Knee joint[edit | edit code]
Knee-joint
formed by the distal end of the femur and the proximal end of the tibia. The proximal end of the tibia also forms the tibiofibular joint with the fibula, allowing some sliding of these two bones relative to each other during pronation and supination of the foot. The patella is adjacent to the distal end of the femur, forming the femoral-patellar joint, which plays an important role in the normal functioning of the knee joint.
Biomechanics of the knee joint on x-ray
The knee joint is a condylar joint
, and movements in it occur around two axes.
The main movements:
flexion and extension are carried out around the frontal axis (Fig. 3.1), but in addition, during flexion, the tibia rotates inward, and during extension, outward.
The relatively shallow knee joint is strengthened by several ligaments. Tibial (medial) collateral ligament
strengthens it on the medial side, preventing excessive valgus displacement of the tibia, and
the fibular (lateral) collateral ligament
strengthens it on the lateral side, preventing excessive varus displacement of the tibia.
Figure 3.1.
Range of motion in the knee joint.
- Valgus position of the lower leg
- displacement of the distal part of the lower leg laterally (as with an X-shaped curvature of the legs). - Varus position of the leg
is a medial displacement of the distal part of the leg (as with an O-shaped curvature of the legs).
Anterior cruciate ligament
- a ligament that runs inside the knee joint from the anterior edge of the tibia to the posterior edge of the femur; limits the forward displacement of the tibia relative to the femur, as well as the rotation of the tibia.
The anterior and posterior cruciate ligaments intersect within the knee joint. The anterior cruciate ligament prevents the tibia from moving forward relative to the femur; The posterior cruciate ligament prevents posterior displacement of the tibia. Because the cruciate ligaments provide joint stability during tibial rotation, injury to them often results in anterolateral or anteromedial rotational instability of the knee.
Anterolateral knee instability
occurs when the lateral condyle of the tibia slips forward; anteromedial instability - when the medial condyle of the tibia slips forward. These types of rotational instability of the knee severely limit physical activity.
Intra-articular cartilages - menisci
- increase the articular surface of the tibia and act as a shock absorber, protecting the tibia and femur from impacts. The medial meniscus is somewhat elongated in the anteroposterior direction and is firmly attached to the tibia and tibial collateral ligament. The lateral meniscus, on the contrary, has a more rounded shape and has greater freedom of movement, since it is not attached to the fibular collateral ligament. Meniscus injuries are difficult to treat because menisci are made of cartilage, and cartilage lacks a blood supply and therefore does not heal well.
Extension of the leg at the knee joint occurs due to the contraction of the strong quadriceps femoris muscle. It consists of the rectus femoris muscle, as well as the vastus medialis, intermedius and vastus lateralis muscles, and is attached by a common tendon to the patella and to the anterior surface of the tibia.
Menisci
- intra-articular cartilages of the knee joint are crescent-shaped.
Quadriceps femoris
- a muscle on the front of the thigh, consisting of the rectus femoris, as well as the vastus medialis, intermedius and vastus lateralis muscles.
Synovial bursa
- a fluid-filled cavity that serves to reduce friction between anatomical structures.
Injuries to this muscle can occur during contact sports.
Flexion of the leg at the knee joint is ensured by the posterior group of thigh muscles, consisting of the semitendinosus and semimembranosus muscles on the medial side and the biceps femoris muscle on the lateral side. These tendons are often damaged during sprinting.
Around the knee joint there are several synovial bursae that reduce tendon friction. These include the suprapatellar, prepatellar, deep and subcutaneous infrapatellar bursae. The suprapatellar bursa communicates with the cavity of the knee joint. With excess fluid in this bursa, the knee joint becomes noticeably swollen. The prepatellar bursa is located in front of the joint and often suffers from bruises.
Restoration of joints after injuries and operations
Restoration of joints after injuries and operations
DEVICES FOR PASSIVE JOINT REHABILITATION
To eliminate joint stiffness after injuries and operations, devices for robotic mechanotherapy of limbs of the Ormed Flex brand are used. The use of these devices helps to quickly reduce swelling, as well as the outflow of fluid from the joint.
"Ormed Flex" are used in rehabilitation and significantly reduce the recovery time on devices for contractures of various origins: after prolonged immobilization in a cast, after injuries and burns, in some neurogenic diseases. This reduces swelling and pain.
The main points suggesting the use of passive movements during rehabilitation are:
- significant deterioration in joint mobility in the absence of movement, the occurrence of contracture;
- indirect improvement in the nutrition of articular cartilage due to physical activity, stimulating the movement of synovial fluid inside the joint;
- the ability of the synovial membrane to slide freely over the surface of the joint and have a high degree of adhesion to the adjacent cartilage tissue;
Continuous passive movements:
- improve nutrition and metabolism of joints;
- stimulate the formation of hyaline cartilage cells on the articular surface from undifferentiated mesenchymal tissue, which leads to joint regeneration. The process occurs much faster than with joint immobilization or active movement therapy;
- prevent the formation of intra-articular adhesions and post-traumatic arthrosis;
- accelerate the healing of ligaments and tendons in the limb;
- prevent muscle atrophy, in contrast to immobilization of the joint with plaster casts;
- promote rapid restoration of cartilage and soft tissues of the joint;
- contribute to the rapid removal of swelling.
