The shoulder girdle (SG) is one of the most loaded joint complexes of the human body. It is he who is responsible for the basic musculoskeletal properties of human hands. This part of the skeleton is structurally connected to the upper and cervical spine. The PP is susceptible to a number of inflammatory and non-inflammatory diseases, and developmental anomalies are also possible. The ability to maintain joint mobility depends on the correct treatment.
Blade structure
The large, flat, triangle-shaped bone located on the upper back is called the scapula. This is a paired bone, the base of which goes up and the sharp end goes down on both sides of the spine. It appears to be a wide, flat structure that is slightly curved backwards.
Reference. A pair of shoulder blades at the back and a pair of clavicles at the front are needed to form the bony shoulder girdle.
Skeleton of the dorsum of the scapula:
- The spine is a bony ridge that crosses the upper edge of the scapula.
- The acromion is the humeral process with which the spine ends. The junction of the acromion and the clavicle constitutes the acromioclavicular junction.
- The coracoid is a hook-shaped projection shaped like a bird's beak that is located on the top of the bony structure near the glenoid socket. Muscles and ligaments are attached to it.
- The neck is a narrowed place that is adjacent to the glenoid cavity of the bone. This area serves to connect the articular surfaces of the scapula and shoulder; it forms the glenohumeral joint.
- Body of the scapula.
- Side edge.
- External corner.
The anterior surface of the human scapula consists of the following elements:
- Body.
- The articular socket together with the head of the humerus forms the shoulder joint.
- Coracoid process.
The anterior surface of the bone structure is concave, and the posterior surface is convex. The scapular muscle is attached to the anterior part.
The upper edge of the bone contains a depression in which nerve fibers and blood vessels pass. The vertebral margin is located next to the spinal column. And the lateral edge is the largest area that is formed by tubercles on the brachialis muscle.
There are 3 angles of the scapula:
- The upper one has a round shape and is located on top.
- The lower one has a thicker structure.
- The lateral one is very thick, includes the articular cavity, which connects to the head of the humerus. It is located opposite the superior medial angle.
The lateral angle is separated from the body of the scapula by the neck.
Anatomy of the scapula
The structure of the scapula is shown above.
Shoulder joint
Shoulder joint, articulatio humeri,
connects the humerus, and through it the entire free upper limb, with the girdle of the upper limb, in particular with the scapula. The head of the humerus, which participates in the formation of the joint, has the shape of a ball. The articular cavity of the scapula that articulates with it is a flat fossa.
Along the circumference of the cavity there is a cartilaginous articular lip, labrum glenoidale
, which increases the volume of the cavity without reducing mobility, and also softens shocks and shocks when the head moves. The articular capsule of the shoulder joint is attached on the scapula to the bony edge of the glenoid cavity and, covering the humeral head, ends at the anatomical neck.
As an auxiliary ligament of the shoulder joint, there is a slightly denser bundle of fibers coming from the base of the coracoid process and woven into the joint capsule, lig. coracohumerale
. In general, the shoulder joint does not have real ligaments and is strengthened by the muscles of the upper limb girdle.
This circumstance, on the one hand, is positive, since it contributes to extensive movements of the shoulder joint, necessary for the function of the hand as an organ of labor. On the other hand, weak fixation in the shoulder joint is a negative point, causing frequent dislocations.
The synovial membrane lining the inside of the joint capsule gives rise to two extra-articular protrusions. The first of them, vagina synovialis intertubercularis
, surrounds the tendon of the long head of the biceps muscle, lying in
the sulcus intertubercularis
; another protrusion, bursa m. subscapuldris subtendinea, located under the upper section of m. subscapularis.
Representing a typical multi-axial ball and socket joint, the shoulder joint is characterized by great mobility. Movements occur around three main axes: frontal, sagittal and vertical. There are also circular movements (circumduction). When moving around the frontal axis, the arm produces flexion and extension. Abduction and adduction occur around the sagittal axis.
The limb rotates outward (supination) and inward (pronation) around the vertical axis. Flexion of the arm and abduction are possible, as stated above, only to the level of the shoulders, since further movement is inhibited by the tension of the articular capsule and the support of the upper end of the humerus into the arch formed by the acromion of the scapula and lig. coracoacromiale
.
