Do your joints hurt? There is a risk of developing a disease such as arthralgia.
Arthralgia
– this is a set of painful sensations that arise due to predominantly organic damage to the joints. The presence of pain syndromes can be a harbinger of joint diseases, including the initial stages of arthrosis and arthritis.
Arthralgia is characterized by pain in the joints
Arthralgia syndrome - what is it?
Arthralgia
– these are pain sensations that can occur in one or several joints of the human musculoskeletal system. The disease is secondary and can be observed in diseases of infectious or autoimmune origin, as well as in the presence of excess body weight.
Joint pain is predominantly “volatile” in nature and usually appears unexpectedly and suddenly.
Painful sensations during arthralgia can occur without the influence of external irritating factors, which usually include increased loads and stress.
An attack of pain can last several minutes, or can last up to several hours. Everything is individual and depends solely on the area of progression of organic damage to the joint, as well as the pain threshold and, of course, the general health of the patient.
Often the pain goes away without the use of medications, however, there are cases when the use of analgesics is required.
The manifestation of the syndrome is distinguished according to factors such as:
- location;
- number of lesions;
- intensity and nature of pain;
- duration of pain;
- rhythmicity of discomfort.
Prevention
No one is one hundred percent protected, so prevention will not be unnecessary for anyone. It is important to always keep your body in good shape and give it moderate physical activity - do morning exercises, take breaks at work, try to walk more in the fresh air, spend less time sitting.
When walking, you not only warm up most of the muscles in the body, but also saturate it with oxygen, which is necessary for normal blood circulation and absorption of substances in the body. If possible, go swimming, jogging, and take mineral and mud baths. In summer, spend more time by the sea, go to a sanatorium.
Pay attention to your diet. Eliminate all foods harmful to the body, add vitamins and minerals. Eat healthy, easy-to-digest foods. It is very important for bones and joints to fill the body with calcium, so consume more dairy products.
Elena Belenko in the program “Doctor I” on TVC. Myalgia
Classification of arthralgia
Key challenge in the treatment of arthralgia
lies in the difficulties of diagnosing it, which is due to the large number of variations in its manifestation and clinical picture.
According to known data, arthralgia is divided into several classifications:
- infectious type
– the occurrence is provoked by general intoxication;
- intermittent
– accompanied by acute and recurrent arthritis;
- long lasting
– characteristic of exceptionally large joints (arthralgia of the knee or hip joint);
- oligo- or polyarthralgia
– the causes are inflammation of the joint, as well as destruction of cartilage tissue;
- post-traumatic
– appears as a residual manifestation of inflammation;
- false
.
It is important to note that each type is accompanied by a certain type of pain.
Arthralgia in children
Arthralgia in a child can be caused by age-related changes.
Sometimes arthralgia of the knee joint develops in children. This is due to the active growth of the student, so the process is considered natural. However, the syndrome may indicate diseases:
- malignant tumor;
- osteomyelitis;
- muscle inflammation;
- Osgood-Schlatter disease.
If your child complains of knee pain, contact a specialist and conduct a full examination. Without the necessary treatment, damage to joint tissues and destruction of the structure of the knees are possible. Take care to prevent such consequences.
Features of childhood arthralgia
Diagnosis of arthralgia in childhood
due to the presence of an acute infectious process. In such a situation, pain localized in the articular and periarticular tissues gradually increases and is aggravated by a feverish state, as well as general intoxication of the body.
Arthralgia in children requires special attention and treatment approach.
There are cases of multiple childhood arthralgia, which is accompanied by changes in the shape of the nail and finger phalanges, which may indicate the presence of serious malfunctions in the functioning of the heart, lungs or other internal organs.
It is important that a pathology of this kind that occurs in childhood requires a particularly careful approach, because if the diagnosis is incorrect or the existing symptoms are ignored, the pathology can become irreversible.
Treatment of the disease
Arthralgia is a disease that requires serious diagnosis and a long course of treatment. If the first syndromes do not go away within three days from the moment of the first manifestation, you should immediately contact a rheumatologist.
Drug therapy
The goal of drug treatment is to eliminate or correct the symptoms of arthralgia that were detected as a result of diagnosis. For these purposes, analgesic and anti-inflammatory medications such as Paracetamol or Aspirin are used.
In some cases, physical therapy may have to be used. It may include magnetic therapy, laser therapy, and heat treatment. In addition, compresses and ointments are used (Ketonal, Neuralgin, Finalgon, etc.).
