Main types and types of sprains
A sprain can affect any joint. The main types of this disease are muscle and ligament sprains.
In turn, they can affect the following joints:
- Ankle.
- Knee.
- Elbow.
- Carpal.
- Brachial.
- Clavicular.
Sprains are also divided into:
- traumatic. This is when force is applied in a direction that exceeds the range of motion. That is, this can happen when jumping, hitting, or sudden movements.
- degenerative. They arise due to the fact that the ligaments are worn out due to the aging of the body. This usually happens in old age. After all, a person’s blood supply is disrupted and the ligaments become weaker.
Features of types of stretching
When stretching occurs, the connective fibers are partially or completely torn.
So, during a fall or an incorrect turn, a sprain occurs in the ankle joint or hand. If the patient twists his shin, the ligaments of the knee joint are stretched.
Typically, when engaging in contact sports activities, sprains of the elbow joint occur. In some cases, such damage may be the result of a fight. Injury to the shoulder joint can occur due to sudden jerks or swings of the arms.
There are 3 degrees of stretching:
- The first one is easier. When it occurs, the tendons are injured and slightly torn. In this case, there is no restriction of mobility, since the pain is insignificant. Swelling may occur, but most often it is not noticeable.
- The second degree is more noticeable, but moderate. That is, slight stretching or rupture of the fibers occurs. This may damage the capsule. There is severe pain that is difficult to endure. In this case, swelling noticeably appears in the place where the injury occurred. Bruising may occur.
- This degree is the most serious, because it completely ruptures the tendons. Swelling becomes too noticeable, as well as hyperemia in the place where the joint is affected. Bruising is also widespread. The joint develops pathological mobility.
Non-steroidal anti-inflammatory drugs in the treatment of sprains of ligaments, tendons and muscles
About the article
75642
0
Regular issues of "RMZh" No. 7 dated 04/09/2005 p. 411
Category: General articles
Author: Mavsisyants L.A.
For quotation:
Mavsisyants L.A. Non-steroidal anti-inflammatory drugs in the treatment of sprains of ligaments, tendons and muscles. RMJ. 2005;7:411.
Well-known American specialists John Pagliano and Doug Jackson conducted a large clinical study in order to determine the nature of various running injuries and the causes that cause them. Over the course of 10 years, they examined 3,273 injured runners of varying abilities, analyzed more than 40 characteristics of injured athletes (age, gender, body weight, conditions of injury, footwear, training methods, etc.) and identified common causes, characteristics and symptoms of injuries.
Injuries were categorized into “female” and “male.” Thus, in men the most common symptoms are: inflammation of the plantar aponeurosis, damage to the tendon-ligamentous apparatus, functional insufficiency of the knee joint; in women - inflammation of the periosteum, “runner’s knee” (chondromalacia). Runners over 40 are more prone to back and foot injuries. Here are some other trends identified: Low-volume runners (less than 20 miles (32 km) per week) were more likely to be injured, 46%; the majority of injured people (66%) used only long slow running, the remaining 34% included some form of speed work; almost every (90%) athlete regularly used stretching exercises before and after running; beginners (14%) were injured less often than those who had more than 6 years of running experience (38%); men were injured twice as often as women. Among all injuries, the authors identified the 10 most common and 5 reasons for their occurrence: 1) too much volume, intensity of training, rapid increase in load; 2) running on too hard, hilly or uneven surfaces; 3) weak, inflexible muscles; 4) Running in inappropriate shoes; 5) defects in the structure of the foot. Sprains of ligaments, tendons and muscles Damage to the tendon-ligamentous apparatus is one of the most relevant and common causes that limit the physical activity of people leading an active lifestyle. The main etiological factor is acute traumatic injury, called sprain, or excessive cyclic load for a long time - overexertion. Sprains of ligaments, tendons and muscles are acute and traumatic due to damage. There are three degrees of severity of a sprain: Grade I – mild pain due to the tearing of several fibers of the ligament. Grade II – moderate pain, swelling and disability. III degree – severe pain due to ligament rupture and subsequent instability of the joint. A muscle strain, in turn, is a traumatic injury to the muscle fibers themselves or the connection between muscle and tendon and is also classified into three degrees of severity: I - moderate. II – moderate degree of damage, associated with weakness of the affected muscle and its painful contraction. III - complete rupture of the connection between muscle and tendon, manifested by severe pain and the inability to contract the damaged muscle. Overstrain is a non-acute, repeated damage to soft tissue structures due to constantly occurring microtraumas, which leads to changes in local microcirculation and, as a consequence, to degenerative processes in soft tissues, where