If the movement of the arm continues above the horizontal, then this movement is no longer performed in the shoulder joint, but the entire limb moves together with the belt of the upper limb, and the scapula rotates with a shift of the lower angle anteriorly and to the lateral side.
The human hand has the greatest freedom of movement. Freeing the hand was a decisive step in the process of human evolution. Therefore, the shoulder joint has become the loosest joint in the human body. As a result, we can reach any point of our body with our hands and manipulate our hands in all directions, which is important during labor processes.
On the posterior radiograph of the shoulder joint, the cavitas glenoidalis is visible, having the shape of a biconvex lens with two contours: medial, corresponding to the anterior semicircle of the cavitas glenoidalis, and lateral, corresponding to its posterior semicircle. Due to the characteristics of the x-ray picture, the medial contour turns out to be thicker and sharper, as a result of which the impression of a half-ring is created, which is a sign of normality (“clear half-ring symptom”).
In old age and with certain diseases, the lateral contour also becomes emphasized, and then the normal “semi-ring symptom” of cavitas glenoidalis
is replaced by a pathological “ring symptom”.
The head of the humerus on the posterior radiograph in its inferomedial part is superimposed on the cavitas glenoidalis. Its contour is normally smooth, clear, but thin. Between the cavitas glenoidalis scapulae and the caput humeri, the x-ray gap of the shoulder joint is visible. The “X-ray joint space” of the shoulder joint looks like a curved clearing located between the clear contours of the medial (anterior) edge of the cavitas glenoidalis and caput humeri
.
To determine the dislocation or subluxation of the shoulder joint, it is very important to know the normal relationships between the articular surfaces of the articulatio humeri
.
On a radiograph taken in the correct posterior projection with the limb extended along the body, these relationships are characterized by the fact that the inferomedial part of the head is layered on the cavitas glenoidalis
and is always projected above its lower border.
The shoulder joint receives nutrition from the rete articulare, formed by the branches of a. circumflexa humeri anterior, a. circumflexa humeri posterior, a. thoracoacromialis (from a. axillaris
).
Venous outflow occurs in the veins of the same name, flowing into v. axillaris
.
The outflow of lymph is through the deep lymphatic vessels - into the nodi lymphatici axillares
.
The joint capsule is innervated from n.
axillaris .
Anatomy of the clavicle
The S-shaped bone, curved along its long axis, is called the clavicle. It is located horizontally on the front and upper part of the chest. This bone borders the neck. The clavicle is classified as a tubular bone, and it consists mainly of spongy substance.
The clavicle consists of a body, an outer end and an inner end
Topography of the human clavicle:
- Body of the bone.
- Outer end.
- Inner end.
The inner end is adjacent to the manubrium of the sternum, it has a convexity that curves forward, and the other part curves backward. The middle part of the bone structure is slightly compressed from top to bottom. The nutrient foramen is located in the lower part of the clavicle. At the inner end there is a recess for the costoclavicular ligament.
The left outer end of the bone is connected to the acromion of the scapula. On this part of the bone there is a cone-shaped tubercle, as well as a trapezoid-shaped line. On the lower surface of the clavicle body, closer to the acromion, there is a recess for the attachment of the muscle of the same name.
The bone is smooth on top and rough on the bottom, with tubercles and lines. Its inner end is thicker. On its inner side there is an articular surface. The outer end is wider, but not as thick. This one often connects the clavicle to the acromion of the scapula.
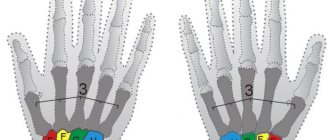
Anatomy of the human hand: basic components
Anatomically, the hand is the upper limb of the human musculoskeletal system. Like most parts of the body, it is formed by bone and muscle structures, ligaments, cartilage and tendons, as well as a network of blood capillaries and nerve fibers that provide tissue nutrition and impulse transmission, respectively.
For a more detailed study, the anatomy of the hand is usually classified into several key areas:
Each of these zones is sequentially connected to the others through complex joints. It is thanks to this that the arms can remain mobile, maintaining a wide trajectory of movement.