During the procedure, the patient is able to completely relax the injured limb. The speed and range of movements are set very precisely; the doctor can increase the angles of development gradually, focusing on the patient’s capabilities and well-being.
That is why the use of robotic therapy devices is the most optimal method.
Ormed Flex simulator is that the characteristics of the exercises (speed, amplitude, duration) are selected strictly individually for each patient, depending on the underlying disease. Thanks to this, the procedure is absolutely painless and safe, which is a necessary condition for muscle relaxation. The absence of pain sets the patient up to continue rehabilitation, increases range of motion, and reduces swelling.
Ormed Flex devices are a new product made in Russia. They were developed in collaboration with practicing orthopedic traumatologists, passed technical and clinical tests in existing medical centers and fully comply with the requirements for modern equipment. They are produced by the Orbita Research and Development Enterprise , which has been supplying the market with devices of the ORMED , known for their quality, for 30 years.
ADVANTAGES OF THE DEVICES:
- mobile in any conditions, thanks to the compact and lightweight design;
- for the production of key mechanisms and components, materials and components produced in Japan and Germany are used;
- the experience of leading European manufacturers was taken into account during the development;
- passed life tests through continuous long-term operation corresponding to 10 years of practical use;
- easily controlled via an LCD remote control with a simple and intuitive interface;
- parameters are configured individually for each patient;
- it is possible to save settings for 250 patients in the device’s memory, as well as use a USB drive;
- ease of fixation of the injured area;
- painless process of joint development procedure;
- possibility of changing limbs;
- resistance load switching function.
The Ormed Flex line includes devices for robotic mechanotherapy:
“Flex F01” – for the knee and hip joints;
“Flex F02” – for the ankle joint;
“Flex F03” – for the elbow joint;
“Flex F04” – for the shoulder joint;
“Flex F05” – for the wrist joint.
ATTENTION! NOW A NEW UNIQUE DEVICE ORMED FLEX F01 ACTIVE
A biofeedback device for passive and active-passive joint development is indicated for restoring range of motion after a stroke.
Features of the device:
- Passive joint training without pain;
- Active training with control of coordination and muscle tone;
- During active training, muscles can work in both concentric and eccentric modes;
- The ability to accurately dose the load on the muscles;
- Ensuring movement taking into account physiological characteristics;
- Simple and convenient control panel with LCD screen;
Possibility of using regular flash cards to record the procedure parameters of each patient.
Self-esteem increases, fears go away, the patient willingly exercises on the device. This promotes rapid recovery of the body.
Indications for the use of devices for robotic mechanotherapy “Ormed Flex” in clinical practice:
- sprains and bruises of the joints of the upper and lower extremities;
- conditions after intra-articular interventions (arthroscopy, arthrotomy, etc.);
- surgical interventions on the ligamentous apparatus and soft tissues in the joint area;
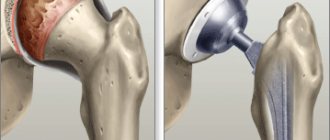
- restoration of motor function after endoprosthetics operations;
- stimulation of reparative processes and restoration of motor function of joints.
Contraindications to the use of devices are:
- acute period of the inflammatory process;
- spastic paralysis;
- unstable osteosynthesis.
This equipment is included in the equipment orders:
Order of the Ministry of Health of the Russian Federation dated July 31, 2020 No. 788n “On approval of the Procedure for organizing medical rehabilitation of adults.”
Order of the Ministry of Health of Russia dated December 29, 2012 No. 1705n “On the procedure for organizing medical rehabilitation.”
Order of the Ministry of Health of the Russian Federation dated August 22, 2019 No. 665n “On approval of the list of products for retrofitting (providing) children’s clinics and children’s outpatient departments of medical organizations subordinate to the executive authorities of a constituent entity of the Russian Federation, and (or) medical organizations of the municipal healthcare system located in territory of a constituent entity of the Russian Federation."
Order of the Ministry of Health of the Russian Federation dated December 31, 2016 No. 260n “On approval of the departmental target program “Development of the material and technical base of children's clinics and children's outpatient departments of medical organizations.”
Advantages of devices for robotic mechanotherapy:
- made of wear-resistant soft materials;
- mobile in any conditions, thanks to compact and lightweight equipment;
- made of high-quality materials and components, which indicates the reliability of the equipment;
- easy to control via remote control, have simple and intuitive software;
- parameters are configured individually for each patient;
- it is possible to save settings for 250 patients in the device’s memory, as well as use a USB drive;
- ease of fixation of the injured area;
- painless process of joint development procedure;
- possibility of changing limbs;
- resistance load switching function.
