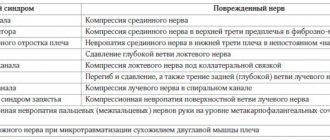
Development mechanism
Mechanism of development
The shoulder joint is one of the most complex structures of the human musculoskeletal system. The glenoid cavity is formed by the clavicle and the acromion process of the scapula, and contains the head of the humerus.
The spherical shape of the joint provides a significant range of movements of the upper limb in various planes, including rotation (shoulder rotation). Increasing the depth of the glenoid cavity and increasing the stability of the shoulder joint is provided by a lip made of connective tissue localized around the cavity, as well as a cuff formed from the glenohumeral ligaments and muscles that provide rotation of the shoulder (rotators).
Under the acromial process of the scapula there is a muscle located, which is one of the most vulnerable structures of the shoulder. The result of its damage is rotator cuff syndrome or impingement syndrome.
The shoulder joint is the most mobile, spherical, sharply incongruent and multi-spinous joint of the human body, connecting the head of the humerus and the articular surface of the scapula.
Shoulder instability is a chronic condition of repeated dislocation or subluxation of the humeral head.
The lion's share (95-98%) of all dislocations are anterior (subcoracoid and subclavian) or so-called anterior-inferior dislocations, the remaining percentage is shared by posterior and multiplanar shoulder dislocations.
Causes of chronic instability:
- Consequence of traumatic dislocation (fracture-dislocation)
- Hyperelasticity syndrome (Ehlers-Danlos, Marfan Syndrome), which affects 10-15% of the population
- Hypermobility of the shoulder joint caused by repetitive movements with maximum amplitude, some professions and sports are at risk, such as swimming, volleyball, tennis (throwing sports - “throwing athlete’s shoulder”)
- Dysplastic changes - a difference in the size of the humeral head and the glenoid cavity of the scapula, its planar position
- Features of the structure of the articular labrum and glenohumeral ligaments
The diagnosis is made based on examination and complaints; MRI and X-ray CT are used to clarify structural damage.
Treatment of instability is exclusively surgical; attention has been paid to this pathology for many centuries; the first mentions begin with Hippocrates (400 BC) - he used cauterization with a hot iron. Over the entire history of attempts to prevent dislocation, about 150 methods of surgery and about 300 of their modifications have been invented. There is still no treatment method that would relieve the patient of the problem with 100% certainty, but with the advent of arthroscopy there was a breakthrough in the surgical treatment of shoulder instability. The operation became as anatomical as possible, it became possible to see the joint from the inside and identify concomitant pathologies about which there was not the slightest idea before.
Common features of arthroscopic operations on the shoulder joint are: performing the intervention through punctures, using high-definition video equipment, and instruments for minimally invasive surgery.
Pain relief for patients is always multicomponent; in our clinic we combine conduction anesthesia (blockade of peripheral nerves with an anesthetic) with the use of a laryngeal mask.
Interventions are carried out with the patient in special positions: “on the side” with the arm abducted, or “chaise lounge”
To fix damaged structures: capsules, ligaments, tendons, osteochondral fragments, anchors are used (anchor - anchor fixator, metal and polymer: non-absorbable and biodegradable).
There are fixators of various sizes and shapes, made of different materials, with specific purposes - for dense cortical and loose cancellous bone. Some are holes that become clogged and require drilling, others are self-tapping screws that are screwed into the bone. Everyone is united by super-strong threads running inside.
Bankart injury is the most common in shoulder dislocation - separation of the cartilaginous lip (labrum) from the glenoid cavity of the scapula. The tendon of the long head of the biceps brachii muscle (biceps) is attached to its upper section, and powerful ligaments woven into the capsule are attached to the anterior and posterior sections.
This is what lip avulsions in the upper (SLAP) and anterior-inferior (Bankart) sections look like in the diagram (English surgeon Arthur Sidney Blundell Bankart, 1879 - 1951).
It is worth noting that multiple (speaking of the number, patients often talk about more than 50, 100 episodes, and some have long lost count, since dislocations that often occur in sleep are corrected on their own) dislocations of the shoulder, not a trace remains of the labrum, The glenohumeral ligament (GHL) and capsule are torn, the anterior chamber of the joint increases in size, and the articular surface of the scapula narrows.
