the deltoid muscle and the head. The diagnostic accuracy of this cuff tear sign was close to 100%;
- an extensive hematoma that fills the space between the head of the humerus and the deltoid muscle. The diagnostic accuracy of this cuff tear sign was close to 100%;
- focal thinning of the rotator cuff as a consequence of the absence of an echo signal as a result of the appearance of direct contact between the muscle and the head of the humerus.
This sign also has high diagnostic significance. Focal thinning in the rotator cuff should be distinguished from thinning of the external rotator cuff tendons as a natural progression of the degenerative process. Degenerative-dystrophic changes in the joints (Milwaukee syndrome) are most often found in elderly women. This manifests as destructive arthropathy due to the accumulation of hydroxyapatite or mixed calcium phosphate crystals. Clinical signs coincide with ultrasound findings, which reveal cartilage changes and bone destruction, subchondral sclerosis, intra-articular tissue damage, rotator cuff tears, and joint deformity. Some authors believe that the initial manifestations of this disease are damage to the rotator cuff, resulting in a high position of the head of the humerus and contact with the acromion and the articular end of the scapula (Fig. 3). Such ruptures can sometimes be asymptomatic.
Rice. 3.
Degenerative-dystrophic changes in joints.
A)
Sonogram shows no rotator cuff, hypoechoic hemorrhages (arrows) and erosion of the articular surface of the humeral head (coronal section of the humerus) (arrowhead).
b)
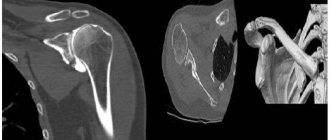
The radiograph shows destruction of the contour of the shoulder joint and extensive subchondral sclerosis; changes in the distal end and chondromatosis of the acromion are determined.
V)
The sonogram shows thickening of the bursa wall (arrowheads) and hypoechoic hemorrhage at the level of the eroded greater tubercle.
The tendons of the supraspinatus and infraspinatus muscles are most often damaged, and less commonly the subscapularis muscle (Fig. 4). Subscapularis tears typically involve displacement of the long head of the biceps tendon.
Rice. 4.
Sonograms of injuries to the supraspinatus, infraspinatus and subscapularis tendons.
A)
Acute rupture of the subscapularis tendon. Axial USG demonstrates a small tendon remnant attached to the lesser tuberosity (arrow).
b)
Dislocation of the biceps tendon. Axial USG shows an empty intertubercular groove (arrow). The biceps tendon is dislocated medially (arrowhead).
V)
Subluxation of the biceps tendon (arrowhead) without injury to the transverse ligament (arrow).
G)
A CT arthrogram of the same patient's shoulder shows proximal subluxation of the biceps tendon (arrow) with an empty intertubercular recess.
A complete rupture of the rotator cuff during longitudinal and transverse scanning is detected in the form of a violation of the integrity of the contours of the cuff.
In case of an incomplete rupture, the rotator cuff flattens on the bursa side (incomplete rupture on the bursa side) or a hypoechoic (or mixed hyper-hypoechoic) defect is clearly visible in the longitudinal and transverse projections on the articular side of the rotator cuff (incomplete rupture on the articular side) (Fig. 5) .
Rice. 5.
Sonograms of partial injury to the supraspinatus tendon.
A)
A small tear with focal loss of the normal convexity of the distal tendon (arrow).
b)
Medium size tear, defect at the distal end of the tendon with flexion into the deltoid muscle defect, the normal convexity of the tendon is altered.
V)
Intrastem injury of the rotator cuff with the formation of a small hematoma.
G)
A hypoechoic stripe runs through the entire thickness of the supraspinatus muscle, indicating partial damage.
d)
Partial damage to the supraspinatus muscle, visible anechoic stripes of damage and uneven contour of the greater tubercle.
e)
A small hypoechoic focus on the articular surface of the tendon (arrow).
and)
T2-weighted coronal image shows a focus of high signal at the distal end of the tendon extending toward the inferior articular surface (arrow), indicating an incomplete rupture of the supraspinatus tendon.