Structure and functions of the shoulder girdle
The shoulder girdle is the transition point from the torso to the upper limbs. It consists of two shoulder blades - right and left - and the same number of clavicles. Thanks to them, the position of the arms relative to the body is supported, as well as their movement along three different axes.
The shoulder blade is a flat, triangular bone located on the side of the back. Its relatively small thickness increases towards the lateral edge, where the articulation with the head of the humerus is located. The glenoid cavity, surrounded by tubercles, supports the humerus and allows for circular movements of the arms.
The scapula itself is slightly curved outward in the direction from the costal arches. On its outer side there is a key bone axis, on both sides of which powerful supraspinatus and infraspinatus muscle fibers are attached. The remaining muscle groups, as well as the ligaments that support the shoulder, are attached to the forward-facing coracoid process.
Another bone of the shoulder girdle - the collarbone - is tubular and has a slightly curved S-shape. It is located horizontally and slightly inclined downwards in the neck area. The collarbones serve as a connecting link between the sternum and shoulder blades, and also support the muscular frame of the shoulder girdle.
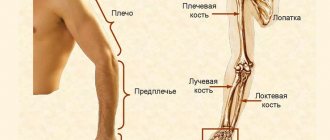
Anatomy of the bones and muscles of the arm in the shoulder area
The shoulder is the upper part of the arm connected directly to the torso. At the elbow joint it passes into another area - the forearm. The shoulder consists of a large tubular bone, the shape of which varies depending on the zone: if closer to the shoulder blade, the section of the humerus has an almost perfectly rounded shape, then closer to the forearm it resembles more of a triangle with rounded corners.
The shoulder bears the majority of the physical load during work, so its muscular system is represented by strong, durable and powerful muscles that are easily amenable to physical development and improvement. The main part of the fibers surrounds the humerus, located parallel to the vertical axis. The skin in this area is relatively thin, so in physically developed, muscular people, the attachment points and the main bends of the muscles stand out noticeably. It is believed that the volume and relief of the forearm is directly proportional to a person’s strength, but this is not entirely correct: the basis of physical strength is not the size of the muscles, but their training, the ability to quickly contract and relax when exposed to high loads.
The functions of the shoulder are varied and include almost the full range of movements of the arm. To understand how this system functions, let's look at the anatomy of the key muscles that carry out certain actions.
Biceps
The biceps is the biceps brachii muscle, both heads of which tightly cover the upper part of the humerus. The two heads of the biceps - short and long - begin in the region of the shoulder joint, and approximately in the middle of the humerus they intertwine together, descending to a round eminence on the forearm.
By contracting and relaxing the muscle fibers that make up the biceps, a person can do the following:
- move your palms up, rotate and straighten them;
- flex your shoulder;
- raise your arms forward and up, including with a load.
Triceps
The triceps, or triceps brachii muscle, consists of three heads of varying lengths that cover the elbow and part of the shoulder joints on the back of the arm. The medial and lateral fusiform heads of the triceps originate in the area of the humerus, and the long one is attached to the protrusion of the scapula. They, like the heads of the biceps, merge into one system in the lower part of the shoulder, forming a tendon attached to the olecranon process of the forearm bone.
The functions of the triceps are as follows:
- straightening the arm parallel to the vertical axis of the body;
- bringing the hand to a position near the body.
Brachialis muscle
This muscle is located directly under the biceps and comes to the surface of the muscular skeleton only at the point of attachment in the lower segment of the humerus. It is not as powerful as the biceps, but it also plays a key role in the physiological capabilities of the arm - thanks to its rhythmic contractions, a person can lift the ulna and flex the forearm.
Brachioradialis muscle
As the name suggests, this group of muscle fibers connects the shoulder and elbow joints, running along the entire length of the humerus. Its main function is to bend the arm at the elbow during contraction. You can notice this muscle on the surface of the ulnar fossa - its ridge protrudes especially clearly when lifting weights.
Anatomy of the forearm
The area of the upper limb starting at the elbow and ending at the wrist is called the forearm. It is formed by two bones of different diameters - the radius and the ulna. The section of the ulna has a triangular shape with a thickening at the upper end, at the point of articulation with the humerus. In front of the elbow joint there is a small trochlear notch that limits elbow extension, preventing unphysiological hyperextension of the muscles of the forearm and shoulder.