Inside the shoulder diagram of the seams after reconstruction
There are many types of ruptures of the glenoid labrum, capsule, and ligaments, but it is necessary to say about the bone damage that accompanies the dislocation:
The Hill -Sachs fracture (Harold Arthur Hill (1901–1973) and Maurice David Sachs (1909–1987)) is an impression (depressed) fracture of the humeral head. The longer the humeral head is in a state of dislocation, the higher the energy of the injury, the worse the quality of the bone (osteoporosis), the more pronounced the defect will be and the cartilaginous covering of the humeral head will decrease, and therefore the risk of relapse will increase - repeated slipping into the usual place. With this pathology, depending on the size of the defect, bone grafting or, for example, a remplissage .
(French remplissage - filling)
Bone Bankart is a fracture of the glenoid cavity of the scapula.
This injury is accompanied by a decrease in the area of the articular surface of the scapula; it must be diagnosed as soon as possible, since the choice of conservative and surgical treatment tactics depends on this. The standard projections used for radiography of the shoulder joint often do not reveal a fracture of the anterior edge of the glenoid, especially if it is small. Therefore, the examination standards include magnetic resonance and x-ray computed tomography with 3D reconstruction.
Arthroscopy remains the best diagnostic and treatment method.
Depending on the size of the defect (lack of bone mass - b), age of the fracture, number of dislocations, quality of bone tissue, the volume of surgical intervention is planned:
refixation of an avulsion fracture, plastic surgery of the ligamentous apparatus, or osteoplastic surgery using an autograft (bone block taken from the patient) from the iliac crest. Or use of the coracoid process of the scapula (coracoid) - Latarget operation (Bristow-Helfet-Latarget).
Rehabilitation after stabilizing operations on the shoulder joint usually begins after 3-4 weeks with passive development - the patient is helped to restore the range of motion of the limb using the healthy arm. Instructions from a physiotherapist and assistance from a massage therapist are required. After achieving the required amplitude within 7-10 days, you can begin active development - “switching on” the muscles of the shoulder girdle - active movements of the operated arm; at this time, the advice of a physical therapy instructor is very important. The average time for consolidation and fusion of ligaments ranges from 6 to 12 weeks, so loads are prohibited during this time. You can start active sports no earlier than after 4-6 months.
The long head of biceps tendon (LCT) and the pathology associated with it should be considered separately. The interest lies in the structural features and its intra-articular location. Often there is persistent pain in the anterior part of the shoulder joint, provoked by load, excessive motor pattern or injury. At the same time, when examining patients, tenosynovitis or tendonitis of the SDGB, sharp palpation pain in the projection of the intertubercular groove are detected, and MRI and arthroscopy reveal damage to the structures that support the tendon of the apparatus, often dislocation of the tendon or separation of the upper part of the articular labrum, discussed above. If conservative measures do not give the desired effect, tenodesis - securing the tendon in the intertubercular groove.
This can be done both externally and intraarticularly, using an interference bioabsorbable screw or anchor fixators. In old age, the muscle belly has almost no contour on the shoulder (especially in women), and tenotomy of the SDGB is permissible - cutting it off from the place of attachment, without any fixation. This has virtually no effect on the function of the arm; the range of motion in the shoulder and elbow joints does not suffer. A small cosmetic defect in the photo of the man on the left.
Calcific tendinitis is an inflammation of the rotator cuff tendon, accompanied by pain, limitation of movements, as well as the deposition of calcium salts (deposits of basic phosphates, more often Ca10(PO4)6OH - hydroxyapatite in the supraspinatus tendon, the type of calcification in the diagram and radiograph).
Causes.
