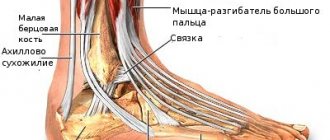
- Ligaments
- Muscles
The articular surfaces of all three bones that form the knee joint are covered with cartilage, which is a hard, elastic material that acts as a shock absorber for the joint. Also, this function is performed by two C-shaped rollers, which also have a cartilaginous structure - the medial (inner) and lateral (outer) menisci. They lie between the femur and tibia, performing a shock-absorbing function and ensuring congruence of the articular surfaces.
Cartilage, joint capsule, synovial fluid...
In the place where the bones are connected to each other, their heads are covered with cartilage , which protects them from friction and impact. Inside the joint there are two menisci , shaped like crescents. They are needed as additional protection of cartilage and bones from mechanical stress.
Cartilage and menisci are located in the so-called joint capsule , inside which synovial fluid . Similar to oil, it lubricates all surfaces of the joint and prevents friction. This is true if there is enough synovial fluid and its viscosity is normal.
In front of the joint is the patella , or kneecap . It is held in place by ligaments and tendons, and covered inside with cartilage. The patella is a kind of shield that protects the internal components of the knee joint from damage.
This is what the knee joint looks like from the inside
How is the knee joint structured? Visual demonstration with detailed explanations:
Synovial joints (joints)
Classification. Examples.
Continuous connections: synarthrosis - between the bones there is a layer of tissue connecting. Fixed, no gap or cavity.
1. Fibrous compounds (syndesmoses) –
1.1. ligaments (spreads from one bone to another) - collagen fibers, low extensibility, very strong,
1.2. membranes – flat, wide, along the cord of bone – radius and ulna, hip joint – pelvic bone – obturator membrane – tibia and fibula;
sutures - skull - serrated suture, flat suture - facial bones, scaly suture - temporal and parietal regions, sutures - zones for shock absorption and shock absorption when walking, jumping. Also serve as areas for bone growth.
1.4. impaction – connection of the tooth root with the walls of the alveoli.
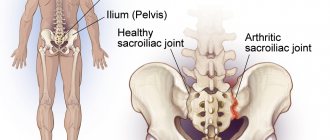
Cartilaginous joints (synchodrosis) are strong and elastic - permanent - sternum and 1 rib, intervertebral discs, temporary - pelvis - ischial, pubic, iliac, sacrum, attachment points of the epiphysis and diaphysis
3. Bone joints (synostoses) – replacement of temporary cartilaginous joints
Indications for ultrasound diagnostics
As a person ages, bones and cartilage deteriorate. When moving, you may feel discomfort, which also occurs with diseases such as arthrosis and arthritis.
It is recommended to undergo an ultrasound of soft tissues and the joints themselves in the following conditions:
- pain and swelling;
- stiffness in the morning (a sign of the onset of many diseases);
- various unpleasant sensations during movements;
- when inflammation and tumor occur (palpable mass formations in the soft tissue area);
- after injury;
- dislocations;
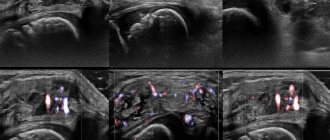
In the photo from an ultrasound machine: the site of rupture of the tendon of the superostriate muscledynamic observation for bursitis;
- with excess body weight (especially important for the joints of the lower extremities);
- newborn children with suspected dysplasia;
- in the presence of already identified diseases (arthrosis, arthritis);
- bone fractures;
- autoimmune and endocrine diseases;
- before puncture;
- suspicion of a Becker cyst or its rupture;
- control of therapy.
Ultrasound normal: what does the echographic picture show?
Subdeltoid bursitis of the shoulder joint (ultrasound image)Synovial membrane: echogenic, difficult to differentiate from connective tissue;
- Cartilage: anechoic, location parallel to the bone surface;
- Bone: highly echogenic, gives an acoustic shadow;
- Tendons: echogenic when examined at a right angle, when examined at other angles - hypoechoic;
- Muscles: hypoechoic; characterized by a feathery echostructure on a longitudinal section and a spotted echostructure on a transverse one;
- Effusion: anechoic or hypoechoic.