Arthralgia in children has a slightly different character. Most of the drugs are contraindicated for children, so therapy is prescribed individually depending on the age and degree of the disease. Most often this is physical therapy, as well as simple normalization of the daily routine and an appropriate diet. However, in more acute forms, anti-inflammatory drugs are used only in extreme cases. If you start treatment on time, you can rid your child of the disease within 2-3 weeks.
ethnoscience
The first thing worth noting is that folk remedies are not aimed at eliminating arthralgia, but only at combating its symptoms and generally strengthening the body. Therefore, first of all, you need to consult a doctor and, with his permission, resort to using traditional methods.
One of the famous recipes is tincture of birch buds. For half a liter of boiling water you need to add two tablespoons of birch buds and let it brew for at least two hours. You should take this tincture half a glass twice a day.
Remember that it is not recommended to self-medicate without consulting a doctor, so as not to aggravate your condition and prevent the disease from developing quietly. This is especially important if we are talking about a child; you should not put him in danger - carry out treatment only as directed by a doctor.
Causes of arthralgia
Timely and competent identification of the causes of the disease is the basis for differential diagnosis of an existing health problem.
With the development of arthralgia it is quite difficult, one might say that it is almost impossible to notice visible changes on X-ray images. In addition, there are no symptoms of joint disease as such, including: swelling and crunching when moving.
Symptoms of arthralgia
is caused solely by irritation of the neuroreceptors of the joint capsule, which can be caused by such reasons as:
- joint damage of organic origin;
- development of the initial stage of arthrosis/arthritis;
- weakening of the immune system;
- severe allergic reaction;
- infectious lesion;
- tumor formations.
What causes arthralgia
Causes of joint pain syndrome:
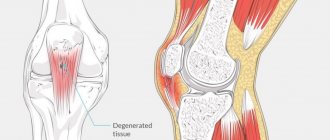
- Gonarthrosis or deforming osteoarthritis of the knee. It is characterized by dystrophic changes in the joint, cartilage and bone, as a result of which the functionality of the limb is significantly reduced. In its advanced form it causes severe pain and leads to disability.
- Reactive arthritis or Reiter's disease is an inflammatory disease that affects the joints. It worsens after infections of the nasopharynx, intestines or genitourinary system.
- Potentially dangerous medications. These medications are taken under the strict supervision of a doctor. After completing the course, the side effects disappear.
- Reactive arthralgia is a symptom of a general disease. Often the symptom is associated with a chronic infectious process that develops in a sluggish form. No special treatment is carried out, since the underlying disease needs to be eliminated.
- Gouty affection of the knees. Usually affects small vessels of the legs, in rare cases it affects large joints. Gout is caused by metabolic disorders, accumulation of urate, and stagnation of uric acid in the body.
Arthralgia is associated with inflammation and diseases of the knee joints that have not yet manifested themselves. A thorough examination is necessary to make a correct diagnosis.
Symptoms of arthralgia
The disease belongs to a category whose course is almost impossible to predict. Each case is individual and requires certain measures.
The disease is extremely variable. The main symptom of arthralgia is pain
, which can be fixed in a specific place or dynamically move. At the same time, it is important to note that the pain sensation can be of a different nature:
- aching/throbbing;
- sharp/blunt;
- intense/weak.
Diagnosis of arthralgia
If you experience systematic pain localized in any area of the musculoskeletal system, you should immediately seek medical help, the first stage of which is diagnosis.
Primary diagnosis is performed by a wide-spectrum specialist - a therapist, who determines the intensity of symptoms, collects the patient's medical history and refers to a specialized specialist.
The next stages of diagnostic examination are carried out by a rheumatologist. A set of certain knowledge, experience, as well as the availability of specialized equipment and the availability of various types of diagnostic methods allows you to accurately make a diagnosis, prescribe the correct treatment and monitor the effectiveness of the treatment method.
To differentiate the etiology of the disease, a number of objective studies are required, which include laboratory diagnostics (blood tests, biochemical tests). In addition, the following methods are used as clarifying methods:
- CT/MRI;
- research using ultrasound therapy.
Treatment of arthralgia
The entire process of treating arthralgia comes down to eliminating the disease that provokes the development of arthralgia syndrome. The treatment plan depends entirely on the existing concomitant diseases.
In the treatment of arthralgia, various methods can be used, in particular, medicinal and non-medicinal. Let's look at each of them in more detail.
Treatment of arthralgia is carried out using different methods
Treatment of arthralgia with medication
The treatment process is closely related to the severity of the symptoms of the disease.
So, in a situation where mild but sharp pain occurs, specialists choose treatment with medications and the use of various forms of drugs, a special place among which is occupied by analgesics.
Pronounced and at the same time long-lasting pain requires more serious measures and is eliminated exclusively by the injection method, using painkillers.
By studying the degree of effectiveness of the medications used, we can identify several groups of medications with the greatest therapeutic effectiveness. Among them:
- NSAIDs
– non-steroidal anti-inflammatory drugs in tablets or rectal suppositories;
- applications and compresses
;
- ointments with local anesthetic or warming effect
.