Where are Ormed Flex devices used:
- in rehabilitation centers;
- in rehabilitation departments of hospitals;
- in hospitals and rehabilitation departments for war veterans;
- in neurological departments;
- in trauma departments;
- in sanatorium and resort institutions;
- in surgical departments;
- in exercise therapy rooms;
- in sports medicine;
You will find detailed information about our products on the website: www.ormed.ru
LLC NVP "Orbita", 450095, Ufa, st. Central, 53/3, Tel., 281-45-13.8-800-700-86-96 (calls within Russia are free) e-mail
We invite doctors and nursing staff to train under the program “Working on devices of the ORMED series.”
Send applications for training to e-mail: [email protected]
Details by phone.
Palpable anatomical landmarks[edit | edit code]
Medial surface
- Tibial collateral ligament
- Medial joint line
- Medial meniscus
Lateral surface
- Peroneal collateral ligament
- Lateral line of the joint
- Lateral meniscus
Front surface
- Quadriceps tendon
- Patella
- Patellar ligament
Rear surface
- Popliteal fossa
- Biceps femoris tendon
- Semitendinosus tendon
- Semimembranosus tendon
muscles involved in various types of movement of the lower end
Laboratory lesson
"Muscles of the lower limb"
The muscles of the lower limb produce movements at the hip, knee, ankle and foot joints.
Muscles
producing movements in the hip joint
According to three mutually perpendicular axes of rotation passing through the center of the hip joint, the following movements can be made in this joint by the thigh with the pelvis fixed, and with it the entire leg :
- flexion and extension, i.e. movement forward and backward;
- abduction and adduction;
- pronation and supination;
- circular motion (circumduction).
When securing the hip or the entire leg, the muscles produce movements of the pelvis: forward, backward, sideways and turns to the right and left. To carry out these movements, there are six functional muscle groups in the hip joint.
Hip
flexion The muscles that produce hip flexion at the hip joint include the muscles that cross the transverse axis of this joint and are located in front of it. These include:
1) iliopsoas
2) tailoring
3) tensor muscle of the fascia lata;
4) comb;
5) rectus femoris muscle
Hip
extension In hip extension, muscles take part that also cross the transverse axis of the hip joint, but are located behind it. These muscles go both from the pelvis to the thigh and from the pelvis to the lower leg. These include:
- gluteus maximus;
- biceps femoris muscle;
- semitendinosus;
- semimembranous;
adductor magnus
Hip
abduction The hip abductor muscles cross the sagittal axis of the hip joint and are located on its lateral side. They are attached mainly to the greater trochanter. These muscles include:
- gluteus medius;
- gluteus minimus;
- pear-shaped;
- internal obturator;
- twins;
6) tensor fascia lata muscle
Hip
adduction Hip adduction is carried out by muscles that cross the sagittal axis of the hip joint and are located medial to it. These include:
- comb;
- thin;
- long adductor;
- adductor brevis;
- adductus magnus
Supination
of the hip
The muscles that supinate the hip, except for the iliopsoas, cross obliquely the vertical axis of the hip joint. The iliopsoas muscle supinates the thigh due to the special location of the lesser trochanter (not only anteriorly, but also medially). The muscles that supinate the thigh include:
- iliopsoas;
- quadratus femoris;
- gluteal muscles, of which the medius and minimus supinate the thigh only with their posterior bundles;
- tailoring;
- obturator internus and obturator externus muscles;
- pear-shaped;
- twin.
Pronation
of the hip
The group of pronator muscles of the hip is relatively small. These include:
- tensor fasciae lata muscle
- anterior bundles of the gluteus medius muscle
- anterior bundles of the gluteus minimus muscle
semitendinosus, semimembranosus and gracilis muscles
Circular hip movement
In the hip joint, all muscle groups located near it produce, acting in turn.
Muscles
producing movements in the knee joint
muscles surrounding the knee joint produce, with the thigh fixed (with proximal support), flexion, extension, pronation and supination of the lower leg, and with the lower leg fixed (distal support), movement of the thigh forward, backward, pronation and supination.
Flexion
of the lower leg
The flexor muscles of the lower leg cross the transverse axis of the knee joint and are located behind it. These include the following muscles:
- biceps femoris
- semitendinosus
- semimembranosus
- tailoring
5) thin
- popliteal
- gastrocnemius (part of the triceps surae muscle)
plantar
Extension of
the lower leg
is involved in extension of the lower leg ,
crossing the transverse axis of the knee joint in front of it. This is one of the most massive muscles in the human body. It is located on the front surface of the thigh and has four heads:
- rectus femoris muscle;
- vastus lateralis muscle;
- vastus medialis muscle
- vastus intermedius muscle.