microscopy shows a disruption of the structure of local tissues with their lysis, leukocyte infiltration and extravasation of blood . Repetitive movements during long-term work lead to “overuse” damage in some occupations. Approximately 10–20% of musicians, typists, cashiers and assembly line workers complain of relapses of sprain syndrome; among athletes, this percentage ranges from 30 to 50. Damage due to overexertion (overtraining) is divided into four degrees: I degree - pain only after physical activity . II degree – pain during and after physical activity, which does not affect the result of work. III degree – pain during and after physical activity, affecting the result of work. IV degree – constant pain that interferes with daily physical activity. It should also be noted that damage to the tendon apparatus can occur in the form of “tendonitis,” “tendinosis,” and “tenosynovitis.” Tendinitis occurs due to tendon injury and associated vascular destruction and acute, subacute or chronic inflammation. Tendinosis is a non-inflammatory atrophy and degeneration of fibers within a tendon, often associated with chronic tendinitis, which can lead to partial or complete rupture of the tendon. Tenosynovitis is an inflammation of the paratendon, which is the outer sheath of some tendons and is lined with a synovial membrane. We will focus on stress injuries caused by frequently repeated monotonous movements, that is, overexertion, and will also try to take into account mild degrees of sprain of ligaments, tendons and muscles, since injury accompanied by rupture of these structures in most cases requires surgical treatment (damage to the anterior cruciate ligament and collateral ligaments of the knee joint, rupture of the Achilles tendon). Types of damage: The most common types of damage due to overexertion (overtraining): – iliotibial tract friction syndrome, “jumper’s knee”, plantar fasciitis; – tendons – Achilles tendinitis, suprapatellar tendinitis, tibialis posterior tendinitis. Iliotibial tract friction syndrome (ITIS) is pain along the lateral aspect of the knee due to irritation and inflammation of the distal iliotibial tract as it passes over the lateral femoral condyle. The pain intensifies with palpation of the distal part of the tract at the moment of extension of the leg at the knee joint. STI occurs when running too intensely or running over rough terrain. “Jumper's knee” is the so-called patellar tendinitis. Often found in high jumpers, basketball and volleyball players, and runners. It is characterized by pain in the lower pole of the patella, at the site of attachment of the patellar ligament. It develops due to constant damage to this area when the injury does not recover and heal. Patellar bursitis is accompanied by pain, swelling and a local increase in temperature in the patellar bursa, which is located superficial to the patella. Bursitis is caused by repeated trauma or stress, such as kneeling. Inflammation of the Achilles tendon manifests itself as pain in the heel, sometimes pain along the back of the leg. Dorsal and plantar flexion of the foot increases pain, the area of greatest pain is 2-3 cm proximal to the junction of the tendon with the calcaneus. The tendon may be swollen and thickened, most often caused by spondyloarthropathy affecting peripheral joints (Reiter's disease, ankylosing spondylitis), as well as trauma. Plantar fasciitis or heel spur anatomically arises from the insertion of the flexor digitorum brevis muscle, which is localized along the anteromedial edge of the tuberosity of the calcaneus, slightly deeper than the insertion of the plantar fascia. Overexertion of one of these structures is thought to result in reactive inflammatory bone production or spur formation secondary to traction on these structures. However, it remains unclear which mechanism is responsible for this. In any case, the spur is secondary to overexertion. Also worth mentioning is shin splints, an overtraining injury caused by chronic traction on the periosteum of the tibia. In this case, either the tibial muscles or m. soleus, which is characterized by gradually onset pain along the anteromedial or posteromedial surface of the leg. Pain occurs in athletes at the start of the race, subsides during the run and intensifies again after the end of the race. On palpation, tenderness is detected along the posteromedial edge of the tibia, usually at the border of the middle and lower third. The pain intensifies with dorsal flexion of the foot against resistance. Treatment Primary therapy: • Weight-bearing protection • Rest • Ice • Pressure bandage • Elevation • Bandage support Secondary therapy • Physical therapy • Rehabilitation • Injections • Exercise therapy • Examination and re-examination • Salicylates The mainstay of treatment is early pain relief and anti-inflammatory therapy for soft tissue injury , especially in cases of concomitant myositis. Long-term inflammation impairs the healing process of soft tissues, which leads to their detraining and functional failure. With an active inflammatory process, relative rest for the affected area is important. Ice is effective as an anti-inflammatory agent only in the first hours after injury, then heat is preferable. Immobilization with a splint or bandage can be used to enhance protection of the