In addition, chondroprotectors are an excellent assistant in the regeneration of damaged tissues, among which the drug “Artracam”
.
Non-drug treatment for arthralgia
Physiotherapeutic procedures are considered one of the most popular non-drug treatment methods.
. Despite the fact that the use of methods of this kind is not justified in all cases, under the careful supervision of the attending physician, measures can be beneficial with an integrated approach to the treatment of diverse diseases.
Physiotherapeutic measures are prescribed taking into account the medical history of each individual patient and are regulated by an established treatment plan. It is important to note that physiotherapy is contraindicated in autoimmune pathologies, but in a situation where dystrophic processes are observed (especially caused by dystrophic processes), treatment should be started as soon as possible.
Among the most effective methods of physiotherapeutic treatment
highlight:
- electrophoresis;
- exposure to a magnetic field;
- UHF therapy;
- laser exposure;
- balneological treatment;
- paraffin therapy;
- use of therapeutic mud.
Surgical intervention
Joint pain may be an indication for various types of surgery. The basis for surgical intervention may be previous injuries or the presence of chronic diseases.
Operations can be carried out using two methods:
- open;
- using endoscopic equipment.
- Taking into account the existing symptoms, as well as the causes of pain, the following operations can be performed:
- arthroplasty, plastic surgery of the ligaments of the joint;
- removal of pathological formations;
- joint endoprosthetics.
The International Statistical Classification of Diseases and Problems, 10th revision (ICD-10), currently in use, is a normative document that ensures the formation of unified statistical control over the activities of medical institutions, assessment of the epidemiological situation in the country, and allows for the unity and comparability of incoming medical data [1] . ICD-10 is one of the important methodological tools for processing statistical data, which is extremely necessary for automating basic planning, regulatory and management work [2]. Unfortunately, this classification contains errors, both in the structural design of clinical sections and in the coding of a number of diseases. Some of the diagnoses that exist in it sound somewhat absurd; there is a confusion of placement of individual polyetiological diseases and syndromes in sections, which are often located in chapters that have a very indirect relationship to this nosology. In addition, many nosological forms, syndromes and symptoms that are currently common are not included in the accepted classification, which undoubtedly significantly limits the practical application of ICD-10.
The variety of different forms of diseases complicates the structure of the classification, so the latest revision has become much larger in volume and was accompanied by extensive guidelines, unfortunately, often without taking into account clinical practice. As a result, some of the clinical diagnoses ended up within the limits of unrefined conditions or conditions that were not sufficiently differentiated, and not in the headings or subheadings of the corresponding sections of the classification.
A number of difficulties arise with regard to the topographic classifications and terms used in ICD-10, many of which are imprecise, contradictory and do not correspond to clinical practice. Unfortunately, it should be noted that ICD-10 cannot currently be recommended as a model for terminology and recording of clinical diagnoses in medical records and other medical records.
To solve the problem of uniform standardization of medical diagnoses and statistical records, back in the late 70s of the last century, the idea arose of creating a “family” of classifications of diseases and health problems based on the ICD, adapted to a specific specialty, taking into account modern achievements of medical science.
Classification options for dentists, oncologists, dermatologists, rheumatologists and orthopedists, pediatricians, psychiatrists, and general practitioners have been published and recommended by WHO. Unfortunately, in the field of andrology there is still no unified classification [2].
Currently, the Research Institute of Urology is developing printed and electronic versions of a similar classification for urology and andrology, which is based on three-digit and four-digit ICD-10 codes. The coding system for urological and andrological diseases is presented in the form of a tree, where each subnode refines the information of the previous node. When forming a subnode, a number from zero to nine is added to the main code through a dot. The proposed system also provides for taking into account the localization of the pathological process, its stage and/or phase [3-5].
The creation of a printed and electronic version of a new unified clinical and statistical classification of andrological diseases will allow:
- facilitate data collection and improve the analysis of statistical material on andrology by increasing the reliability of statistical information and reducing the number of errors due to inconsistency of clinical diagnoses with ICD-10 diagnoses;
- provide a detailed assessment of the complexity of clinical cases and final treatment results when providing specialized (including high-tech) medical care;
- standardize the formulation of andrological diagnoses in medical documents and computer information systems of health authorities of the Russian Federation;
- improve the economic and statistical analysis of the provision of medical care in the field of andrology in the interests of healthcare of the Russian Federation, individual medical institutions and compulsory health insurance (CHI);
- optimize costs for diagnosis and treatment of andrological diseases.