It is assumed that the development of the disease is based on both local and general factors. Hydroxyapatite crystals are deposited in the initially damaged tendon, which explains the typical localization of these crystals in the tendons of the shoulder joint. As a rule, frequently injured and poorly supplied areas of tendons undergo calcification, sometimes with foci of necrosis, which contributes to a local increase in the concentration of calcium and phosphorus. Such a region is the area of the supraspinatus tendon near its attachment to the greater tubercle of the humerus - the Codman area, where calcifications are most often detected radiographically. In turn, calcification contributes to the further progression of degenerative changes, as well as the development of an inflammatory response. However, the frequent bilateral and multiple localization of deposits suggests the existence, along with local ones, of common predisposing factors, such as diabetes mellitus, thyroid diseases, and hyperphosphatasia. Familial cases of the disease have been described. Deposition of hydroxyapatite crystals in tissues has been described in many conditions, including in patients with chronic renal failure on long-term hemodialysis. Hydroxyapatite crystals are present in soft tissues in systemic scleroderma, dermatomyositis, mixed connective tissue disease, causing multiple calcification. Finally, calcification of periarticular tissues is known after previous intra-articular injections. The causes and mechanisms of calcification in all of these conditions remain unclear. (RMJ).
In our practice, it has been noticed that the prevailing number of patients are women whose professions involve prolonged forced positioning of the arm (microtraumatization), often abduction. For example, hairdressers, teachers, painters, doctors (ultrasound diagnosticians and dentists), etc.
Treatment is possible using physiotherapeutic methods; good results are observed after courses of extracorporeal shock wave therapy, with the help of which it is possible to achieve the dissolution of calcifications. In the case of massive salt deposits, after unsuccessful conservative therapy, it is possible to loosen the salt layer invasively under ultrasound guidance by injecting an anesthetic under the acromion process of the scapula. In advanced cases, with dense calcification, arthroscopic subacromial bursoscopy and removal of deposits through punctures cannot be avoided. Sometimes tendinitis with large calcifications spreads to all layers of the tendon mass of the rotator cuff , and after their removal, a tissue defect is formed that must be closed, i.e. stitch, repair a tear.
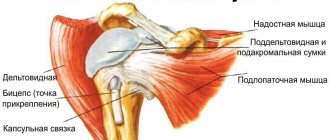
The rotator cuff is a joint tendon for several muscles: supraspinatus, infraspinatus and teres minor, which are a group of external rotators of the humerus attached to the greater tubercle of the humerus. There is also an internal rotator of the shoulder, which is part of the cuff - the subscapularis muscle (subscapularis), the tendon of which is attached to the lesser tubercle. Despite the intricacy of the tendon fibers of all four muscles and their structural unification, each has its own function, the common one is the stabilization of the head, its pressing and centering in the glenoid cavity of the scapula.
Rotator cuff tendon, muscles, top and side views.
There are many types of tendon ruptures and rotator cuff tears, some affecting function and others causing pain. Massive damage does not allow a person to care for himself, since the rotators are responsible for everyday, habitual movements. Personal hygiene becomes difficult (combing your hair, washing, etc.), sometimes impossible, especially if the dominant hand has been injured.
Treatment involves restoring the integrity of the structure - suture of the rotator cuff, performed arthroscopically in our clinic. Options for single-row and double-row fixation (anchor with threads and tapes).
Suture diagram (A) and arthroscopic view (B) after reconstruction
Rehabilitation
In the postoperative period, it is necessary to wear, for 3-4 weeks, an orthosis (retainer) - an immobilizing bandage with possible abduction and rotation of the arm in order to unload the muscles.
Then physiotherapy, massage, physical therapy are necessary, the prescription of drug therapy is justified, since the age of patients with rotator cuff injuries often ranges from 45 to 65 years.
Continuing the topic of older patients, it is necessary to mention degenerative damage in the absence of injury as such.
Impingement syndrome.
A condition in which the rotators are compressed, colliding with the acromion process of the scapula, during movements. And taking into account the suffering blood supply to this zone, damage to the cuff occurs, sometimes not full-thickness, partial ruptures (partial ruptures PASTA - partial articular supraspinatus tendon avulsion). They are accompanied by severe pain in extreme positions of the shoulder and are often difficult to diagnose even on MRI:
Age-related changes , such as: thinning of the cartilaginous layer, narrowing of the subacromial space, rigidity of the ligamentous apparatus, coupled with the anatomical structure, predisposition of some people, can lead to a similar disease (3 types of acromions, see below).
Problems arise with types 2 and 3 of the process; they serve as an obstacle to the greater tubercle and injure the cuff (supraspinatus tendon). There are also frequent cases of osteophytes appearing on the process, so-called spurs (examples on radiographs).