The extent of the rotator cuff tear is determined by transverse measurements. If the tear extends posteriorly from the intra-articular portion of the biceps tendon by 1.5 cm or less, then the condition is assessed as an injury involving only the supraspinatus tendon. If the tear is more than 3 cm, then it is assessed as an injury involving the supraspinatus and infraspinatus tendons. The teres minor tendon is not assessed when determining the extent of injury.
A rupture of the long head of the biceps tendon is reported when the tendon is not identified within or medial to the intertubercular groove (Figure 6). A biceps tendon dislocation is characterized by its displacement anterior or medial to the lesser tubercle of the humerus.
Rice. 6.
Sonograms of damage to the long tendon of the biceps brachii muscle.
A)
With complete damage, in the transverse projection there is no tendon in the intertubercular groove.
b)
With a partial rupture of the biceps tendon, atrophic echogenicity of the long head of the muscle (arrow) is determined on the transverse projection, which indicates damage to the tendon.
V)
Contralateral side of the long head of the muscle.
G)
Damage to the biceps muscle at the junction of the tendon part. An anechoic hematoma is detected in the damaged area (arrow). The tendon part of the muscle is disintegrated (arrowheads), and there is no normal structuring of the muscle.
Ultrasonographic and arthroscopic findings were correlated regarding the presence or absence of complete and incomplete rotator cuff tears, the size and extent of the tear, and the presence of biceps tendon dislocation or rupture. Complete tears were analyzed regarding their size and extent. Two of the 25 shoulders with complete tears were excluded from the analysis because in one case the range of motion was severely limited and the extent of the tear was unclear. In another case, arthroscopic examination was performed 1 year after sonography.
results
Determination of rotator cuff tears.
Ultrasonography accurately identified all 65 complete rotator cuff tears that were diagnosed at arthroscopy. No false negative results were identified. Complete rotator cuff tears were misinterpreted in three shoulders that had incomplete tears at arthroscopy; one of these tears was large (more than 50% of the cuff thickness) and involved the entire supraspinatus tendon.
Seven of 15 incomplete rotator cuff tears that were diagnosed arthroscopically were correctly identified. In three shoulders, complete tears were identified instead of incomplete tears. 5 false negative results were identified. In two of these joints, ultrasonographic imaging of the rotator cuff was limited by range of motion, and in three cases, arthroscopy showed only moderate thinning of the supraspinatus tendon. There were 3 false positive results. In the first case, a poorly defined hypoechoic area was identified, which appeared to be a partial tear in depth on the capsular side of the cuff near its insertion. Another false-positive case had slight flattening of the supraspinatus tendon on the side of the subacromial bursa. Sonography correctly diagnosed the absence of a tear in 17 of 20 shoulder joints, which was confirmed arthroscopically.
In three cases, ultrasonography revealed a complete tear, but arthroscopy revealed an incomplete tear. In 3 patients, an incomplete tear was noted sonographically, but the cuff was normal at arthroscopy.
Dimensions and length of ruptures.
Of the 63 complete rotator cuff tears analyzed using these parameters, arthroscopic examination revealed involvement of the supraspinatus tendon in the pathological process in 26 cases. The tears were less than 1.5 cm in width, and in 37 joints, the damage involved the supraspinatus and infraspinatus tendons. The size of the rupture was more than 1.5 cm. Only in 7 joints was a rupture of the subscapularis tendon detected. Transverse measurements performed with ultrasonography correctly determined the extent of the tear in 21 cases (81%) of 26 shoulders with an isolated rupture of the supraspinatus tendon. In 3 joints, during sonography, the width of the rupture was greater or lesser by 0.5 cm and in 2 cases - by 1.1 and 1.3 cm. In the first two cases, arthroscopy confirmed the presence of not only a complete rupture of the supraspinatus tendon, but also a longitudinal incomplete tear (more than 50% of the cuff thickness) extending to the infraspinatus tendon. However, on sonography this tear was interpreted as a complete rupture.
Transverse measurements performed with ultrasonography correctly identified the extent of the tear in 33 (89%) of 37 shoulders that had a combined rupture of the supraspinatus and infraspinatus tendons. In the remaining 4 shoulders, the extent of the infraspinatus tendon tear was sonographically underestimated by 1.5 cm. In 3 of these cases, arthroscopy showed that the infraspinatus component constituted the middle portion of the tear, medial to the site of the supraspinatus injury. Sonography correctly identified 6 of 7 subscapularis tendon ruptures. Overall, sonography accurately determined the size and extent of tears in 86% of shoulders with complete ruptures.