It should be taken into account that andrological diseases, as a rule, are multi-etiological and many of them do not fit only into the framework of the block “Diseases of the male genital organs”. The modern concept of andrology is, of course, based on interdisciplinary interaction and is at the intersection of related medical disciplines (urology, endocrinology, psychiatry, genetics, neurology, therapy, etc.). Therefore, andrological diseases are heterogeneous in nature and are widely represented in different sections of ICD-10 (Table 1).
Table 1. General classification of andrological diseases according to ICD-10 and proposals for its correction
| ICD-10 code | Nosology | Correction and comments |
| 1 | 2 | 3 |
| A54.0 | Gonococcal infection of the lower genitourinary tract without abscessation of the periurethral or accessory glands | |
| A54.1 | Gonococcal infection of the lower genitourinary tract with abscess formation of the periurethral and accessory glands | |
| A56 | Other chlamydial sexually transmitted diseases | |
| A56.0 | Chlamydial infections of the lower genitourinary tract | |
| A56.1 | Chlamydial infections of the pelvic organs and other genitourinary organs | |
| A56.2 | Chlamydial infection of the genitourinary tract, unspecified | |
| A56.8 | Chlamydial infections, sexually transmitted infections, other localization | |
| A59 | Trichomoniasis | |
| A59.0 | Urogenital trichomoniasis | |
| A60 | Anogenital herpetic viral infection (herpes simplex) | |
| A60.0 | Herpetic infections of the genitals and genitourinary tract | |
| D17.6 | Benign neoplasm of adipose tissue of the spermatic cord | |
| E28.0 | Excess estrogen | Controversial diagnosis. It has no clinical use in men. |
| E28.1 | Excess androgens | Controversial diagnosis. Not all specialists accept the upper limits of normal. |
| E29 | Testicular dysfunction | Controversial diagnosis. Has no clinical use. |
| E29.0 | Testicular hyperfunction | Controversial diagnosis. Has no clinical use. |
| E29.1 | Testicular hypofunction | Controversial diagnosis. Has no clinical use. |
| E29.8 | Other types of testicular dysfunction | Controversial diagnosis. Has no clinical use. |
| E29.9 | Testicular dysfunction, unspecified | Controversial diagnosis. Has no clinical use. |
| E89.5 | Testicular hypofunction after medical procedures | Controversial diagnosis. Has no clinical use. |
| F52 | Sexual dysfunction not due to organic disorders or diseases | We propose to reduce this diagnosis due to its uncertainty, and refer all cases of erectile dysfunction to paragraph N48.4. |
| F52.0 | Lack or loss of sexual desire | |
| F52.1 | Aversion to sexual intercourse and lack of sexual pleasure | |
| F52.2 | Lack of genital response | Controversial diagnosis. It has no clinical use in men. |
| F52.3 | Orgasmic dysfunction | |
| F52.4 | Premature ejaculation | Correction: F52.4: Ejaculation disorders |
| Correction: F52.4.0 Premature ejaculation. | ||
| Correction: F52.4.1 Delayed ejaculation. | ||
| Correction: F52.4.2 Retrograde ejaculation. | ||
| Correction: F52.4.3 Anejaculation. | ||
| F64.0 | Transsexualism | |
| F64.2 | Gender identity disorder in childhood | |
| F64.8 | Other gender identity disorder | |
| F64.9 | Gender identity disorder, unspecified | |
| F65 | Sexual preference disorders | |
| F65.6 | Multiple disorders of sexual preference | |
| F65.8 | Other disorders of sexual preference | |
| F65.9 | Disorder of sexual preference, unspecified | |
| F66 | Psychological and behavioral disorders associated with sexual development and orientation | |
| F66.0 | Sexual maturation disorder | |
| F66.1 | Egodystonic sexual orientation | |
| F66.2 | Sexual relationship disorder | Controversial diagnosis. Correction: sexual disharmony. |
| F66.8 | Other psychosexual developmental disorders | |
| F66.9 | Psychosexual development disorder, unspecified | |
| F68.0 | Exaggeration of somatic symptoms for psychological reasons | |
| F83 | Mixed specific psychological development disorders | |
| F84 | General psychological disorders | |
| I86.1 | Varicose veins of the scrotum (varicocele) | |
| Correction: I86.1.0 Varicocele on the left. | ||
| Correction: I86.1.1 Varicocele on the right. | ||
| Correction: I86.1.2 Varicocele hemodynamic type 1 (renotesticular type of reflux). | ||
| Correction: I86.1.3 Varicocele hemodynamic type 2 (ileotesticular type of reflux). | ||