Pronation
of the lower leg
Pronation of the lower leg at the knee joint is possible only as it bends, i.e. as the collateral ligaments (tibial and fibular) relax. The muscles that produce pronation of the lower leg are all those located behind and on the medial side of the knee joint:
- semitendinosus
- semimembranosus
- tailoring
- thin
- medial head of the gastrocnemius
- popliteal
Supination of
the lower leg
Supination of the lower leg at the knee joint (like pronation) is possible only as it bends. The muscles located on the lateral side of the knee joint serve as supinators of the lower leg:
- biceps femoris
- lateral head of the gastrocnemius. Thus, the pronator muscle group is much stronger than the supinator muscle group.
Muscles producing
movements the foot
slight adduction and abduction as it flexes, pronation and supination.
Flexion
of the foot
The flexor muscles of the foot cross the transverse axis of the ankle joint and are located posterior to it on the posterior and lateral surfaces of the lower leg. These muscles include:
- triceps surae muscle;
- plantar;
- posterior tibial;
- flexor pollicis longus;
- flexor digitorum longus;
- long fibular
- short fibula.
Extension of
the foot
The extensor muscles of the foot, like the flexor muscles, cross the transverse axis of the ankle joint, but are located in front of it, constituting the anterior group of muscles of the lower leg. These include:
- anterior tibial;
- extensor digitorum longus;
- extensor pollicis longus.
Foot adduction
- There are no special muscles involved in adducting the foot; this movement is carried out according to the rule of parallelogram of forces with simultaneous contraction of the following muscles:
- anterior tibial
- posterior tibial
Foot
abduction The muscles involved in foot abduction are located on the lateral side of the vertical axis of the ankle joint. These include:
- peroneus brevis muscle
- peroneus longus muscle
Pronation
of the foot
In pronation of the foot, muscles located on the lateral side of the sagittal axis around which this movement occurs take part. The following muscles pronate the foot:
- long fibula;
- short fibula;
- third fibular
Supination of
the foot
Supination of the foot involves muscles that cross the sagittal axis around which this movement occurs and are located medial to it. The following muscles supinate the foot:
- anterior tibial
- extensor pollicis longus. The alternating action of muscle groups passing near the joints of the foot and coming to it from the lower leg causes its circular movement.
Muscles that
produce movements of the toes The
movements of the toes involve the muscles that move from the lower leg to the foot, and the muscles of the foot itself. The muscles located on the plantar surface of the foot flex the toes, and the muscles located on the back of the foot extend them. The muscles of the foot itself include those that both begin and attach to the foot. They are quite numerous and can be divided into two groups: the muscles of the plantar surface of the foot and the muscles of the dorsum of the foot.
Read also[edit | edit code]
- Knee orthoses
- Hyperextension of the knee joint
- Femoral-patellar syndrome
- Knee sprain (treatment)
- Meniscus tear: symptoms and treatment
- Osteochondrosis dissecans
- Injuries and damage to the quadriceps femoris muscle
- Quadriceps tendon rupture
- Patellar ligament rupture
- Avulsion of the tibial tuberosity
- Knee ligaments Collateral ligament rupture
- Anterior cruciate ligament rupture
- Posterior cruciate ligament rupture
- Chondromalacia patella: symptoms and treatment
Muscles of the knee joint
In the knee joint, according to the two main movements - flexion and rotation - the presence of mainly a group of flexors and extensors is necessary; rotation can be performed by those muscles from this group that are attached linearly in the longitudinal direction and the resultant of which crosses the longitudinal axis of the leg. Here, just as in the hip joint, we must distinguish between the action of the muscles at the top and at the bottom support. Of all the muscles of the knee joint, the extensors should be the strongest, since during changes in body position and movements they take the greatest part in balancing the torso and in the movement of the lower leg.
The upper and lower limbs of a person, as has already been described in the section of the skeletal system, undergo movement (twisting around the longitudinal axis) during their development. During the first period of development, both limbs are located with the extensor surfaces lateral and the flexor surfaces medially. In the further course of development, both limbs change their position, turning around their longitudinal axes in the opposite direction. Thus, on the shoulder and forearm the extensor surface is turned posteriorly, and on the thigh and lower leg - anteriorly. The radius and big toe lie laterally, and the tibia and big toe lie medially. Therefore, the muscle groups in both limbs are located differently: while the elbow extensors, which produce backward flexion in this joint, are located on the posterior surface of the upper limb, the knee extensors are located in the front. Therefore, the anterior group of muscles of the knee joint will be extensor, and the posterior group will be flexor.*
* (This movement of the bones of the limb in embryonic life makes it possible to understand the apparent contradiction in the terminology of the muscles of the limbs. In most cases, flexors are the muscles that bend forward, and extensors are the muscles that bend backward. On the lower limb, depending on the above-mentioned movement, we have extensors in the hip joint located on the posterior surface; in the knee and in the joints of the toes - on the front surface. As for the ankle joint, the forward flexion is called dorsiflexion, and the backward flexion is called plantar flexion. The muscles that produce these movements are named not on the basis of the action they produce, but on the basis of their location.