injured limb or part of it from stress. Corticosteroid injections for chronic processes do not provide a complete cure; moreover, they increase the rate of collagen degradation, reduce the synthesis of new collagen, and reduce the tensile strength of the tendon, which leads to its rupture if injections are performed incorrectly or very often. In this regard, their use is justified only in the acute period and no more than once every 2–3 weeks. It is also necessary to use non-steroidal anti-inflammatory drugs (NSAIDs) per os. Their long-term use is recommended for chronic conditions of overstrain; for acute injury, they are effective for 72 hours. An effective method for treating traumatic injuries of soft tissue is local therapy using ointments and gels containing NSAIDs. A well-proven NSAID drug is Nurofen Plus. This is a combination drug, the effect of which is due to the effects of its constituent components ibuprofen (200 mg) and codeine phosphate (12.8 mg). Both active principles of the drug are well known and have been used in clinical practice for a long time. Their combination provides both central and peripheral effects. Ibuprofen is an NSAID, a derivative of phenylpropionic acid. Ibuprofen is widely used throughout the world, and in the last decade has become the standard against which the effectiveness and tolerability of other analgesics are compared. It has analgesic, antipyretic and anti-inflammatory effects. The excellent safety profile made it possible to distinguish ibuprofen from a number of other drugs in this group and give it the status of an over-the-counter drug. The main mechanism of action of ibuprofen is to inhibit the synthesis of prostaglandins, which leads to an increase in the pain sensitivity threshold of afferent nerve fiber receptors in relation to the corresponding mediators (histamine, substance P, serotonin, bradykinin). In addition, according to experimental studies, ibuprofen inhibits the migration of leukocytes from the bloodstream into damaged tissues. Codeine phosphate is an opium alkaloid of the phenanthrene series, an opioid receptor agonist. It has an analgesic effect; when used together with ibuprofen, it enhances its analgesic effect. Codeine, unlike ibuprofen, has a central effect. It is able to weakly bind opioid receptors, and some of it is converted into morphine. In addition, codeine inhibits the release of substance P, a neuropeptide that lowers the pain threshold. Codeine is rapidly absorbed from the gastrointestinal tract, after which it is largely metabolized in the liver. Approximately 10% of the ingested dose is converted to morphine and excreted in the urine. Composition and release form: Film-coated tablets 1 tablet. Ibuprofen 200 mg Codeine (in the form of codeine phosphate hemihydrate) 10 mg Excipients: MCC; sodium starch glycolate; hypromellose; povidone; pregelatinized corn starch. For adults and children over 12 years of age, the drug is prescribed 1–2 tablets. every 4–6 hours. The maximum daily dose is 6 tablets. The tablets should be taken with water. Nurofen in tablets and capsules has already received recognition from Russian specialists and consumers due to its high efficiency and quality. Now Nurofen gel is in great demand. The active substance of the gel, like all Nurofen products, is ibuprofen. When applied, Nurofen gel is instantly absorbed and begins to act, eliminating inflammation and pain. Clinical trials have demonstrated the high efficiency and rapidity of the therapeutic effect of Nurofen gel. Thanks to its light, pleasant texture, it is very convenient to use, as it leaves no marks on clothes and has virtually no odor. Nurofen gel is used not only for joint pain, bruises, sprains and sports injuries, but also for back pain. Release form: 50 g tube. Conclusions Injuries to the musculoskeletal system are common. And in the scheme of their treatment, NSAIDs play an important role (both per os and locally). Among this group, the drug Nurofen occupies a special place. Today it is represented in more than 120 countries and is effectively used in the treatment of various types of pain and fever by millions of people. Nurofen appeared in Russia in 1997, and quickly became one of the leading brands in the market of painkillers and antipyretics. Nurofen Plus provides targeted dual action against severe pain thanks to the appearance in Russia of the only combination of two substances - ibuprofen and codeine. It has been clinically proven that Nurofen Plus has the effectiveness and targeted action of ibuprofen and the additional benefit of codeine, which has a pronounced general analgesic effect. Nurofen gel acts directly at the site of severe pain. The use of modern topical preparations, such as Nurofen Plus and Nurofen gel, is an effective method of relieving pain and accompanying inflammation in case of traumatic injury to the tendon-ligamentous apparatus, which contributes to the rapid restoration of physical activity and improves the quality of life of patients.
Content is licensed under a Creative Commons Attribution 4.0 International License.
Share the article on social networks
Recommend the article to your colleagues
Sprain
Causes of sprains
A ligament that is severely sprained or torn by a sudden jerk (such as a sprained ankle) or severely damaged by a fall or slip.