The radius, on the contrary, thickens downward, at the carpal joint. They are connected to the ulna bone movably, thanks to which the hand can rotate up to 180 degrees.
In its normal state, the forearm has a flattened shape with a noticeable expansion upward. This configuration is due to the specific location of the muscle tissue: closer to the elbow joint there are massive muscle bellies, which narrow and turn into tendons in the wrist area. Thanks to this, the volume of the lower part of the forearm can be used to judge how developed the bone structure of the hand is - thin carpal zones are characteristic of people with anatomically weak bones, and vice versa.
The muscles of the forearm are divided into 3 key groups. At the front are the fibers that control flexion and extension of the wrist and fingers, at the back are the extensor muscles, and at the side are the group responsible for the movement of the opposable thumb.
Topography of the humerus
The tubular bone that is located in the upper part of the arm is called the humerus. It has a long body and widens at the ends. The upper section is round in shape, and the lower section is triangular.
The humerus bone consists of a body, upper, lower end
Topographic anatomy of the humerus:
Clavicle subluxation
- The upper end (proximal epiphysis) consists of a rounded head that fits into the glenoid cavity of the scapula and forms the shoulder joint with it. Under the articular surface there is an anatomical neck. Under the neck there is a large and small tubercle, to which the muscles are attached. From both tubercles, ridges descend down the body of the bone. Between the tubercles and ridges there is a recess for the biceps tendon. The surgical neck is located under the tubercles.
- The body of the bone starts from the surgical neck. Approximately in its middle (outer surface) there is a deltoid tuberosity, to which the muscle of the same name is adjacent. On the back surface there is a radial groove, which spirals downwards and then outwards. The radial nerve passes through this depression, as well as the large brachial artery, which provides blood supply to the posterior group of muscles, the humerus.
- At the lower end (distal epiphysis) there are the internal and external condyles, as well as the articular surface that connects the humerus to the bones of the forearm. The trochlea of the humerus is the inner part of the articular surface that is adjacent to the ulna. The head of the condyle is the outer part that connects to the radius. Above the trochlea, in front and behind, during movement of the upper limb, the coronoid (in front) and also the olecranon (in back) processes enter. The epicondyles (internal and external) are located under the distal end of the humerus. The ulnar nerve groove is located on the posterior side of the internal epicondyle.
Muscles and also ligaments are attached to the epicondyles.
Which lifts are most effective?
There are no ineffective exercises, there is incorrect technique and lack of understanding of the process, which leads to a lack of results and, as a consequence, the question “which exercises are effective” arises
Before we look at the basic exercises, remember this trick: Do imaginary rows and presses without weight for three to five minutes every day. This way you will learn to perform the exercise correctly and feel the muscle group working.
Try to understand the difference between pulling with your arms and pulling with your elbows. Don’t try to skip this exercise; if you master visual traction, you will be able to perform the exercises competently, and the classes will not be wasted for you. Now let's look at the exercises.
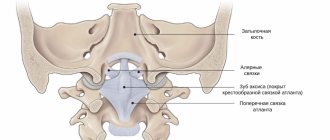
Ligamentous apparatus
The connection between the acromion and the collarbone is called the acromioclavicular joint. It is formed by flat articulated surfaces. The joint is stabilized by the coracoclavicular ligament, which arises from the coracoid process and reaches the inferior surface of the clavicle.
Shoulder joint ligaments
The scapula has its own ligaments – the coracoacromial and superior transverse. The first looks like a triangle-shaped plate that runs from the acromion to the coracoid process of the scapula. The coracoacromial ligament forms the arch of the shoulder.
The structure of the humeral joint is simple: a spherical head and an articular recess of the scapula.
Reference. The articulating depression of the scapula is equal to 1/3 of the surface of the head. The labrum is a ring-shaped cartilaginous formation that is attached along the edge of the glenoid fossa, increasing its depth.
The articular capsule is adjacent to the anatomical neck of the shoulder. It is quite thin and large. Between the tubercles of the bony structure of the shoulder is the synovial sheath (inner layer of the capsule), which surrounds the tendon and facilitates its gliding.