Y-projection to assess the shape of the acromion process and spur
True AP view for assessing joint space and subacromial space
Treatment is arthroscopic subacromial decompression, consisting of removal of the subacromial bursa (bursectomy) and spur, resection of the acromial process of the scapula (acromioplasty, see below).
For significant partial tears, in addition to expanding the space between the humerus and the scapula, the suture described above is also necessary.
Shoulder joint replacement is the replacement of worn, injured and irretrievably lost parts of the joint with artificial ones (metal, ceramic, polyethylene), a surgical method for treating pathologies such as:
- Osteoarthritis of the shoulder joint (arthrosis), often developed as a result of injury or professional activity
- Arthropathy of the shoulder joint occurs after a massive rupture of the rotator cuff tendons (English - Cuff tear arthropathy)
- Hass disease - aseptic osteonecrosis of the head of the humerus, osteochondropathy in which bone tissue cells die
- Congenital dysplastic disorders (abnormal development) of the humeral head and glenoid cavity of the scapula
- Comminuted fractures and fracture-dislocations of the proximal humerus, glenoid cavity of the scapula, the synthesis of which obviously disrupts the function of the shoulder joint.
- Rheumatoid arthritis.
For each pathology there is its own, strictly defined, depending on the damaged part, method of endoprosthetics:
Riserfacing - replacement of the surface of the destroyed cartilaginous layer, most often the head of the humerus, with a metal one (diagram and x-ray)
Unipolar endoprosthetics - replacement of one of two damaged structures, most often replacement of the head and neck of the humerus in case of fractures of its upper part (diagram and x-ray)
Total arthroplasty is the replacement of two components of the joint, i.e. the use of riserfacing techniques for contacting surfaces, or an anatomical prosthesis on a stem, with the replacement of the glenoid cavity of the scapula, as well as reverse arthroplasty (the reverse - the concave part is transferred to the pedicle of the shoulder, and the convex head to the articular scapula cavity), used, for example, in cases of arthropathy due to irreparable tears of the rotator cuff.
Below are examples of radiographs of total endoprostheses
Shoulder arthroplasty is a precise, high-tech operation, performed more often in patients of the older age group, the purpose of which is to return lost arm movement and relieve the patient of pain. The sooner the patient consults a doctor, the fewer complications will be avoided and you will be able to return to your favorite activities!
Rehabilitation begins with passive movements already 2-3 days after surgery, after pain has reduced, after 5-7 days it is possible to begin active physical therapy, the postoperative wound heals on days 10-12 and the sutures are removed. As the load increases and the range of movements increases, the patient consults with the operating surgeon and control X-ray examinations are carried out.
Shoulder capsulitis or frozen shoulder
The general term scapulohumeral periarthritis (described by Durlay in 1882), the above-mentioned term “Frozen shoulder” (suggested by Codman in 1932), adhesive capsulitis (used in ICD - 10) is also applicable - a neurotrophic disease characterized by inflammation of the synovial membrane, retraction and fibrosis of the capsule, i.e. a decrease in the volume of the joint and stiffness.
The reason is not fully understood; there is a connection with, sometimes minor, trauma - awkward movement, which led to severe pain and forced limitation of movements. Occurring separately, this disease often develops against the background of concomitant pathology. For example, in diabetes mellitus - up to 30% of cases, hyperthyroidism, previous myocardial infarction and stroke, oncopathologies, fibromatosis - connective tissue diseases. Females are more often affected (5:1), hormonal disorders, and a stress factor can be a possible cause of the disease, which has 3 phases (4):
- “red” - duration from 3 to 12 months - pain at rest, not associated with specific movement, worse at night.
- “red-white” - lasts from 4 to 12 months - painless severe limitation of movements, especially rotation. This is the freezing stage, with the shoulder pressed to the body and the forearm to the stomach.
- “white” - from 12 to 24 months the process is completed by the stage of “getting rid of stiffness”, the phase of development, pliability.
In general, the duration can take from 1.5 to 4 years according to different authors; the duration of each subsequent phase depends on the time of the previous one.
There is an opinion that one should not interfere with the disease process, since recovery always occurs - self-resolution. There have been cases of incomplete restoration of function, which many patients do not pay attention to. A number of other patients wish for a speedy recovery and restoration of function of the shoulder joint due to long-term disability.