Symptoms of a Sprain
- joint pain;
- swelling and redness;
- restriction or inability to move due to severe pain;
- in severe cases, joint deformation.
Complications
- damage to tendons (the tough fibrous structure that connects muscles to bones) or muscles;
- cracks or broken bones;
- Repeated sprains weaken the joint.
Crick
General information
Very often this happens due to intense physical activity, disproportionate to your capabilities, as well as during excessively active or fast movements or stress on unstretched, unheated muscles. You may feel something pop or tear when muscle or ligament tissue is too tight. It may be painful for you to walk and move. Typically, treatment for a sprain takes 1 to 6 weeks.
Symptoms
Muscle strain - the muscle in such injuries is overstretched, some tissues may be torn. There may be bleeding and swelling in the damaged area. As the sprain wears off, small scars may appear, so the muscle may not be as flexible or strong after the injury. If the joint has been too stressed, the tissues of the ligaments and other supporting elements of the joint may tear. In this case, the joint swells and becomes very sensitive and painful.
Prostatitis is the most common urological disease in adult men under 50 years of age and the third most common urological diagnosis in men over 50 years of age [1]. According to statistics, every second man experiences symptoms characteristic of prostatitis at least once during his life [1-3]. The prevalence of chronic prostatitis in the world ranges from 2.2% to 9.7% [4]. In the United States, chronic prostatitis accounts for about 8% of all visits to a urologist and 1% of all visits to a general practitioner [5]. About 5%-12% of infertile men have a history of inflammation of the genitourinary organs, including the prostate gland (P) [1].
We analyzed scientific data available in professional sources regarding pain associated with non-cancer lesions of the pancreas and methods for its management. The majority of patients with an established diagnosis of prostatitis belong to categories IIIa and IIIb (according to the classification of the American National Institute of Health (NIH USA). As a rule, in such men it is not possible to identify pathogenic microorganisms in the secretion of the pancreas, and the predominant complaint is pain in the perineum, above womb, groin, lumbosacral region, without clear localization, lasting more than 3 months, which can be regarded as chronic pelvic pain syndrome (CPPS).
According to Chinese researchers, chronic pelvic pain syndrome in chronic prostatitis is about 90-95% [6]. The intensity and nature of pain depend on many factors: age, characteristics of the disease, individual pain sensitivity threshold [7]. Pain syndrome that lasts for a long time, disturbances in urination and sexual life contribute to the emergence of a “vicious circle” that seriously affects the patient’s quality of life.
In prostatitis, both acute and chronic, the pathogenesis of pain is twofold:
- nociceptive pain;
- neurogenic pain.
Nociceptive pain sensations appear, as a rule, with inflammation and local ischemia. During inflammation, cellular and humoral immunity is activated with the release of biologically active substances, arachidonic acid, cycloxygenase (COX), responsible for the production of prostaglandins and thromboxane, leukotrienes, which cause irritation of pain receptors, form and maintain pain sensations [7]. Stimulation of pain receptors leads to the release of neuropeptides by unmyelinated nerve fibers (neurogenic nature of pain). LJ Miller et al. discovered the existence of biomarkers that correlate with the level of pain in chronic prostatitis and chronic pelvic pain syndrome.
It was found that neurotrophin, a protein that is part of the group of nerve growth factors, plays a fundamental role as a mediator of pain and an amplifier of neurogenic inflammation. Men with a history of long-term chronic prostatitis are 5 times more likely to have neurological diseases (for example, migraine, spinal disc disease, etc.) and symptoms such as numbness or tingling in the extremities [8]. There are certain standards for the treatment of chronic prostatitis using first-line drugs (such as antibiotics, alpha blockers). However, many patients note the persistence of pain for a long time even after the end of treatment [6]. Therefore, due to the widespread prevalence of pancreatic diseases, the search for alternative treatment methods is a current trend in medicine.
Since it is pain that causes the most suffering to men with prostate diseases, leading the patient to depression, sexual dysfunction, decreased self-esteem and overall quality of life, painkillers are included in the standards of treatment for most categories of prostatitis: acute, chronic bacterial, and chronic pelvic syndrome pain. To relieve prostate pain, the most widely used pharmacological group of drugs is nonsteroidal anti-inflammatory drugs (NSAIDs), which have both analgesic and anti-inflammatory properties [7].