| Correction: I86.1.4 Varicocele hemodynamic type 3 (mixed type of reflux). | ||
| Correction: I86.1.5 Bilateral varicocele. | ||
| N34.0 | Urethral abscess | |
| N34.1 | Nonspecific urethritis | |
| N34.2 | Other urethritis | |
| N35 | Urethral stricture | |
| N35.0 | Post-traumatic urethral stricture | |
| N35.1 | Post-infectious urethral stricture, not elsewhere classified | |
| N35.8 | Other urethral stricture | |
| N35.9 | Urethral stricture, unspecified | |
| N36 | Other urethral diseases | |
| N36.0 | Urethral fistula | |
| N36.1 | Urethral diverticulum | |
| Correction: N36.2 Stenosis of the external urethral meatus. | ||
| Correction: N36.3 Obliteration of the urethra. | ||
| N36.8 | Other specified diseases of the urethra | |
| N36.9 | Urethral disease, unspecified | |
| N37* | Lesions of the urethra in diseases classified elsewhere | |
| N37.0* | Urethritis in diseases classified elsewhere | |
| N37.8* | Other lesions of the urethra in diseases classified elsewhere | |
| N39 | Other diseases of the urinary system | |
| N39.0 | Urinary tract infection without established localization | |
| N39.3 | Involuntary urination | |
| N39.4 | Other specified types of urinary incontinence | |
| N39.8 | Other specified diseases of the urinary system | |
| N39.9 | Urinary system disorder, unspecified | |
| N40 | Benign prostatic hyperplasia | |
| Correction: N40.0 With impaired quality of urination. | ||
| Correction: N40.1 Without affecting the quality of urination. | ||
| N41.0 | Acute prostatitis | |
| N41.1 | Chronic prostatitis | |
| Correction: N41.1.0 Chronic bacterial prostatitis. | ||
| Correction: N41.1.1 Chronic abacterial prostatitis. | ||
| Correction: N41.1.1.1 Abacterial CP with the presence of inflammation. | ||
| Correction: N41.1.1.2 Abacterial CP without signs of inflammation. | ||
| Correction: N41.1.2 Asymptomatic chronic prostatitis. | ||
| N41.2 | Prostate abscess | |
| N41.3 | Prostatocystitis | Controversial diagnosis. Has no clinical use. We propose to reduce this diagnosis. Correction: N41.3 Colliculitis. |
| Correction: N41.4 Sclerosis of the prostate gland. | ||
| N41.8 | Other inflammatory diseases of the prostate gland and seminal vesicles | |
| N41.9 | Inflammatory disease of the prostate, unspecified | |
| N42 | Other prostate diseases | |
| N42.0 | Prostate stones | Controversial diagnosis. Has no clinical use. We propose to reduce this diagnosis. Correction: Simple prostate cyst. |
| N42.1 | Congestion and hemorrhage in the prostate gland | Controversial diagnosis. Has no clinical use. We propose to reduce this diagnosis. |
| N42.2 | Prostate atrophy | |
| N42.8 | Other specified prostate diseases | |
| N42.9 | Prostate disease, unspecified | |
| N43 | Hydrocele and spermatocele | We propose in paragraph N43 to consider only hydrocele. |
| N43.0 | Hydrocele encyscum | Controversial diagnosis. Has no clinical use. We propose to reduce this diagnosis. Correction: Hydrocele on the left. |
| N43.1 | Infected hydrocele | Correction: Hydrocele on the right. |
| N43.2 | Other forms of hydrocele | Correction: Infected hydrocele. |
| N43.3 | Hydrocele, unspecified | Correction: Uninfected hydrocele. |
| N43.4 | Spermatocele | Correction: Hydrocele, unspecified. |
| Correction: N43.5 Spermatocele. | ||
| N44 | Testicular torsion | Correction: N44.0 Testicular torsion. |
| Correction: N44.1 Torsion of Morgagni's hydatid. | ||
| N45 | Orchitis and epididymitis | |
| N45.0 | Orchitis, epididymitis and epididymo-orchitis with abscess | Correction: Unilateral orchitis, epididymitis and epididymo-orchitis with abscess. |
| N45.9 | Orchitis, epididymitis and epididymo-orchitis without mention of abscess | Correction: N45.1 Unilateral orchitis, epididymitis and epididymo-orchitis without abscess. |
| Correction: N45.2 Bilateral orchitis, epididymitis and epididymo-orchitis with abscess. | ||
| Correction: N45.3 Bilateral orchitis, epididymitis and epididymo-orchitis without abscess. | ||
| N46 | Male infertility | Due to the polyetiological nature of the factors leading to male infertility, we propose to differentiate these forms depending on the causative factors. |
| Correction: N46.0 Male infertility caused by dysfunction at the level of the hypothalamus/pituitary gland. | ||
| Correction: N46.1 Male infertility caused by dysfunction at the testicular level. | ||