)
Knee flexors and extensors
Quadriceps femoris
, or
extensor leg
(m. quadriceps femoris, sm extensor cruris, Fig. 61-c, 7, 6). This muscle is primarily involved in the extension of the lower leg. Occupies almost the entire front surface of the thigh. There is disagreement regarding the number of heads of this muscle. German anatomists consider its most superficial part - the long head, or rectus femoris (n. rectus femoris, Fig. 61-6) - to be a separate independent muscle. In the rest of the muscle mass, some distinguish only two wide heads - the outer (vastus externus, Fig. 62-3) and the internal (vastus internus, Fig. 62-2). Other anatomists still distinguish the third, middle (vastus intermedius, sm cruralis, Fig. 62-4). French anatomists consider the extensor leg muscle to be a quadriceps muscle, including the rectus femoris muscle. The combination of these four ulnar muscles into one muscle allows us to compare it with the elbow extensor, if even there we take the fourth ulnar muscle not as an independent muscle, but as the fourth head of the triceps elbow extensor (P. Lesgaft).
In this manual, we will adhere to the views of French anatomists, considering this muscle as a quadriceps extensor of the tibia, consisting of four heads. One of the heads, superficial, passes through two joints: the femoral and knee; and the rest are related to only one knee joint.
Superficial head - rectus femoris muscle
(m. rectus femoris, Fig. 61-6), as already indicated when analyzing the femoral joint, has an upper attachment on the ilium with two well-developed tendons: one begins on the lower anterior spine of the ilium, passes in a straight direction into the muscular body; the second goes in an arcuate manner, starting from the roughness around the acetabulum and partly from the bursa ligament of the femoral joint. Both of these tendons, joining into one, form an arch that strengthens the femoral joint, especially during extension of the torso, when the head of the femur protrudes most forward and tends to stretch the anterior wall of the femoral joint bursa. The fibers of the rectus femoris muscle, gathering together, form a spindle-shaped muscle body with a clear pinnate arrangement of fibers. A few centimeters above the base of the patella, it passes into a strong flat tendon, which, connecting with the other heads of the femoral extensor, is attached to the upper edge of the patella more superficial than all the other heads. The patellar bone, however, cannot be considered as the site of application of the force of this most developed muscle of the human body, since it is a sesamoid bone embedded in the thickness of the tendon of the muscle, and is important for increasing the angle at which the muscle approaches the bone at the site of application of its force. The place of attachment of the rectus femoris muscle should be considered the tibial tubercle, to which the muscle tendon approaches in the form of its own ligament of the patellar bone (lig. patellae, Fig. 61; 62-5), attached to the tibial tuberosity.
The patella bone does not connect directly to neighboring bones and has no direct relationship to the joint; it is strengthened by ligaments that extend from both sides of the femoral condyles and merge with the lateral parts of the quadriceps extensor tendon. Between the tendon of this muscle, in other words, the patellar bone ligament and the tibia, there is a mucous bursa (bursa mucosa subpatellaris, s. infrapatellaris, Fig. 72-24) to reduce friction. This bursa never communicates with the joint, since it is separated from its synovial membrane by a large amount of fat, which here forms the synovial folds of the joint, the so-called pterygoid ligaments (lig. ala-ies). Between the tendon and the femur above the patella there is also a mucous bursa (bursa mucosa supra-patellaris), adjacent directly to the joint bursa or to the synovial protrusion that sometimes exists here, with which it often communicates.
Superior attachment of the broad extensor head of the tibia
(vastus externus, Fig. 61-7, 62-3) starts from the outer surface of the base of the greater trochanter, from the outer rough line of the femur, from the outer intermuscular septum and to some extent from the outer surface of the thigh. From these attachment points, the fibers descend down, the upper ones are completely vertical, and the lower ones are arched, surrounding the femur. This entire attachment occupies the upper two-thirds of the femur; Below, the outer head lies free, and below it, the fibers of the middle head begin from the bone.
Internal wide head
(vastus internus, Fig. 62-2, 61-8) the extensor of the tibia is smaller than the outer one, it starts from the surface of the bone with a whole series of fibers connecting it to the middle head, which makes many consider these two heads to be one. One has only to cut this connection below, and then the division of their attachments into bones is clearly revealed: they are separated from each other by the entire inner surface of the thigh, which here is completely free of muscle attachments. The superior attachment of the vastus medialis extensor head begins at the medial lip of the linea aspera of the femur, almost at the insertion of the femoral bursa. Its fibers go from above and behind, down and forward, surrounding the femur.