Auxiliary elements of the shoulder joint capsule: coracobrachial ligament, supraspinatus, infraspinatus, subscapularis and teres minor muscles. The ligament stabilizes the joint capsule, and the muscles not only strengthen it, but also protect it from pinching.
Reference. The humeroulnar joint is formed by the humerus and ulna. The humeral joint is formed by the humerus and radius bones.
Shoulder muscle injuries
A sprain or rupture of the ligaments of the shoulder joint is one of the most common sports and everyday injuries.
Causes:
- sudden movement, blow, fall on an outstretched arm;
- hanging on one arm, sudden lifting of weights;
- fractures - when fragments are displaced, damage to muscle and tendon fibers occurs;
- incorrect execution of bench presses in a prone position or from the forearm, exercises on the horizontal bar and uneven bars.
Weakening of the muscular and ligamentous apparatus often occurs due to metabolic disorders, age-related changes, smoking, intoxication, and long-term hormonal therapy. If a sprain is left untreated, tendonitis, bursitis , and tendon problems arise.
Muscles
The upper limb girdle includes the following muscles:
- Deltoid. The fibers of this muscle extend from the spine, acromion, acromial end of the clavicle, and adjoin the deltoid tuberosity of the humerus. The posterior part (scapular) extends the shoulder, and the anterior (clavicular) flexes.
- Supraspinatus. This anatomical structure originates from the supraspinatus fossa of the scapula and is attached to the superior portion of the greater tubercle of the humerus. The supraspinatus muscle abducts the shoulder.
- Infraspinatus. It is localized in the infraspinatus recess of the scapula, and is attached to the greater tubercle of the shoulder. The infraspinatus muscle helps adduct, rotate and extend the shoulder.
- Small round. It arises from the scapula and is adjacent to the greater tubercle. It allows you to rotate your shoulder outward.
- Big round. It starts from the lower angle of the scapula and is attached to the crest of the lesser tubercle. Functions: adduction, internal rotation, shoulder extension.
- Subscapular. It starts from the outer edge of the scapula, fills the subscapular cavity, and is attached to the lesser tubercle of the shoulder. It helps move the arm inward and bring it toward the body.
Muscles of the upper limb girdle
Classification of shoulder muscles:
- The anterior group (flexors) includes the coracobrachialis, brachialis, and biceps muscles.
- Posterior group (extensors): triceps and ulnaris muscles.
The structure of the muscles of the humerus:
- Coracobrachial. It arises from the coracoid process and attaches under the crest of the lesser tubercle to the humerus. Responsible for bending the arm.
- Shoulder. It arises from the lower two-thirds of the humerus, adjacent to the tuberosity of the elbow. Participates in flexion of the forearm.
- Double-headed. The long head of the muscle comes from the supraglenoid tubercle of the scapula, and the short one comes from the coracoid process, connects with the tuberosity of the radius and the fascia of the forearm (the connective tissue membrane that covers organs, vessels and nerves). The biceps muscle flexes the shoulder, forearm, and allows you to rotate your arm from the elbow to the wrist.
- Three-headed. The long head extends from the tubercle of the scapula under the joint, and the inner and outer heads arise from the posterior surface of the humerus. They are adjacent to the tendon, which is attached to the olecranon process. Helps to make extension, adduction movements of the shoulder, forearm and straighten the elbow.
- Elbow. It starts from the external epicondyle of the shoulder, the ligament of Henle, as well as the fascia, and connects to the ulna in its upper part on the posterior surface. Helps extend the forearm.
All muscles in the area of the shoulder joint are located on top. Below the bony junction is the axillary depression, through which the nerves and blood vessels of the arm pass.
How to pump up and strengthen the muscles of the shoulder girdle
To pump up and give beautiful relief to your shoulders and forearms, you need to perform strength exercises .
The weight for exercise must be selected taking into account physical fitness, otherwise you can get serious injuries. You need to start with 5-7 repetitions, perform 3 approaches. The best exercises for developing the muscles of the shoulder girdle :
- The close-grip bench chest press is one of the effective exercises for developing the strength of the triceps and pectoral muscles.
- Bench extension with a barbell lying down. For deep muscle work, it is better to use barbells with a straight bar.
- Pull-up on the horizontal bar with a neutral grip.