Some ultrasound signs of joint pathologies
Pannus – erosive lesions on the articular surface.
Synovitis is an effusion in the joint cavity, characterized by hypoechoic thickening of the capsule.
True bone erosion is a permanent change in the integrity of the bone surface.
Tendinitis is a hyperechoic tendon with a hypoechoic contour around it.
Types of joints
Joints can be divided into groups depending on the shape and number of articulating surfaces or their function - the number of axes around which the joint can produce movements. The following forms of movements in the joints are distinguished.
1. Movements around the frontal axis: decreasing the angle between the articulating bones - flexion, flexio, and increasing the angle between them - extension, extensio.
2. Movements around the sagittal axis: approaching the median plane - adduction, adductio, and moving away from it - abduction, abductio.
3. Movements around the vertical axis: rotation, rotatio, outward rotation, supinatio, inward rotation, pronatio, and circular rotation, circumductio, in which the rotating segment of the limb describes a cone.
The range of motion in the joints is related to the shape of the articulating surfaces. If one surface is small and the other is large, there is a large range of motion in that joint. On the contrary, in joints with approximately the same length of articular surfaces, the range of motion is small. In addition, the range of motion in the joints is related to the degree of fixation by ligaments and muscles.
The shape of the articular surfaces is conventionally compared with geometric bodies (sphere, ellipse, cylinder, etc.). Therefore, they are classified by shape and the following joints are distinguished: flat, spherical, ellipsoid, trochlear, condylar, cylindrical, saddle. Based on the number of axes, multiaxial, biaxial and uniaxial joints are distinguished. The shape of the articular surfaces of the joints also determines their functional mobility and, consequently, the number of axes. Therefore, according to the shape and number of axes, the following types of joints can be distinguished: 1) uniaxial - block-shaped, cylindrical; 2) biaxial - ellipsoidal, saddle-shaped; 3) multiaxial - spherical, flat. Movements in a joint determine the shape of its articular surfaces.
1. Uniaxial joints. The trochlear joint, ginglymus, has a transversely lying cylinder on one of the articular surfaces, and on the other there is a notch, a groove in which the cylinder lies. Movements in such a joint are possible only around the frontal axis - flexion and extension. An example of uniaxial block joints is the interphalangeal joints. A type of trochlear joint is a helical joint, articulatio cochlearis, in which the groove on the articular surface is located somewhat obliquely relative to the plane perpendicular to the axis of rotation. As this furrow continues, it forms not a circle, but a screw. These are the ankle-foot and elbow joints. This group also includes the cylindrical rotary joint, articulatio trochoidea, where the axis of rotation runs along the length of the bone. Around the vertical axis, rotation occurs inward - pronation and outward - supination. An example is the radioulnar joint or the articulation of the atlas with the axial vertebra. Rotation in the latter occurs around the odontoid process.
2. Biaxial joints. The ellipsoidal joint, articulatio ellipsoidea, is close to an ellipsoid in shape of the articular surfaces. In this joint, movements around two axes are possible: frontal - flexion and extension, sagittal - abduction and adduction. In biaxial joints, movements are possible when circular rotation, circumductio, is carried out. An example is the radiocarpal or atlas-occipital joints. Biaxial joints also include saddle joints, articulatio sellaris, the articular surfaces of which resemble the shape of a saddle. The movements in this joint are the same as in the elliptical joint. An example of such a joint is the carpometacarpal joint of the thumb. The condylar joint, articulatio condylaris, also belongs to the biaxial joint (in the shape of its articular surfaces it approaches an ellipsoid). In such a joint, movements around two axes are possible. An example is the knee joint.
3. Multiaxial joints. Ball-and-socket joints, articulatio spheroidea (cotylica), have the greatest freedom of movement. They allow rotation around three mutually perpendicular axes: frontal, sagittal and vertical. Around the first axis there is flexion and extension, around the second - abduction and adduction, around the third - outward and inward rotation. Circular rotation is possible in the ball and socket joint. An example of such a joint is the shoulder joint. If the articular surface is larger than a semicircle, as is observed in the hip-femoral joint, where the head of the femur is deeply covered by the articular cavity of the pelvic bone, then such a joint is called cup-shaped, articulatio cotylica. This same group of joints includes flat joints, articulatio plana, where the articular surfaces are slightly curved and represent segments of a circle with a large radius. An example is the intervertebral joints or the rib head joint.