Medium wide (intermediate) head
(vastus intermedins s. cruralis, Fig. 62-4) extensor leg, covered on both sides by the just described external and internal heads, is located on the outer and anterior surface of the femur. It starts from these two surfaces and receives more fibers from the outer and inner edges of the femur. Its middle fibers descend straight down, and the outer and inner ones go obliquely to the midline of the limb, to the tendon stretch, connecting to the tendons of the outer and inner heads.
The tendon, formed by all these muscle heads, is attached along the outer, inner and upper edge of the patellar bone, merging with the ligaments that strengthen it and with the aponeurosis. Next, the tendon (Fig. 62-5) passes through the patellar bone and continues in the form of its own ligament of the patellar bone, attached to the tubercle of the tibia. The fusion of the tendon on top of the patellar bone with the ligaments that strengthen it and with the aponeurosis makes it possible to extend the knee joint even if the patellar bone’s own ligament is damaged.
Deeper than the wide middle head of the extensor leg, from the anterior surface of the femur, the muscle begins in the form of several bundles or in the form of a continuous muscle plate, the fibers of which end on the bursa ligament of the ankle joint. This muscle is called the knee joint muscle
(m. articularis genu, s. subcruralis); its fibers protect the bursa ligament from pinching.
All four extensor heads of the tibia, approach the lower leg from the inside, outside and directly from above, with the upper support they will produce extension in the knee joint, and with further contraction through the rectus femoris muscle they can also participate in flexing the thigh forward (Fig. 60-4, 5 , 9). With lower support on both legs, the rectus femoris muscle flexes (tilts) the pelvis forward. With lower support on one leg, it tilts the pelvis forward and towards the support. The three wide extensor heads of the tibia produce only extension of the knee joint. Isolated contraction of the wide external and internal heads causes lateral movement of the patella bone, while the joint contraction of both heads destroys this movement. When all four heads contract, some movement of the patella bone outwards is caused, since the middle wide head, when contracting, enhances the action of the outer head.
The quadriceps extensor muscle of the leg is the strongest muscle in the human body, but its action is manifested with varying strength and in different ways, depending on the position of the body. In a calm vertical position of the body, the quadriceps extensor of the tibia does not take any active part, since in this case the knee is extended under the influence of the gravity of the body, and the line of the center of gravity of the body passes either through the knee joint itself or in front of it. The cruciate ligaments of the joint and the knee flexor muscles will resist further extension (hyperextensio). But as soon as a slight bending of the knees occurs in this position, the quadriceps extensor muscle with all its parts should help balance the body, since the line of the center of gravity in this case passes behind the knee joint.
When walking, the muscle we are considering is greatly involved. During walking, the weight of the body is transferred alternately from one limb to another, with one leg moving, being free, and the other holding the weight of the whole body - the supporting leg. The quadriceps extensor does the most work in the supporting leg at the moment the weight of the body is transferred to it, while in the free leg it is mostly relaxed and contracts very quickly before the moment the leg is placed on the ground.
In a sitting position, with the knee bent, the long head of the quadriceps extensor can exert the greatest force in flexing the leg at the hip joint, since its tendon in this case approaches the pelvis at a right angle and the muscle is in some degree of stretch. When moving from a sitting to a standing position, the quadriceps extensor muscle lifts the entire torso. In general, it acts most powerfully as a knee extensor when the leg is extended at the hip joint and bent at the knee; as a hip flexor - when the leg is bent at the knee. In both cases, it is preliminarily stretched to a certain extent and therefore from this position it can exert the greatest force.
Innervation: femoral nerve (n. femoralis, LII-IV).
The flexors of the knee back with the upper support are the muscles we have already described - biceps, semitendinosus and semimembranosus; these muscles pass in the same way as the long head of the quadriceps extensor leg muscle - the rectus femoris muscle - through two joints; they are also joined by the popliteus muscle, which is related only to the knee joint.
The first three muscles apply their force on the front surface of the tibia, wrapping this bone in a loop. R. Fick
believes that the main muscles that flex the knee are only the short head of the biceps and popliteus, due to the fact that all the others pass through two joints and act simultaneously on the femoral joint.