The most well-known NSAIDs used in urological practice are ketoprofen, ibuprofen, and diclofenac. The main pharmacological effect of drugs in this group is the non-selective inhibition of the enzymes COX-1 and COX-2, due to which a peripheral analgesic effect is achieved [5]. NSAIDs are prescribed long-term with preference for rectal forms, thereby reducing the likelihood of adverse events from the gastrointestinal tract when taken orally [5]. Results of the meta-analysis by T. Anothaisintawee et al. showed that the use of NSAIDs is 80% effective in the treatment of chronic prostatitis and relief of chronic pelvic pain syndrome compared with placebo (relative risk: 1.8; 95% CI 1.2–2.6) [10].
V. Magri et al. recorded that the use of alpha blockers in combination with NSAIDs in patients with chronic prostatitis and chronic pelvic pain syndrome led to a decrease in pain and an improvement in quality of life [11]. The authors state: “Despite the fact that each of these drugs has certain side effects, and long-term use of NSAIDs is limited by the side effect profile, a multimodal therapeutic regimen for the treatment of chronic prostatitis is more rational than the use of drugs separately” [11]. Chinese researchers noted a decrease in pain, improvement in the quality of urination and life when using ibuprofen for 6 weeks in patients with chronic prostatitis [12].
Noteworthy is the study by A. Del Rosso et al. [13], the purpose of which was to determine the possibility of combining NSAIDs with antibacterial therapy to normalize the level of prostate-specific antigen (PSA) in negative prostate biopsies. The authors examined men (n=31) with PSA values of 4-10 ng/ml. After a gland biopsy, patients received 1000 mg of ciprofloxacin daily for 15 days in combination with 100 mg of ketoprofen administered rectally. PSA determination was repeated two weeks after treatment. Nineteen patients (61%) experienced a persistent decrease in PSA levels after therapy. PSA values were within normal limits in 5 patients (16%). The researchers concluded that elevated PSA values can be regarded as due to chronic inflammatory processes in the pancreas.
The combination of therapy with ketoprofen and antimicrobial drugs allows not only to relieve inflammation and pain, but also, as a result, to normalize PSA and avoid unnecessary biopsies in patients with “gray zone” PSA [13]. Despite the fairly high effectiveness of NSAIDs in the treatment of chronic prostatitis, drugs of this pharmacological group are not without side effects (dyspeptic disorders, damage to the gastric mucosa, decreased platelet aggregation, etc.). Therefore, world medicine continues to search for not only effective, but also safe drugs to eliminate pain, including pancreatic diseases. Having analyzed various NSAIDs presented in Russia, we became interested in the drug under the trade name “OKI”.
It is the lysine salt of ketoprofen and is available in the form of granules for the preparation of an oral solution and in the form of rectal suppositories containing 160 mg of ketoprofen. The combination of ketoprofen with lysine salt significantly enhances the pharmacokinetic properties of the drug while maintaining its good tolerability. “OKI” - lysine salt of ketoprofen is characterized by anti-inflammatory, analgesic and antipyretic properties, rapid onset of action and good tolerability [14]. “OKI” reduces pain due to a powerful anti-inflammatory effect, which is its common property with other NSAIDs, and is associated with inhibition of cyclooxygenase and partially lipoxygenase (Fig. 1).
Fig. 1. Mechanism of action of “OKI” - Ketoprofen lysine salt 1. The mechanism of action of “OKI” - Ketoprofen lysine salt
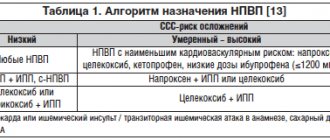
The combination of ketoprofen with the amino acid lysine led to an improvement in the pharmacokinetic properties of the molecule (Table 1) [14], due to which “OKI” has a dual mechanism of analgesic effect:
- peripheral (blocking the release of inflammatory mediators);
- central (decreased afferent signaling in receptors that report pain to the central nervous system and decreased central sensitivity).
Table 1. The mechanism of action of “OKI” – ketoprofen lysine salt [14] Table 1. The mechanism of action of “OKI” – ketoprofen lysine salt
The content of lysine salt in "OKI" improves the solubility of ketoprofen in the gastrointestinal tract (GIT), which facilitates the transport of the substance through the mucous membrane into the bloodstream, thereby ensuring high concentrations of the active substance in the site of inflammation and the speed of onset of the effect by almost 4 times, compared with regular ketoprofen. According to L. Brandolini et al. The content of the L-lysine molecule in ketoprofen has a gastroprotective effect due to its specific ability to regulate gastroprotective proteins and counteract NSAID-induced oxidative stress [14]. Due to rapid absorption from the gastrointestinal tract, OKI has a high safety profile compared to other NSAIDs derived from propionic and phenylacetic acid.