| Correction: N46.2 Male infertility caused by dysfunction of the efferent seminal tract and accessory sex glands. | ||
| Correction: N46.3 Male infertility caused by an ejaculation defect. | ||
| Correction: N46.4 Male infertility caused by an immunological factor. | ||
| Correction: N46.5 Male infertility caused by dysfunction of other androgen target organs. | ||
| Correction: N46.6 Male infertility, idiopathic form. | ||
| ALTERNATIVE CLASSIFICATION OF MALE INFERTILITY | ||
| Correction: N46.0 Male infertility is caused by a damaging external factor. | ||
| Correction: N46.1 Male infertility is caused by chromosomal pathology. | ||
| Correction: N46.2 Male infertility is caused by an anomaly in the structure or development of the male genital organs. | ||
| Correction: N46.3 Male infertility is caused by an endocrine factor. | ||
| Correction: N46.4 Male infertility is caused by infectious and inflammatory diseases of the male genital organs. | ||
| Correction: N46.5 Male infertility is caused by an immunological factor. | ||
| Correction: N46.6 Male infertility is caused by an iatrogenic factor. | ||
| Correction: N46.7 Male infertility is caused by an isolated pathology of seminal plasma. | ||
| Correction: N46.8 Idiopathic male infertility. | ||
| N47 | Excessive foreskin, phimosis and paraphimosis | Correction: N47.0 Excessive foreskin. |
| Correction: N47.1 Phimosis. | ||
| Correction: N47.2 Paraphimosis. | ||
| Correction: N47.3 Functional paraphimosis. | ||
| N48 | Other diseases of the penis | |
| N48.0 | Leukoplakia of the penis | |
| N48.1 | Balanoposthitis | |
| Correction: N48.1.0 Acute balanoposthitis. | ||
| Correction: N48.1.1 Chronic balanoposthitis. | ||
| N48.2 | Other inflammatory diseases of the penis | |
| Correction: N48.2.0 Cavernit. | ||
| Correction: N48.2.1 Serous cavernitis. | ||
| Correction: N48.2.2 Purulent cavernitis. | ||
| Correction: N48.2.3 Cavernous fibrosis. | ||
| N48.3 | Priapism | |
| Correction: N48.3.0 Arterial priapism. | ||
| Correction: N48.3.1 Ischemic priapism. | ||
| Correction: N48.3.2 Nocturnal intermittent priapism. | ||
| N48.4 | Impotence of organic origin | We suggest making a correction: Psychosomatic syndrome of erectile dysfunction. |
| Correction: N48.4.0 Erectile dysfunction with a predominance of the organic component. | ||
| Correction: N48.4.1 Erectile dysfunction with a predominance of the psychogenic component. | ||
| N48.5 | Penile ulcer | |
| N48.6 | Balanitis | |
| Correction: N48.6.0 Acute balanitis. | ||
| Correction: N48.6.1 Chronic balanitis. | ||
| Correction: N48.6.2 Xerotic balanitis obliterans. | ||
| N48.8 | Other specified diseases of the penis | |
| Correction: N48.8.0 Small penis. | ||
| Correction: N48.8.1 Ectopia of the penis. | ||
| Correction: N48.8.2 Double penis. | ||
| Correction: N48.8.3 Webbed penis. | ||
| Correction: N48.8.4 Retractile penis. | ||
| Correction: N48.8.5 Hidden penis. | ||
| Correction: N48.8.6 Peyronie's disease. | ||
| Correction: N48.8.6.0 Peyronie's disease in the active stage. | ||
| Correction: N48.8.6.1 Peyronie's disease in the functional stage. | ||
| N48.9 | Disease of the penis, unspecified | |
| N49 | Inflammatory diseases of the male genital organs, not elsewhere classified | |
| N49.0 | Inflammatory diseases of the seminal vesicle | Correction: Vesiculitis. |
| Correction: N49.0.0 Acute vesiculitis. | ||
| Correction: N49.0.1 Chronic vesiculitis. | ||
| N49.1 | Inflammatory diseases of the spermatic cord, tunica vaginalis and vas deferens | |
| N49.2 | Inflammatory diseases of the scrotum | |
| Correction: N49.3 Fournier's gangrene. | ||
| N49.8 | Inflammatory diseases of other specified male genital organs | |
| N49.9 | Inflammatory diseases of the unspecified male genital organ | |
| N50 | Other diseases of the male genital organs | |
| N50.0 | Testicular atrophy | |
| N50.1 | Vascular disorders of the male genital organs | Controversial diagnosis. Has no clinical significance. |
| Correction: N50.2 Contact dermatitis of the genitals. | ||
| N50.8 | Other specified diseases of the male genital organs | |
| N50.9 | Male genital disease, unspecified | |
| N51* | Lesions of the male genital organs in diseases classified elsewhere | |
| N51.0* | Lesions of the prostate gland in diseases classified elsewhere | |