Hamstring muscle
(m. popliteus, Fig. 67-1) with its upper attachments it begins from the external condyle of the femur, immediately under the beginning of the external collateral ligament of the knee joint. Its origin in the form of a flat tendon runs medially from the fibrous bursa of the joint and resembles to some extent the relationship to the bursa of the joint of the tendon of the long head of the biceps brachii muscle. Passing between the synovial and fibrous bursa, the tendon of the popliteus muscle comes into contact with the outer semicircular cartilage of the knee joint and forms an arch for it, preventing it from slipping out under increased pressure from the overlying parts, which could happen since the cartilage lies freely in the joint cavity, not connected with a joint capsule. The synovial membrane of the joint fuses with the tendon of the popliteus muscle and, due to the movement of the tendon, forms a synovial protrusion, which, following the movement of the tendon, descends down to the upper joint of the tibia with the fibula; in some cases there is even communication between these two joints. At the level of the knee joint, the tendon of the popliteal muscle is directed to the midline of the limb and, emerging from under the fibrous capsule, sends two extensions to it: one goes upward - to the oblique popliteal ligament (lig. popli-teum obliquum, Fig. 67-5), forming the outer part of the arcuate popliteal ligament (lig. popliteum arcuatum, Fig. 67-9), and the other goes down to the head of the fibula (retinaculum lig. arcuata, Fig. 67-10). Coming out from under the fibrous bursa already in the form of a muscle belly, the popliteal muscle is located along the posterior surface of the tibia, reaches the level of the oblique (otherwise called popliteal) line of this bone and is attached along the inner edge of the tibia, above the popliteal line.
With upper support and a fixed hip, the popliteus assists in flexion and mediates medial rotation of the tibia. With lower support and a fixed shin, in some positions it helps flexion in the knee joint produced by the calf muscle, for example, at the moment of transition of the body from a standing to a sitting position.
Innervation: tibial nerve (n. tibialis, LIV-V and DI).
The flexor muscles of the knee joint with lower support include the triceps surae muscle.
Triceps surae muscle
(m. triceps surae, Fig. 70-1).
When describing this muscle, there are different views on it. Some anatomists take its two superficial heads, called the gastrocnemius muscle
, as an independent muscle, while the third,
the soleus
, or internal gastrocnemius, is also isolated as a separate muscle. Others combine all three heads into one due to the fact that all these parts merge into one thick Achilles tendon (tendo Achillis) and therefore call it the triceps muscle of the leg. In this presentation we will adhere to the latter view.
The two superficial heads refer to the muscles that pass through two joints: the knee and ankle. The third head, the soleus, relates only to the ankle joint.
Rice. 70. Muscle of the posterior surface layer of the leg. (Spaltegolts.) Triceps surae muscle: 1 - gastrocnemius muscle, 2 - soleus muscle, 3 - common flexor digitorum longus tendon, 4 - peroneus longus, 5 - peroneus brevis, 6 - plantaris muscle, 7 - semimembranosus tendon, 8 - mucosa bursa between the inner head of the gastrocnemius muscle and the tendon of the semimembranosus muscle
The first two heads, which make up the gastrocnemius muscle itself (m. gastrocnemius, Fig. 70-7), are very similar in structure and origin. They both begin at the condyles of the femur and have the same fiber arrangement. The inner head is thicker and longer, starting higher on the femur and ending lower. The inner edge of the superior tendon of the internal head is in contact with the semimembranosus tendon (Fig. 70-7), and between them is the mucous bursa (Fig. 70-8). Between the tendon of the internal head and the surface of the internal condyle there is also a mucous bursa, often communicating with the knee joint or with the bursa described above, located between the tendons of the two muscles. Sometimes in the tendons of both the internal and external heads there are sesamoid bones, which increase the angle of approach of the muscle thrust to the femoral condyles. Both heads of the gastrocnemius muscle are directed down to the midline of the leg and, drawing closer to each other, immediately pass into one common wide tendon. The end of the muscle fibers of both heads is very clearly expressed by an arcuate line, below which their common tendon runs. It, going down, narrows and, thickening, merges with the tendon of the soleus head, forming the Achilles tendon, which is attached to the lower part of the posterior surface of the calcaneal tubercle. Between the tendon and the adjacent upper part of the calcaneal tubercle there is always a mucous bursa
The third head of the triceps flexor of the leg - the soleus muscle (m. soleus, s. gastrocnemius internus, Fig. 71-1) - is located deeper than the two heads described; it starts from both bones of the leg: from the lower lip of the oblique line of the tibia and from the upper half of its inner edge, also from the head, from the upper third of the outer edge and from the posterior surface of the fibula and, in addition, from the tendinous arch between both bones, under which they pass nerve and vascular trunks of the leg. From all places of attachment of the soleus muscle, a tendon plate begins, which stretches along the anterior surface of the muscle and gives continuations into its depth, noticeable along its entire length. Short muscle fibers, usually not exceeding 2-3 cm
lengths along the medial and lateral surfaces begin directly from the corresponding bones, and in front - from the surface of the entire anterior tendon plate. The fibers are directed obliquely posteriorly and downward and also pass into a wide tendon plate, which covers almost the entire posterior surface of the muscle and, tapering downwards, passes into the Achilles tendon.