Treatment boils down to relieving pain in the first phase with anti-inflammatory drugs. The use of glucocorticosteroids in the second phase, their intra-articular administration with an anesthetic, preferably under ultrasound control, physiotherapy, massage, shock wave therapy, active exhausting development of movements. Surgery is also possible - arthroscopic capsulotomy - dissection and redressing.
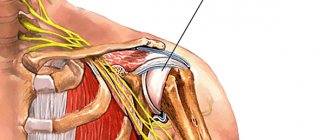
Continuing the topic of neurotrophic diseases, it is necessary to mention shoulder pain, sometimes associated with the above-mentioned pathologies, but caused by nerve compression or damage. These processes are best suited by the names “tunnel syndrome” and “neuropathy.” Anatomy has once again rewarded us with many forms. For example, below are 6 types of notch of the scapula in which the suprascapular nerve passes - n.suprascapularis (SSN).
Top view: 1 - scapular notch 2 - coracoid process 3 - superior transverse ligament 4 - suprascapular artery 5 - suprascapular nerve 6 - supraspinatus fossa 7 - scapular spine 8 - neck of the scapula 9 - inferior transverse ligament 10 - acromial process
The a.suprascapularis artery passes over the transverse ligament, as shown in the figure above, and the nerve lies in the notch of the scapula in the subglottic space. Compression of the nerve in these areas can be caused by the anatomical structure, muscle retraction due to rotator cuff tears, ganglion cysts, synovial cysts - benign fluid formations, etc. Determination requires accurate MRI and ultrasound diagnostics; needle electroneuromyography is used.
MRI and diagram of a cyst compressing a nerve
Clinically, pathologies associated with compression of the SSN are manifested by pain in the scapula with radiation to the shoulder joint, weakness, and sometimes atrophy of the rotator muscles. Damage to the suprascapular nerve occurs during sports such as weightlifting, basketball, volleyball, etc. The mechanism of injury is nerve pinching during arm movements in the shoulder joint, which is caused by rapid swings of the arm from behind the head. Suprascapular neuropathy results in persistent, dull pain behind the shoulder joint and weakness in arm abduction and external rotation.
Treatment consists of decompression (release) of the suprascapular nerve; surgical interventions are performed endoscopically - through punctures. Arthroscopy of the shoulder joint comes to the rescue again - it is possible to open and evacuate the contents of the cyst, dissect the transverse scapular ligament, depending on the found anomaly of the notch. In the early stages, it is possible to take NSAIDs, physiotherapy, carried out, if necessary, under ultrasound control, nerve blockade with anesthetic solutions in combination with glucocorticosteroids.
Pterygoid scapula is a rare neuropathy of the long thoracic nerve (LPN) n. thoracicus longus - arising as a result of its damage (overextension). Causes paresis or paralysis of the serratus anterior muscle, which is manifested by a wing-shaped position of the scapula. A similar unusual position of the scapula can occur with paralysis of the rhomboid and trapezius muscles as a result of traumatic injury to the accessory nerve, but in this case the lower angle of the scapula deviates outward, whereas in NDHN the lower angle of the scapula, on the contrary, deviates inward towards the spine. As a result of damage to all three muscles, in rare cases, varus alignment of the scapula occurs with progressive posterior subluxation of the shoulder. A type of pterygoid scapula is paralytic vara (loss of the serratus, trapezius and rhomboid muscles), combined with posterior subluxation of the shoulder (described by P. Ya. Fishchenko in 1967), examples in the photo below.
The arrows below indicate n. thoracicus longus and serratus anterior muscle
Treatment is aimed at stimulating the muscles of the shoulder girdle, improving nerve nutrition, standard physiotherapy, massage and exercise therapy are complemented by drug therapy, surgery is not required unless a rupture has occurred.
Damage to the axillary (axillary) nerve n.axillaris. The axillary nerve is mixed in function. The motor fibers of the nerve innervate the deltoid and teres minor muscles. The sensory fibers of the axillary nerve are part of the superior lateral cutaneous nerve of the shoulder and innervate the skin of the outer surface of the shoulder. Damage to the axillary nerve is possible due to a number of reasons. In most cases, neuropathy is caused by trauma, such as a fracture or dislocation of the shoulder, a gunshot wound, prolonged compression of nerve fibers (for example, by crutches), incorrect positioning of the shoulder during sleep or anesthesia, etc. Clinically, damage to this nerve is characterized by the fact that the patient cannot move his arm to a horizontal level, which is explained by the development of paralysis and atrophy of the deltoid muscle. Looseness appears in the shoulder joint - paralytic subluxation. The sensitivity of the skin of the outer surface of the upper third of the shoulder is also impaired.