| N51.1* | Lesions of the testicle and its appendages in diseases classified elsewhere | |
| N51.2* | Balanitis in diseases classified elsewhere | |
| N51.8* | Other lesions of the male genital organs in diseases classified elsewhere | |
| N51.8* | Other lesions of the male genital organs in diseases classified elsewhere | |
| N94.1 | Dyspareunia | |
| N99 | Disorders of the genitourinary system after medical procedures not classified elsewhere | |
| N99.1 | Postoperative urethral stricture | |
| N99.8 | Other disorders of the genitourinary system after medical procedures | |
| N99.9 | Disorders of the genitourinary system after medical procedures, unspecified | |
| Q53 | Undescended testicle | |
| Q53.0 | Ectopic testicle | |
| Q53.1 | Unilateral undescended testicle | |
| Q53.2 | Bilateral undescended testicle | |
| Correction: Q53.3 Pseudocryptorchidism. | ||
| Q53.9 | Undescended testicle, unspecified | |
| Q54 | Hypospadias | |
| Q54.0 | Hypospadias of the glans penis | |
| Q54.1 | Penile hypospadias | |
| Q54.2 | Hypospadias penis-scrotum | |
| Q54.3 | Perineal hypospadias | |
| Q54.4 | Congenital curvature of the penis | |
| Q54.8 | Other hypospadias | Correction: Hypospadias without hypospadias. |
| Q54.9 | Hypospadias, unspecified | |
| Q55 | Other congenital anomalies [malformations] of the male genital organs | |
| Q55.0 | Absence and aplasia of the testicle | |
| Q55.1 | Testicular and scrotal hypoplasia | |
| Q55.2 | Other congenital anomalies of the testicle and scrotum | |
| Correction: Q55.2.0 Monorchidism. | ||
| Correction: Q55.2.0.0 Monorchidism on the right. | ||
| Correction: Q55.2.0.1 Monorchidism on the left. | ||
| Correction: Q55.2.1 Polyorchidism. | ||
| Correction: Q55.2.2 Synorchidism. | ||
| Q55.3 | Atresia of the vas deferens | |
| Q55.4 | Other congenital anomalies of the vas deferens, epididymis, spermatic cord and prostate | |
| Q55.5 | Congenital absence and aplasia of the penis | |
| Q55.6 | Other congenital anomalies of the penis | |
| Q55.8 | Other specified congenital anomalies of the male genital organs | |
| Q55.9 | Congenital anomaly of the male genital organs, unspecified | |
| Q56 | Sex ambiguity and pseudohermaphroditism | |
| Q56.0 | Hermaphroditism, not elsewhere classified | |
| Q56.1 | Male pseudohermaphroditism, not elsewhere classified | |
| Q56.3 | Pseudohermaphroditism, unspecified | |
| Q56.4 | Gender ambiguity, unspecified | |
| Q64 | Other congenital anomalies [malformations] of the urinary system | |
| Q64.0 | Epispadias | |
| Correction: Q64.0.0 Epispadias of the head. | ||
| Correction: Q64.0.1 Penile epispadias. | ||
| Correction: Q64.0.2 Total epispadias. | ||
| Q64.1 | Bladder exstrophy | |
| Q64.2 | Congenital posterior urethral valves | |
| Q64.3 | Other types of atresia and stenosis of the urethra and bladder neck | |
| Q64.5 | Congenital absence of the bladder and urethra | |
| Q64.7 | Other congenital anomalies of the bladder and urethra | |
| Q64.8 | Other specified congenital anomalies of the urinary system | |
| Q64.9 | Congenital anomaly of the urinary system, unspecified | |
| Q89.7 | Multiple congenital anomalies not elsewhere classified | |
| Q89.8 | Other specified congenital anomalies | |
| Q89.9 | Congenital anomaly, unspecified | |
| Q92.7 | Triploidy and polyploidy | |
| Q95.3 | Balanced sexual/autosomal rearrangements in a normal individual | |
| Q98.0 | Klinefelter syndrome, karyotype 47,XXY | |
| Q98.1 | Klinefelter syndrome, male with more than two X chromosomes | |
| Q98.2 | Klinefelter syndrome, man with 46,XX karyotype | |
| Q98.3 | Another man with a 46,XX karyotype | |
| Q98.4 | Klinefelter's syndrome, unspecified | |
| Q98.5 | Karyotype 47,XYU | |
| Q98.6 | A man with structurally altered sex chromosomes | |
| Q98.7 | Male with mosaic sex chromosomes | |
| Q98.8 | Other specified sex chromosome abnormalities, male phenotype | |
| Q98.9 | Sex chromosome abnormality, male phenotype, unspecified | |
| Q99 | Other chromosomal abnormalities not elsewhere classified | |
| Q99.0 | Mosaic [chimera] 46,ХХ/46,ХY | |
| Q99.1 | 46.XX true hermaphrodite | |
| Q99.2 | Fragile X chromosome | |
| Q99.8 | Other specified chromosomal abnormalities | |
| Q99.9 | Chromosomal abnormality, unspecified | |
| R10.2 | Pain in the pelvis and perineum | |
| R30.9 | Painful urination, unspecified | |
| R32 | Urinary incontinence, unspecified | |