In 5 cases out of 37, a massive rupture of the supraspinatus tendon with retraction of the damaged tendon under the acromion was detected. During ultrasonographic examination, the proximal end of the injured tendon was not identified.
Dislocation and rupture of the biceps tendon.
Sonography correctly identified 5 of 6 biceps tendon dislocations that were diagnosed arthroscopically. In one case, a false negative result was obtained. This was due to the absence of tendon in the intertubercular groove and the dislocation was interpreted as a rupture. A total of 94 true negative ultrasonograms were obtained. No false positive results were identified.
Sonographic examination correctly identified 7 of 11 biceps tendon ruptures that were diagnosed arthroscopically. 4 false negative results were identified. Two of them showed normal echogenic character of tendon fibers in the intertubercular groove. In total, one false-positive ultrasonogram and 80 true negative ultrasonograms were obtained.
Discussion
The high resolution of ultrasonographic examination of the shoulder joint is not widely used by orthopedic surgeons to diagnose and identify the nature of rotator cuff pathology. This may be due in part to the paucity of ultrasonographic studies of the shoulder compared with magnetic resonance imaging (MRI), the often lack of radiological verification of the data, and the difficulty of recognizing archival sonograms for relevant anatomy and pathological conditions. In addition, some publications have reported wide variations in sensitivity (57-100%) and specificity (50-100%) for sonographic detection of rotator cuff tears in series ranging from 10 to 225 patients, which also reduced confidence in the accuracy of this method [1- 9]. Researchers who have reported poor results in diagnosing rotator cuff tears have used ultrasonographic criteria that are either no longer used or have been improved, and have used older equipment and lower frequency transducers than is currently available [3]. 5, 7].
In this paper, the accuracy of shoulder ultrasonography was re-examined in the context of recent improvements in scanning techniques and improved criteria for diagnosing rotator cuff tendon tears. In contrast to previous studies in which sonographic findings were correlated with arthrography or open surgery, we compared ultrasonographic findings with arthroscopy, which has a number of potential advantages. Enhanced arthroscopic imaging can provide accurate intra-articular visualization, including the rotator cuff tendon, incomplete intratendinous tears, and the presence of intra-articular pathology of the biceps brachii tendon.
We have found that ultrasonography is highly accurate for identifying complete transverse rotator cuff tears and for determining the extent of injury. Sonography gave an incorrect diagnosis of complete rupture in only 3 shoulder joints; on arthroscopic examination, all of them were incomplete; in one case, more than 50% of the cuff substance was involved in the rupture. In our study, the sensitivity was 100% and the specificity was 86%. Our results were close to those reported in previous studies (where sensitivity or specificity, or both, was 95% [8, 9], as well as to data reported in numerous MRI studies [7, 10]. 12].
The use of sonography to determine the size and extent of a tear has been evaluated in [6, 9]. Brenneke and Morgan reported that sonographic studies accurately determined the size of large tears, but decreased accuracy for moderate and small tears [6]. We found that sonographic studies were extremely accurate in determining the extent of tears of any length if measurements were carried out in a transverse projection. Our data confirm the reports of Wienner and Seitz [9]. In two shoulders in which we overestimated the extent of the tear by more than 1 cm, arthroscopic examination revealed a complete tear with a prominent distal tendon component. This distal component was incorrectly interpreted as a complete rupture. In both joints, a local defect was caused by the sensor pressing the deltoid muscle against the rotator cuff. Incomplete tears involving more than 50% of the cuff have a focal defect (this is the criterion used to define a complete tear). This symptom is observed with complete damage, when the deltoid muscle fills the rupture site. Manipulation of the probe increased the sensitivity of sonography for detecting small (without significant distasis) tears, but reduced the specificity of the method. Ultrasonographic studies cannot distinguish large longitudinal incomplete tears from complete ones. In three shoulders in which the extent of the tear was underestimated by ultrasonography, arthroscopic examination revealed a tear of the medial portion of the supraspinatus tendon in the infraspinatus tendon. The component of the midsubstantia tear was not determined when we examined only the lateral rotator cuff near its insertion, indicating the importance of arm position in visualizing the rotator cuff not only at its insertion, but also more medially.