Therefore, “OKI” can be used both orally and rectally for longer periods. The results of the study by G. Carlucci et al. demonstrates high physicochemical compatibility between ketoprofen lysine salt and a number of medicinal substances: antispasmodics, vitamins, steroidal anti-inflammatory drugs, local anesthetics [15]. All this makes it possible to use “OKI” simultaneously with several pharmacological groups of drugs in the treatment of prostate diseases. Ketoprofen lysine salt is already widely used for pain relief in various branches of medicine [16,17]. G. Cossellu et al. compared the effect of ketoprofen lysine salt and paracetamol/acetaminophen on pain perception during dental procedures (n=151) [18].
The authors recorded the level of pain using a visual analogue scale (VAS). The results of this study showed that when using ketoprofen lysine salt, patients reported significantly less pain during the entire treatment period compared to the other drug (p < 0.05) [18]. Another study assessed the effectiveness of a single dose of paracetamol (12 mg/kg), ketoprofen lysine salt (40 mg sachet) compared with placebo in relieving acute pain in children aged 6-12 years (n=97) [19]. 1 hour after taking ketoprofen lysine salt, a subjective analgesic effect was noted by 55% of patients; after using paracetamol, 44% of people had a decrease in pain, and with placebo – 22% (p = 0.0156).
According to the observations of the parents of these children, good health after 1 hour was observed after taking ketoprofen lysine salt in 61% of people, after taking paracetamol - in 59% of people, and after taking placebo - in 25% (p = 0.0016). Thus, the observation of foreign authors demonstrates the successful, safe and effective use of ketoprofen in combination with lysine salt in reducing pain [19]. Ketoprofen lysine salt has been proven to be highly effective in the treatment of diseases of the musculoskeletal system compared to other NSAIDs (diclofennac and ibuprofen) [20]. The results of a multicenter, double-blind study (n=165) showed that after 7 days of using NSAIDs, there was a halving of pain in 78% of patients taking ketoprofen lysine salt (50 mg/day 3 times) versus 58% of patients using ibuprofen (p<0. 05) (Fig. 1) [20].
A particularly high analgesic effect is achieved with parenteral use of ketoprofen lysine salt. Complete pain relief was reported after 15 minutes with 100 mg ketoprofen lysine salt administered intramuscularly in 92% of patients compared with 84% of people who used diclofenac (75 mg intramuscular) (p < 0.001) [20]. Other authors also note an improvement in the quality of life, a persistent decrease in pain intensity and severity of vertebral syndrome with the use of Ketoprofen lysine salt. Based on their observations, researchers recommend long-term (at least two weeks) use of Ketoprofen lysine salt for the treatment of nonspecific lower back pain [21]. Observation by Russian scientists demonstrates the successful long-term use of ketoprofen lysine salt in the relief of pain [22].
The study included 3349 patients with diseases or injuries of the musculoskeletal system (mainly dorsopathy and osteoarthritis) [22]. According to A.E. Karataeva et al. the dosage form of ketoprofen lysine salt can be used for a long time due to its safety and high efficiency, especially in patients with chronic pain syndrome [22]. Similar results were obtained by Italian researchers comparing the use of ketoprofen with diclofenac and ibuprofen in the treatment of acute and chronic pain, both rheumatic and traumatic origin [23]. Thus, “OKI” - Ketoprofen lysine salt has additional advantages over ketoprofenic acid and other NSAIDs, having a more favorable pharmacokinetic profile and increased safety due to high absorption and good gastric tolerability.
"OKI" can be used in the treatment of all categories of prostatitis, since the drug affects the main links in the pathogenesis of this disease. The emergence of new modified drugs, such as OKI, significantly expands the possibilities for treating pancreatic diseases.
CONCLUSIONS
- "OKI" - Ketoprofen lysine salt is an innovative NSAID drug registered in 2010.
- "OKI" - Ketoprofen lysine salt is the most effective among NSAIDs derivatives of propionic acid.
- Thanks to the improved formula, “OKI” - Ketoprofen lysine salt is safe for the gastrointestinal tract, therefore, if it is necessary to prescribe long-term therapy with NSAIDs, “OKI” seems to be the most promising,
- Due to the pronounced analgesic and anti-inflammatory effect of "OKI", it is possible to use both a stand-alone drug and in combination with drugs from other pharmacological groups in multimodal therapy of chronic and acute prostatitis, as well as chronic pelvic pain syndrome.
LITERATURE
- Paulis G. Inflammatory mechanisms and oxidative stress in prostatitis: the possible role of antioxidant therapy. Res Rep Urol 2018;17(10):75-87. doi: 10.2147/RRU.S170400.