| R33 | Urinary retention | |
| R36 | Discharge from the urethra | |
| R39 | Other symptoms and signs related to the urinary system | |
| R39.1 | Other difficulties related to urination | |
| R39.8 | Other and unspecified symptoms and signs related to the urinary system | |
| R44.8 | Other and unspecified symptoms and signs relating to general sensations and perceptions | |
| R45 | Symptoms and signs related to emotional state | |
| R45.0 | Nervousness | |
| R45.1 | Anxiety and agitation | |
| R45.2 | State of anxiety due to failures and misfortunes | |
| R45.3 | Demoralization and apathy | |
| R45.4 | Irritability and anger | |
| R45.7 | State of emotional shock and stress, unspecified | |
| R45.8 | Other symptoms and signs related to emotional state | |
| R46 | Symptoms and signs related to appearance and behavior | |
| R52.1 | Constant, unrelieved pain | |
| R52.2 | Other constant pain | |
| R52.9 | Unspecified pain | |
| R53 | Malaise and fatigue | |
| R54 | Old age | Controversial diagnosis. |
| R62 | Lack of expected normal physiological development | |
| R62.0 | Delayed developmental milestones | |
| R62.8 | Other delays in expected normal physiological development | |
| R62.9 | Lack of expected normal physiological development, unspecified | |
| S30.2 | Bruise of the external genitalia | |
| S31.2 | Open wound of the penis | |
| S31.3 | Open wound of the scrotum and testicles | |
| S31.5 | Open wound of other and unspecified external genitalia | |
| S38.0 | Crushing of the external genitalia | |
| S38.2 | Traumatic amputation of the external genitalia | |
| T19 | Foreign body in the genitourinary tract | |
| T19.0 | Foreign body in the urethra | |
| T19.8 | Foreign body in another or several parts of the genitourinary tract | |
| T19.9 | Foreign body in an unspecified part of the genitourinary tract | |
| Z84.2 | Family history of other diseases of the genitourinary system | |
| Z87.4 | Personal history of diseases of the genitourinary system | |
| Z90.7 | Acquired absence of sexual organ(s) | |
| Z99.8 | Dependence on other auxiliary mechanisms and devices | |
This summary table shows those symptoms, syndromes and nosological forms according to ICD10 that a practicing specialist in the field of andrology encounters in real practice. At the same time, in our opinion, some of them no longer correspond to the modern understanding of pathophysiological processes and require terminological and classification clarification (right column).
Naturally, the above classification needs to be supplemented and refined, and fundamental amendments be made taking into account interdisciplinary interaction. With our publication, we would like to provoke a discussion among specialists in the field of andrology, the main goal of which would be to create a single, integral classification of andrological diseases. This is undoubtedly valuable and convenient for medical practitioners, health authorities, scientific research, and insurance companies. We will be grateful for your comments and remarks, which can be sent to the email address
Key words: ICD-10, andrological diseases, clinical and statistical classification.
Keywords : ICD-10, andrology diseases, clinical and statistical classification.
Literature
- International classification of diseases and related health problems. WHO, 1992
- Order of the Ministry of Health of the Russian Federation dated May 27, 1997 No. 170 (as amended on January 12, 1998) “On the transition of health authorities and institutions of the Russian Federation to the international statistical classification of diseases and health-related problems of the X revision.”
- Sivkov A.V., Kakorina E.P., Keshishev N.G. Unified clinical and statistical classification of urological diagnoses // Materials of the XI Congress of Urologists of Russia. M. 2007. pp. 598-599.
- Unified clinical and statistical classification of urolithiasis / Apolikhin O.I., Dzeranov N.K., Sivkov A.V., Kakorina E.P., Keshishev N.G. // Urology. 2008. No. 6. P. 3-6.
- On the creation of a unified clinical and statistical classification of oncological urological diseases using the example of kidney tumors / Apolikhin O.I., Sivkov A.V., Chernyshev Yu.V., Kakorina E.P., Keshishev N.G., Zhernov A.A. // Experimental and clinical urology. 2010. No. 1. pp. 23-28.
| Attached file | Size |
| Article in PDF format | 414.14 kb |