In our studies, the ability to detect incomplete rotator cuff tears using sonography was limited; however, 2 of the 5 shoulders that had false-negative results had reduced range of motion (the patient was unable to externally rotate the arm or extend the shoulder joint to the level of the buttocks), which precluded cuff evaluation. In the third case, the incomplete tear, which was identified arthroscopically, was due to only moderate thinning of the supraspinatus tendon and could not be detected by ultrasonography. Brenner and Morgan also reported low sensitivity of sonography in detecting incomplete tears; in their other two more recent studies, the sensitivity of the method was more than 90% [6, 9].
Biceps tendon pathology is often associated with rotator cuff tendon injuries. In a recent study, the prevalence of biceps tendon rupture was 11% and the prevalence of dislocation was 6%. Anterior or medial dislocation in relation to the lesser tuberosity is easily detected using sonography. 5 of 6 dislocations were correctly diagnosed. On the other hand, we identified only 7 of 11 biceps tendon ruptures. Adhesion of a torn tendon at the joint entry point on the groove is the most likely cause of false-negative ultrasonograms. Two false-negative ultrasonograms had normal echogenicity for tendon fibers within the groove, giving the appearance of an intact tendon.
Our work was limited by the retrospective nature of our collection, however, when discrepancies in arthroscopic and ultrasonographic findings arose, HDD ultrasonograms and arthroscopic images were again carefully reviewed to explain the discrepancies. In addition, prior to this work, standardized criteria were established to determine the presence, location, and extent of rotator cuff tendon tears. Statistical analysis was based on the initial interpretation of the ultrasonographic examination rather than on a retrospective review of the images.
Although diagnostic arthroscopy was not performed blindly, the surgeon's knowledge of the ultrasonographic findings preoperatively was beneficial to the patient as the rotator cuff could be more specifically assessed, especially when the arthroscopic findings did not match the sonographic findings. In all shoulders in which the sonographic findings were inconsistent with the arthroscopic findings, the area of doubt was marked intraoperatively, allowing intra-articular cuff imaging as well as the bursa-side cuff image to be focused.
Patients with normal sonograms and pain relief did not undergo arthroscopy, and these patients were excluded from our study. Therefore, the actual number of false negatives could possibly be higher than that reported in our work. Patients with normal sonograms but persistent pain symptoms often underwent arthroscopy and were included in our study.
It should be noted that ultrasonography is a highly accurate and reliable method for identifying complete tears of the rotator cuff and dislocation of the biceps tendon in the case of pain in the shoulder joint. The high accuracy is due in part to improved image resolution, optimization of scanning techniques and the use of well-defined criteria. However, more than with all other imaging modalities used to evaluate the shoulder joint, the success of sonographic examination depends largely on the experience of the operator.
Literature
- Hyvonen P., Paivansalo M., Lebtiniemi H., Leppilahti J., Jalovaara P. Supraspinatus outlet view in the diagnosis of stages II and III impingement syndrome //Acta Radiol.-2001.-Vol.42.-P. 441-446.
- Worland RL, LeeD., Orozco CG, SozaRexF., Keenan J. Correlation of age, acromial morphology, and rotator cuff tear pathology diagnosed by ultrasound in asymptomatic patients //J. South. Orthop. Assoc.-2003.-Vol.12.-P. 23-26.
- Prickett WD, Teefey SA, et al. Accuracy of ultrasound imaging of the rotator cuff in shoulders that are painful postoperatively //J Bone Joint Surg.-2003.-Vol.85-A.-S.-P.1084-1089.
- van Holsbeeck MT, Kolowich PA, et al. US depiction of partial-thickness tear of the rotator cuff//Radiology.-1995.-V.197.-P. 443-446.
- Omari A., Bunker TD Open surgical release for frozen shoulder: surgical findings and results of the release //J Shoulder Elbow Surg.-2001.-Vol.10.-P. 353-357.
- Beall DP, Williamson EE, et al. Association of biceps tendon tears with rotator cuff abnormalities: degree of correlation with tears of the anterior and superior portions of the rotator cuff//AJR Am J Roentgenol, 2003.-Vol. 180. -P. 633-639.