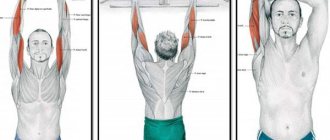
- Lifting dumbbells from behind your head. To achieve results, the hand must be retracted as much as possible and fixed in the lower position.
It is better to perform in a standing position, this accelerates the growth of the shoulder, pectoral muscles, deltoid muscles, and the long head of the triceps. Your arms should be straightened strictly above your head, without falling back.
Dumbbell press.- Swing dumbbells in a lying position. Lie face down on the bench, toes touching the floor. Take dumbbells in your hands, bend your arms slightly at the elbows. Raise the weight, bringing your shoulder blades together.
- Bent-over dumbbell raises. Tilt your body, bend your knees. Do 7 repetitions with a neutral grip - palms facing each other. Another 7 - with a reverse grip - palms facing down.
Valeria
General doctor
Ask a Question
To pump up your shoulders, you need to create a proper training program. The complex should include exercises for various muscle groups in the shoulder area. If you need to work specific muscles, you just need to increase the number of approaches. Before training, be sure to warm up to avoid injury. Classes should be done every other day, the muscles should rest.
Functions of the bones of the shoulder girdle
The role of the scapula in the girdle of the upper limbs is important; first of all, it ensures the mobility of the arm, connecting the humerus and collarbone.
The bones of the shoulder girdle, together with ligaments and muscles, allow various movements of the arms
Other functions of the scapula:
- protective;
- connecting;
- stabilizing;
- motor.
This bone structure protects important organs and blood vessels from damage.
Together with the muscles, the scapula provides mobility of the upper limb:
- rotation;
- abduction to the side, back, forward;
- lifting up.
Reference. To determine the functional state of the shoulder girdle in the joint area, the volume of active (movements that a person performs) and passive (movements that a doctor performs) movements are measured. Measurements are recorded in degrees. For example, physiological movements in the shoulder joint: flexion - about 90°, extension - up to 45°, abduction - no more than 90°, abduction with the participation of the scapula can reach 180°.
Functions of the clavicle:
- Support. The scapula and arm are attached to the clavicle bone. In addition, this bone connects the upper limb to the rest of the skeleton.
- Transmits physical impulse from the upper limb to the axial skeleton.
- Provides protection to nerves, blood and lymphatic vessels, which are located in the area between the neck and arm.
The humerus is a kind of lever, thanks to which the amplitude of arm movements increases. In addition, it helps maintain balance when the center of gravity shifts during movement.
How to deal with weak areas in the muscles?
— If your body does not have strong enough trapezius and deltoid muscles, then add more repetitions of shoulder exercises to your training program. Every week, increase the load by about 5-10% of the original.
— Instructors also advise trying the “drop method,” in which the exercises begin with the maximum weight you can tolerate without harm to your health, during which you progressively reduce the weight and the degree of load on the body.
— Also, for accelerated training of the muscles of the shoulder girdle, super series of presses and lifts are used. How does this happen in practice? Each barbell press is followed by dumbbell raises (for experienced athletes, high barbell rows) to invigorate the entire anterior deltoid muscle and add intensity to the workout. But be sure to discuss this method with your instructor, as pain may occur after training.
Injuries and illnesses
The likelihood of damage to the scapula increases when falling on the back, shoulder, arm, or after a direct blow. With closed injuries, there are no wounds; with open injuries, the integrity of the skin is compromised.
Injuries to the bones of the shoulder girdle are common.
Reference. Most often, the scapula is injured in the area of the articular socket and acromion. The most serious injury is considered to be a neck fracture, which can lead to dangerous complications.
Scapula injuries:
- The fracture is accompanied by a triangular swelling and pain, which intensifies when the victim tries to move his arm. When a fracture is displaced, a characteristic crunch is heard. In case of an injury in the area of the bone connection, the shoulder and arm are raised; in case of a fracture in the neck area, the arm hangs down. If the acromion process is damaged, the shoulder protrudes forward, and if the coracoid process is damaged, it deepens.
- Dislocation of the scapula is a rare occurrence. The injury occurs after a sudden movement of the upper limb to the side. It manifests itself as protrusion of the scapula and intense pain.