Axillary nerve neuropathy can be treated conservatively. It consists of physical therapy and interstitial electrical stimulation. If there is no improvement within six months, an operation is indicated - neurolysis - freeing the nerve from surrounding scar adhesions or its transplantation (transposition). The results of such operations are usually favorable; the sensory function of the nerve is restored before the motor function.
Damage to the musculocutaneous nerve n. musculocutaneus.
The motor fibers that make up the musculocutaneous nerve innervate the biceps, brachialis and coracobrachialis muscles. Sensitive nerve fibers innervate the skin on the outer surface of the forearm. When the musculocutaneous nerve is damaged, atrophy of the biceps brachii, brachialis, and coracobrachialis muscles is noted. There is a loss of the flexion-elbow reflex, as well as a violation of all types of skin sensitivity on the radial surface of the forearm and tenor. Causes and treatment may be similar to those described in the previous section (axillary nerve).
Considering the shoulder joint, it is necessary to talk about the most common traumatic injuries in it, especially in old age. These are intra-articular, fragmentary, comminuted fractures of the head and neck of the humerus with avulsions of These injuries are almost always multicomponent, combining ligament ruptures, muscle damage, fracture-dislocations and displacement of bone fragments.
Therefore, surgical treatment should be comprehensive. Osteosynthesis is always combined with restoration of tendon integrity, reduction of dislocations and, if necessary, joint replacement - endoprosthetics .
The future of shoulder surgery lies in the development of bioengineering technologies. The use of “patch patches” from biocompatible materials for rotator cuff defects, the use of growth factors (PRP - Platelet-Rich Plasma - platelet-rich plasma), expansion of indications for minimally invasive arthroscopic surgery, development of new surgical techniques.
Scheme for using a patch for a defect in the supraspinatus tendon.
Most people with the above diseases of the shoulder joint cannot fully care for themselves. They do not find the right specialist, they are treated by general practitioners, they turn to therapists, neurologists or surgeons. And only an orthopedic traumatologist can help them, for consultations with whom patients come already in chronic and advanced stages. Our clinic offers a full range of examinations and treatments for your joints. Currently, arthroscopy is a minimal risk, the key to successful treatment and predictable recovery of our patients, regardless of age.
The text and illustrations are intended solely to inform about diseases and their treatment options. Do not forget: self-medication can harm your health.
Contact your doctor.
If you have any questions, you can ask them by sending an email to: [email protected] or by making an appointment.
Traumatologist-orthopedist of the National Health Institution "Road Clinical Hospital at Voronezh-1 station of JSC Russian Railways" Genyuk Yuri Vladimirovich
Causes
Subacromial impingement syndrome is a polyetiological pathological condition. This means that compression of the subacromial muscle of the shoulder joint can be caused by a significant number of provoking factors, which include:
- Congenital or acquired (as a result of injury or a destructive pathological process) anatomical features of the acromial process of the scapula. The curved, hook-shaped shape of this structure causes mechanical compression of the subacromial muscle, which increases even when the arm is raised up for a short time.
- The appearance of pathological bone outgrowths (osteophytes) in the area of the junction of the acromial process of the scapula with the clavicle, which leads to compression of the muscle.
- A chronic inflammatory process in the shoulder joint, leading to an increase in the thickness of the connective tissue bursa in the area of the posterior surface and cuff.
- Previous injuries in which there was a violation of the integrity of the tubercle of the humerus or the acromion process of the scapula. Tissue regeneration is often accompanied by the formation of callus, which compresses the subacromial muscle.
- Congenital decrease in the strength of the ligamentous apparatus.
- Pathological decrease in the tone of the striated muscles of the shoulder area due to paralysis, myasthenia.
- Rupture of the connective tissue structures of the ligamentous apparatus of the shoulder, which often accompanies dislocation of the humerus with its head coming out of the glenoid cavity.
- Pathological reduction in size (“wrinkling”) of the joint capsule of the shoulder.