- Dendeberov E.S., Logvinov L.A., Vinogradov I.V., Kumachev K.V. Tactics for choosing a treatment regimen for bacterial prostatitis. Russian Medical Journal 2011;19(32):2071-2074. .
- Kulchenko N.G., Yatsenko E.V. Herbal medicine for inflammatory diseases of the prostate gland. Research and Practice in Medicine 2019;(3):87-97. doi:10.17709/2409-2231-2019-6-3-8.
- Vermassen T, Van Praet C, Poelaert F, Lumen N, Decaestecker K, Hoebeke P, et al. Diagnostic accuracy of urinary prostate protein glycosylation profiling in prostatitis diagnosis. Biochemia Medica 2015; 25(3): 439–449.
- Suskind AM, Berry SH, Ewing BA, Elliott MN, Suttorp MJ, Clemens JQ. The prevalence and overlap of interstitial cystitis/bladder pain syndrome and chronic prostatitis/chronic pelvic pain syndrome in men: results of the RAND Interstitial Cystitis Epidemiology Male Study. J Urol 2013;189(1):141-5. doi: 10.1016/j.juro.2012.08.088
- Hu M, Wazir J, Ullah R, Wang W, Cui X, Tang M, et al. Phytotherapy and physical therapy in the management of chronic prostatitis-chronic pelvic pain syndrome. Int Urol Nephrol 2019;51(7):1081-1088. doi:10.1007/s11255-019-02161-x.
- Tripp DA, Nickel JC, Shoskes D, Koljuskov A. A 2-year follow-up of quality of life, pain, and psychosocial factors in patients with chronic prostatitis/chronic pelvic pain syndrome and their spouses. World J Urol 2013;31(4):733–9. doi: 10.1007/s00345-013-1067-6
- Miller LJ, Fischer KA, Goralnick SJ, Litt M, Burleson JA, Albertsen P, et al. Nerve growth factor and chronic prostatitis/chronic pelvic pain syndrome. Urology 2002;59(4):603–608. doi: 10.1016/s0090-4295(01)01597-7
- Pontari MA, Krieger JN, Litwin MS, White PC, Anderson RU, McNaughton-Collins M, et al. Pregabalin for the treatment of men with chronic prostatitis/chronic pelvic pain syndrome: a randomized controlled trial. Arch Intern Med 2010;170:1586–1593. doi:10.1001/archinternmed.2010.328.
- Anothaisintawee T, Attia J, Nickel JC, Thammakraisorn S, Numthavaj P, McEvoy M, et al. A. Management of chronic prostatitis/chronic pelvic pain syndrome: a systematic review and network meta-analysis. JAMA 2011;305(1):78-86. doi: 10.1001/jama.2010.1913.
- Magri V, Boltri M, Cai T, Colombo R, Cuzzocrea S, De Visschere P, et al. Multidisciplinary approach to prostatitis. Arch Ital Urol Androl 2019;90(4):227-248. doi: 10.4081/aiua.2018.4.227.
- Lee CB, Ha US, Lee SJ, Kim SW, Cho YH. Preliminary experience with a terpene mixture versus ibuprofen for treatment of category III chronic prostatitis/chronic pelvic pain syndrome. World J Urol 2006; 24(1):55–60. doi: 10.1007/s00345-005-0039-x
- Del Rosso A, Saldutto P, Di Pierro ED, Masciovecchio S, Galatioto GP, Vicentini C. Impacts of antibiotic and anti-inflammatory therapy on serum prostate specific antigen in asymptomatic men: our experience. Urologia 2012;79(Suppl 19):37-40. doi: 10.5301/RU.2012.9364.
- Brandolini L, d'Angelo M, Antonosante A, Villa S, Cristiano L, Castelli V, et al. Differential protein modulation by ketoprofen and ibuprofen underlines different cellular response by gastric epithelium. J Cell Physiol 2018;233(3):2304-2312. doi: 10.1002/jcp.26102.
- Carlucci G, Gentile MM, Bartolini S, Anacardio R. Physicochemical compatibility between ketoprofen lysine salt injections (OKi Fiale, PG060) and pharmaceutical products frequently used for combined therapy. Boll Chim Farm 2004;143(1):15-9.
- Trubetskaya E.A., Boyko A.N., Khozova A.A., Kamchatnov P.R. , Petrov S.V., Otcheskaya O.V., GandzhulA P.A. The effectiveness of the lysine salt of ketoprofen (arthrosylene) in the treatment of nonspecific vertebrogenic pain syndromes in an outpatient setting. Journal of Neurology and Psychiatry. CC Korsakova 2013;113(1):53-5. .