If two bones take part in the formation of a joint, then such joints are called simple, articulatio simplex, if three or more are called complex, articulatio composita. An example of the first joint is the shoulder, an example of the second is the elbow. Combined joints are a collection of several individual joints in which movements occur simultaneously. For example, it is impossible to move in one temporomandibular joint without movement in the other.
A number of factors are important in fixing joints: adhesion of articular surfaces, strengthening them with the capsular-ligamentous apparatus, traction of muscles and tendons attached to the circumference of the joints.
The joints have pronounced individual, age and gender characteristics. The amount of mobility in bone joints depends on the individual structural features of these joints. It is not equally expressed in people of different ages, genders and degrees of fitness.
Human joint diseases
According to WHO statistics, at least every seventh person around the world is familiar with joint pain, and among the age group from 40 to 70 years old, certain problems can be encountered in 50% of cases, and over 70 years old - in 90% of cases. This prevalence of musculoskeletal diseases is associated with many factors:
- low physical activity, in which the joints do not function and, accordingly, do not receive the proper amount of nutrition through the bloodstream;
- uncomfortable, too tight shoes and clothes that limit the functionality inherent in nature;
- poor heredity as one of the risk factors for the development of pathologies associated with joints;
- dramatic changes in temperature, including both overheating and hypothermia;
- infectious processes in the body, which often provoke complications associated with the functioning of the joints;
- injuries that reduce the functionality of the musculoskeletal system;
- old age.
Experts say that maintaining healthy joints is quite possible if you take timely measures to prevent diseases. You should avoid injuries and damage, strengthen your immune system, and include sports in your daily schedule. Yoga can be an excellent option, because static loads well strengthen the muscles and ligaments that hold the joints. Take care of your health in advance - this natural resource is much easier to preserve than to replenish!
What can hurt a joint?
There are no nerve endings in cartilage and menisci, so they cannot hurt. In fact, there is nothing in the joint that could hurt in the usual sense. The nerves do not approach the bones, but rather the periosteum - thin membranes covering the outside of the bone. Therefore, a person experiences pain when a bone is damaged. What happens if there is no fracture?
In the absence of a fracture, the source of pain may be the ligaments surrounding the knee joint and holding the menisci inside. In addition, the nerve endings approach the joint capsule, which can also cause pain.
Cartilage does not hurt: there are no nerve endings in them
When a mechanical injury occurs, the following occurs:
- the joint is injured, the ligaments swell;
- the body initiates the healing process - drives blood to the damaged area;
- the skin around the joint turns red, the joint swells;
- Synovial fluid stops circulating freely and puts pressure on the nerves in the joint capsule, which leads to increased pain.
After some time, the small ligaments heal, the swelling subsides, the fluid begins to circulate again - the pain disappears. This happens if only small ligaments are damaged, while the large ones and the meniscus remain intact. If the meniscus is damaged, the situation develops differently, since the person does not experience pain, but the structure continues to be damaged.
Over time, the meniscus is damaged even more, the cartilage around it also becomes deformed, finding itself in unfavorable conditions. Their surface gradually wears away, which leads to friction of the bones, irritation of the nerve endings in the periosteum and, as a result, pain. This is how arthrosis of the knee joint develops - a disease that is rarely diagnosed at an early stage.
When a person is prescribed treatment for arthrosis or osteoarthritis, the condition of his joints already leaves much to be desired. There is almost certainly not enough synovial fluid in the joint capsule, and in conditions of insufficient lubrication, the cartilage quickly dries out, cracks and wears out. The situation can be corrected with intra-articular injections of the synovial fluid substitute Noltrex.
Noltrex is like the missing brick in building a house
The drug is injected into the joint capsule and evenly distributed over the cartilaginous surfaces. Due to its high molecular weight, it does not penetrate inside, but lingers there, performing the function of a lubricant. Noltrex does not contain animal proteins, therefore it does not cause allergies and is not recognized by the body's immune cells. A few injections are enough to restore the physiological characteristics of the joint for a year, a year and a half, or even two, and therefore relieve a person from pain.