After determining the factor that provokes rotator cuff syndrome, treatment necessarily includes measures aimed at eliminating its subsequent effects.
Prevention
Large loads on the shoulder joint should be avoided. If the work involves performing monotonous movements, you need to give your hand the opportunity to rest. At the first symptoms of the disease, you should immediately consult a doctor and treat the joint. This will allow you to quickly relieve unpleasant symptoms and avoid the development of irreversible processes.
Our clinic has extensive experience in treating such patients. Thanks to our knowledge of modern diagnostic and treatment methods, we successfully treat impingement syndrome not only at the initial stage, but also in advanced cases.
We will help you restore the function of your shoulder joint in a short time and return to your usual active lifestyle.
Kinds
Kinds
With the development of a pathological process against the background of an initial change in the anatomical relationship of the shoulder structures, a primary disease occurs. If compression of the rotator muscle occurs due to a previous injury or pathological process, then secondary subacromial syndrome is diagnosed.
Clinical picture
Clinical picture
This disease mainly occurs in patients over 40 years of age who suffer from constant shoulder pain. They have no previous injuries. Pain in such patients occurs when raising the arm between 70 ° and 120 °, in a “painful arc” (see figure), when forced to move the arm above the head and when lying on the affected side. Symptoms may be chronic or acute. More often than not, it is a gradual, degenerative process that causes impingement, rather than some strong external factor. This is why it is often difficult for patients to name the exact onset of symptoms.
Symptoms
Subacromial shoulder syndrome has quite characteristic clinical symptoms, which include several symptoms:
- Pain caused by raising the arm up. At first it has an unexpressed intensity, but as the disease progresses it can intensify and disturb a person at rest (including during sleep).
- Painful sensations during palpation of the shoulder joint. However, they can spread to the supraclavicular region and down the arm.
- Limitation of mobility in the joint affected by the pathological process, which is often accompanied by intense pain.
Subsequently, subacromial impingement syndrome of the shoulder joint is manifested by thinning (atrophy) of the muscles and ligaments of the shoulder with a pronounced decrease in their tone and strength.
Definition/Description
Diercks et al. define SBS as a collection of non-traumatic, unilateral shoulder problems that cause pain localized around the acromion, usually worsening during or after raising the arm. It is essentially an umbrella term that describes pain caused by any injury to any structure or structures within the subacromial space. Thus, the term includes all conditions associated with subacromial structures: subacromial bursitis, forearm calcification, biceps tendonitis, or rotator cuff tendon degeneration.
Diagnostics
Diagnostics
Additionally, to identify the disease and differentiate it from other pathological conditions, the Neer impingement test is performed, the essence of which is to inject lidocaine into the subacromial process bursa. If compartment syndrome is present, pain after injection is reduced.
Impingement syndrome of the shoulder joint - treatment without surgery
Conservative therapy is prescribed for minor changes in the structures of the shoulder and mild compression of the subacromial muscle. It includes several activities, which include:
- Providing functional rest for the joint.
- The use of non-steroidal anti-inflammatory drugs to reduce the severity of inflammation in tissues.
- Direct injection of glucocorticosteroids (hormonal drugs with a pronounced anti-inflammatory effect) into the area of the acromion process, which is prescribed in a short course no more than once a week.
- Physiotherapeutic procedures, which include magnetic therapy, ozokerite, mud baths, electrophoresis with anti-inflammatory drugs.
- Therapeutic exercise (PT), which is carried out to gradually restore the functional state of the shoulder joint, as well as reduce the degree of compression of the subacromial muscle.
Conservative treatment can be prescribed as monotherapy or to prepare the patient for surgery.
Impingement syndrome of the shoulder joint - surgery
Surgical intervention is prescribed by a doctor if there is severe compression of the subacromial muscle or if there is no desired effect after 4 months of conservative therapy. The main purpose of the operation is to release the pinched muscle (subacromial decompression), for which plastic surgery (acromioplasty) of the tissues and structures of the shoulder joint is performed.
This type of surgical intervention is performed using 2 main techniques:
operation
operation
In modern medical clinics, arthroscopy is the technique of choice, since it does not lead to significant tissue trauma. This shortens the duration of the rehabilitation period and also minimizes the possibility of complications.