- Humphreys CL Shoulder Injuries & Weight Training //Muscle Mag International.-1999.- Mississauga, ON CA.
- Teefey SA, Middleton WD et al. Sonographic differences in the appearance of acute and chronic full-thickness rotator cuff tears. //J Ultrasound Med.-2000.- 19.- S. 377-378; quiz 383.
- Hashimoto T., Nobuhara K., et al. Pathological evidence of degeneration as a primary cause of rotator cuff tear. //Clin Orthop Related Res.-2003.-Vol. 415.-P. 111-120.
- Umans HR, Pavlov H., Berkowitz M., Warren RF Correlation of radiographic and arthroscopic findings with rotator cuff tears and degenerative joint disease //J. Shoulder. Elbow. Surg.-2001.-Vol. 10.-P. 428-433.
- Martinoli C., Bianchi S. et al. US of the shoulder: non-rotator cuff disorders //Radiographics.-2003.-23.-P. 381-401, 534.
- Teefey SA, Hasan SA, et al. Ultrasonography of the rotator cuff. A comparison of ultrasonographic and arthroscopic findings in one hundred consecutive cases //J Bone Joint Surg.-2000.-Vol. 82.-P. 498-504.
- Green A. Arthroscopic treatment of impingement syndrome //Orthop. Clin. North Am.-1995.-Vol.26.-P. 631-641.
Ultrasound scanner HS60
Professional diagnostic tools.
Assessment of tissue elasticity, advanced 3D/4D/5D scanning capabilities, BI-RADS classifier, options for expert cardiological studies.
WHAT PATHOLOGIES CAN BE IDENTIFIED?
During an ultrasound examination, the following pathologies can be detected:
- Traumatic or degenerative damage to the muscle complex that ensures mobility of the shoulder joint - the rotator cuff;
- Fractures or cracks of the humerus;
- Tenosovinitis or bursitis are various inflammatory diseases of the joint;
- Injury or displacement of the humeral process of the scapula;
- Rupture of the articular labrum - the cartilage tissue surrounding the socket of the joint;
- Excessive or insufficient amount of fluid in the joint cavity;
- Connective tissue damage – arthritis;
- Muscular atrophy – a decrease in the number of muscles and a decrease in their functionality;
- A synovial cyst is a benign formation that on ultrasound looks like a small darkened area with uneven contours;
- Osteoarthritis is a disease during which the cartilage tissue of the joint becomes thinner and loses functionality. Usually accompanied by pain and limited mobility.
- Inflammation of the synovial bursa.
If during the diagnosis any of the listed diseases were identified, do not rush to get upset. If the pathology is detected at the initial stage, drug therapy usually helps to restore the functionality of the joint.
Cost difference
The affordable price of joint ultrasound allows all patients to undergo examination. You just need to make an appointment for a scan at a time convenient for you. MRI of the shoulder joint is a more expensive test. However, the information content of MRI of joints is certainly higher than ultrasound examination. Therefore, if alarming signs of inflammation are detected, orthopedists often refer the patient for a magnetic resonance examination rather than an ultrasound.
| Service | Price according to Price | Discount Price at Night | Discount Price During the Day |
| Shoulder MRI | 4000 rub. | 3190 rub. | 3690 rub. |
| Appointment with an orthopedist | 1800 rub. | free after MRI | free after MRI |
| First aid program for joints (8 studies + appointment with an orthopedist + MRI of the joint) | 13000 rub. | 7500 rub. | 7500 rub. |
| Ultrasound services of joints | price, rub. |
| Ultrasound of the shoulder joint | 1500 rub. |
| Ultrasound of the elbow joint | 1500 rub. |
| Ultrasound of the hip joint | 1500 rub. |
| Ultrasound of the knee joint | 1500 rub. |
| Ultrasound of the ankle joint | 1500 rub. |
| Ultrasound of one small joint (hand, foot) | 1000 rub. |
| Ultrasound of two small joints | 2000 rub. |
| Ultrasound of two large joints | 2500 rub. |
Author: Usenko Nikita Sergeevich
Orthopedist-traumatologist with 8 years of experience