- Bursitis (inflammation of the joint capsule) can be caused by infection, trauma, or autoimmune diseases. The pathology is accompanied by pain in the affected area, swelling, redness of the skin, numbness, and limited movement in the joint.
- Pterygoid scapulae, as a rule, are of congenital origin. Acquired pathology occurs due to prolonged curvature of the spine (scoliosis, kyphosis, etc.).
Common clavicular bone injuries:
- Injury. After mechanical impact, small vessels are damaged and a hematoma appears. With a severe injury, the hand becomes numb and mobility is limited.
- Dislocations. Damage to the outer edge is diagnosed more often than to the inner edge. The injury occurs when a person falls on an outstretched arm or shoulder. The dislocation is accompanied by pain, one of its ends protrudes from under the skin, and mobility is limited.
- A fracture is the most dangerous injury. In case of injury, the victim cannot raise the arm on the injured side, feels sharp pain, and swelling appears.
Non-mechanical pathologies include neuroma, osteochondroma, chondroma. With all of the above diseases, a benign growth appears on the bone, which provokes pain and decreased mobility.
Reference. Chondroma can develop into a malignant formation. Therefore, it is important to identify it in time and then carry out treatment.
Osteomyelitis of the clavicular bone is an infectious disease that manifests itself as pain, redness, and inflammation of the lymph nodes. Occurs due to injury, kidney disease, diabetes, etc.
Ewing's sarcoma is a malignant tumor. The pathology is accompanied by pain, swelling, sleep disorders, shortness of breath, loss of appetite, etc.
The most common injuries to the humerus include dislocations. This is due to the high mobility of the hand. The articular surfaces can shift anteriorly, posteriorly, downwards. When damaged, pain appears, swelling is observed in the affected area, and mobility is limited. If a nerve is pinched, the hand goes numb.
Common causes of a bone fracture: a blow, falling backwards on your elbows, or landing on your hands from a height.
Reference. Most often, a fracture of the humerus occurs in the area of the anatomical or surgical neck, condyles, head, and middle of the bone. The victim feels sharp pain, cannot move the injured limb, and after a while swelling and bruising appear. In addition, the bone in the damaged area is deformed.
Common non-mechanical pathologies of the humerus include osteomyelitis. The infection enters the bone marrow through the blood. Pathology is common, since the humerus is classified as tubular and has an abundant blood supply. If left untreated, bone tissue is destroyed, then fractures occur even as a result of minor external influences.
In addition, arthritis (degenerative-dystrophic changes) of the bony joint of the shoulder is common.
X-ray, MRI, and CT will help identify injuries or diseases of the bones of the upper limb girdle. To assess the general condition of the patient, laboratory tests of blood and urine are performed.
Dislocations are adjusted by a qualified health care professional. Treatment of fractures should be comprehensive: plaster casts, medications, exercise therapy, massage. In severe cases (displaced fractures), surgery is needed to compare bone fragments.
Infectious and inflammatory diseases are treated conservatively or surgically. It all depends on the severity of the pathology, the age of the patient, and his general health.
Diagnosis and treatment
First aid for injuries is to immobilize the injured limb in the position it assumed after the injury. You should absolutely not try to reset a dislocated joint or bone on your own to give it the correct position. After immobilizing (immobilizing) the affected arm, the victim should be given an anesthetic and/or antipyretic and immediately call an ambulance.
Treatment of such injuries is usually carried out at home after applying the basic techniques covered in the Standards of Medical Care in the field of Traumatology and Orthopedics (GEOTAR-Media, 2021, Moscow). After reduction of the dislocation, a tight bandage or plaster splint is applied. Surgery and hospitalization are necessary only in the case of a multiple comminuted fracture of the humerus or a fracture of the scapula of any complexity. Full recovery after a dislocation occurs in about 2 months; after a fracture of the scapula, this process can take up to six months. The treatment prescribed by the doctor and a complex of physical therapy exercises are of great importance.
If other pathologies are diagnosed, depending on the severity, conservative therapy (medicines, physical therapy) or surgery may be performed. Both methods are often prescribed. When the PP is affected by a tumor, therapy is carried out according to the techniques specified in the List of Federal Standards of Medical Care in the Oncology profile.