- Alekseev VV, Alekseev AB, Goldzon GD Nonspecific pain in the lower back: from symptomatic to pathogenetic treatment. Journal of Neurology and Psychiatry. CC Korsakova 2014;114(2):51-5..
- Karateev A.E., Zhuravleva M.V., Alekseev V.V., Denisov L.N., Tsapina T.N. The effectiveness of a combination of dosage forms of ketoprofen lysine salt (ARTROZILEN®) in patients with musculoskeletal pain in clinical practice. KULON study (ketoprofen: satisfaction with treatment and assessment of adverse events). Clinical pharmacology and therapy. 2013;22(4): 23-30. [Karateev AE, Zhuravleva MV, Alekseev VV, Denisov LN, Tsapina TN The effectiveness of the combination of dosage forms of ketoprofen lysine salt (ARTROZYLEN®) in patients with musculoskeletal pain in clinical practice. CULON study (ketoprofen: satisfaction with treatment and evaluation of adverse events). Klinicheskaya farmakologiya i terapiya=Clinical pharmacology and therapy 2013;22(4): 23-30 (In Russian)]
- Sarzi-Puttini P, Atzeni F, Lanata L, Bagnasco M, Colombo M, Fischer F, et al. Pain and ketoprofen: what is its role in clinical practice? Reumatismo 2010; 62(3):172-188.
| Attached file | Size |
| 314.7 kb |
‹ Reproductive potential of spermatozoa obtained surgically in patients with azoospermia Up Modern methods of preventing infectious and inflammatory complications of contact and extracorporeal lithotripsy ›
What can you do
If you notice these signs, immediately visit a doctor who can treat you:
- There is severe unbearable pain, which makes it difficult to move and move the joint.
- There is a feeling of numbness in the place where the joint or limb was damaged.
- You notice extensive redness and a hematoma has appeared.
- You have lost the ability to move the joint, or the movements have become unnatural and painful.
- You hear a cracking sound in your joints and at the same time feel a sharp and piercing pain.
- There is a feeling of fever: chills, body temperature rises.
- A couple of days after the injury there are no noticeable changes.
What can a doctor do?
When sprained
The doctor will order an x-ray of the joint to identify bone displacement or fracture, and will properly fix the joint to ensure the joint remains immobile while the damage heals. Surgery is performed to repair severely torn ligaments or tendons.
For muscle strain
Your doctor may suggest that you use medications to relieve pain and reduce swelling, but most sprains will go away on their own within a week or so if you follow the above recommendations. You may need a referral to a physical therapist. If the joint sprain is very severe, your doctor may suggest x-rays to make sure there is no damage to the bone. If the ligament is completely torn, surgery may be necessary.
What should be inside drugs for the treatment of joints and ligaments
It is necessary that every athlete be able to distinguish dummy supplements from valuable substances that really have a positive effect on damaged joints and ligaments, strengthen them and promote their speedy recovery, and also serve as good prevention.
The most effective ingredients are glucosamine sulfate, chondroitin sulfate, collagen, as well as vitamin D and calcium (provided they are taken together).
In addition, high-quality preparations for the treatment of joints and ligaments may contain:
- methylsulfonylmethane - relieves discomfort, suppresses the inflammatory process;
- bromelain - effective for recent injuries, relieves pain well;
- hyaluronic acid - helps maintain flexibility and mobility of joints;
- vitamins B6, E and C - inhibit oxidative processes, work as antioxidants;
- zinc, selenium, magnesium - ensure normal cell functioning;
- Omega-3 fatty acids - relieve discomfort and reduce pain.
And although extracts of plant and animal origin are considered ineffective, such products may contain, for example, shark cartilage and curcumin. But they rather act as auxiliary substances, and by themselves are not capable of improving health.
In short, any working drug is aimed not only at the regeneration of connective tissues, ligaments, cartilage, tendons, joints, but also at increasing the functionality of the entire musculoskeletal system, as well as antioxidant protection.
Prevention of sprains
A sprain can occur in almost anyone who does not follow precautions during physical education and active recreation. Therefore, if you decide to train, you will need suitable shoes and clothing for this. If you like high heels, be careful and pay close attention to the road to avoid potholes and potholes. It is also important to monitor your weight. After all, excess weight can cause joint overload, which leads to sprains. And if you love sports, then you need to eat well. At the same time, constant uniform load can strengthen the ligaments.