Rice. 71. Muscles of the posterior surface layer of the leg. (Braus.) Triceps surae muscle: 1 - its soleus part, 2 - distal segment of the gastrocnemius muscle, 3 - plantaris muscle, 4 - popliteus muscle, 5 - fascia of the popliteus muscle, into which the fibers of the semimembranosus muscle continue, 6 - internal head of the gastrocnemius muscle , 7 - external head of the gastrocnemius muscle, 8 - tendon of the semitendinosus muscle, 9 - semimembranosus muscle, 10 - deep fascia of the leg, 11 - superficial fascia of the leg, 12 - tendon of the plantaris muscle
This structure determines the presence of a large number of short fibers, which is characteristic of static muscles. The arc of movement produced by the soleus muscle is very small, but it can resist stretching for a long time, while exhibiting significant strength. It plays a major role in holding the body in an upright position, preventing the lower leg from bending forward under the influence of the weight of the body, the line of the center of gravity of which lies mostly in front of the ankle joint.
With the upper support and joint tension of all three heads, the triceps surae muscle acts on the double-armed lever, formed in this case by the foot, and produces mainly plantar flexion (extension). Without considering for now the actions of this muscle on the foot, let us dwell on an analysis of its actions in relation to the knee joint. With lower support, the triceps surae muscle with its calf heads will produce flexion at the knee joint. The soleus muscle, stretching the Achilles tendon, at the same time forms an arch, which serves as a support for the action of the gastrocnemius muscle. The effect of the gastrocnemius muscle on flexion of the knee joint is small, but with increasing flexion due to an increase in the angle of application of force, its effect also increases; at maximum knee flexion it is greatest.
The gastrocnemius muscle in general, through its combination with the single-joint soleus muscle, is important, on the one hand, for economical work during long walking, and on the other hand, for fast and sharp contractions (ballistic) during running and jumping. In the squat, where both knee flexion and plantar flexion of the foot (extension) occur simultaneously, the gastrocnemius muscle is primarily involved in plantar flexion.
Innervation; tibial nerve (n. tibialis, LV and SI-II).
Plantaris muscle
(m. plantaris, Fig. 71-3), very poorly developed, often completely absent. It starts from the femur above the external condyle, above the beginning of the head of the external gastrocnemius muscle, partly from the bursa of the knee joint; located in front of the gastrocnemius, between it and the soleus. It has a very poorly developed muscle belly, which turns into a long thin tendon, running downward and inward (Fig. 71-12). Coming from under the Achilles tendon from the inside, the tendon of the plantaris muscle either merges with it, or is independently attached to the calcaneal tuber, fused with its fibers to the wall of the mucous bursa, located here between the Achilles tendon and the calcaneal tuber, or ends, fused with the deep plate fascia of the leg.
The plantaris muscle in humans is a vestigial muscle. It is especially strongly developed in one- and two-hoofed quadrupeds: in them it passes through the calcaneal tubercle and merges with both the plantar fascia and the tendons of the plantar flexor digitorum. In plantigrade walkers, as well as in monkeys, the plantaris muscle is less developed and is already related only to the plantar fascia; in a person, depending on his vertical position and the pressure of the weight of the body on the heel tubercle, the place of its transition into the plantar fascia disappears, and the plantar muscle remains only on the lower leg. Depending on the place of its attachment, the plantaris muscle pulls either the posterior wall of the knee joint bursa, or the wall of the mucous bursa of the Achilles tendon, or, finally, only the fascia of the leg.
Innervation: tibial nerve (n. tibialis, LV and SI-II).
Muscles that rotate the shin outward and inward
All the muscles of this section have already been described above.
With the knee flexed and in superior support, the muscles that rotate the tibia are the knee flexors: biceps femoris, popliteus, semitendinosus, semimembranosus, sartorius, internal rectus.
Only the biceps femoris muscle, which is attached to the head of the fibula and tibia, and partly to the fascia of the leg, belongs to the outward rotation.
The muscles that internally rotate the tibia include the popliteus, semimembranosus, semitendinosus, rectus internus, and sartorius.
The popliteus muscle (Fig. 67-7), as is already known, begins on the outer condyle and is attached along the inner edge of the tibia, above the oblique popliteal line. By crossing the longitudinal axis of the tibia in an oblique direction, with upper support it can rotate the tibia inwards along with flexion.
The semimembranosus muscle (Fig. 63-9; 65-3), forming three bundles with its distal tendon, merges with the bursa of the knee joint, with the posterior plate of the fascia of the leg and is attached to the internal tubercle of the tibia. The remaining muscles - the semitendinosus, the sartorius and the internal rectus - form a general tendon stretch, known as the anserine, and are attached to the anterior crest larger than the tibia, immediately under its tubercle. With the knee bent, the tendons of these muscles cross the longitudinal axis of the tibia at a right angle and, approaching from the inside, are able to rotate the tibia inwards.
As for the triceps surae muscle, according to some researchers, the inner head of the gastrocnemius muscle can take part in inward rotation.