The hip joint is one of the most important in the musculoskeletal system. By supporting the weight of the entire body, the joint can withstand enormous overloads.
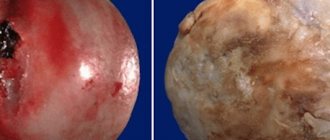
This is what the disease looks like.
It is presented in a spherical shape and allows the use of all axes of movement: adduction and abduction (sagittal axis), flexion and extension (frontal axis), pronation and supination (vertical axis). Due to its mobility, the joint is often damaged.
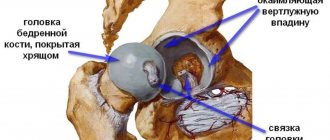
Structure of the hip joint
One of the most dangerous injuries is avascular necrosis of the femoral head (AFH). It is a consequence of a gross disruption of local microcirculation with the development of ischemia and necrotization of the bone marrow components of the femoral head. DDI is a consequence of previous operations on the hip joint, a history of trauma, previous osteomyelitis of the femur, and the development of epiphyseal and/or spondyloepiphyseal dysplasia.
We list several causes of vascular disorder leading to necrosis:
- repeated heart attacks due to arterial thrombosis;
- long-term insufficiency of arterial blood supply to the joint;
- venous stasis;
- combined disorder of the arterial-venous network.
The factors that provoke this situation are: congenital hypoplasia of the vessels of the hip joint, disruption of neurohumoral regulatory mechanisms, insufficient vascularization of the femoral head associated with the anatomical and functional immaturity of the vascular network.
Blood supply to the hip joint
Malnutrition of the bone components of the hip joint is the cause of necrotic changes.
Surgical intervention
It can be performed at different stages of aseptic necrosis and is used mainly in cases where traditional therapy methods do not bring the desired results. Several surgical methods can be used to treat ANFH:
- Decompression of the head of the bone or greater trochanter. Channels are drilled through the neck to the place of the head of the bone where blood circulation is not active enough. New vessels grow in these canals, pressure inside the bone decreases, blood flow normalizes and pain subsides.
- Osteotomy. A part of the fibula is transplanted to the affected area of the femoral head with the connection of the connecting arteries. This helps strengthen bone structures, restore blood flow and prevent further deformation.
- Endoprosthetics. During the operation, the destroyed joint is replaced with an artificial one. The femoral head is replaced with a ball with a titanium or zirconium pin. At the same time, a bed for the head is formed. The purpose of the operation is to restore mobility in the hip joint.
If the treatment was carried out correctly, the process of aseptic necrosis stops and does not progress further. The patient's condition stabilizes, unpleasant symptoms disappear, and the joint begins to function normally.
Symptoms and differences from coxarthrosis
The symptoms of ANFH are determined by the stages of the pathology. The onset is marked by asymptomatic symptoms or minor pain for no apparent reason. At the same time, the normal range of motion in the joint is maintained, pain is noted when the hip rotates inward.
The progression of the disease is expressed by paroxysmal, severe pain. Such a symptom may indicate the presence of collapse or fracture of the femoral head, inherent in the final stage of degenerative changes. They lead to a decrease in range of motion and the presence of constant pain, crepitus and instability of the femoral head.
The clinical symptoms of ANFH are similar to the classic picture of coxarthrosis:
- pain in the groin that runs along the anterolateral surface of the thigh and radiates to the knee joint. The load only intensifies these sensations, with the pain moving to the lumbar region. They always bother a person, even at night;
- the range of motion in the affected joint is noticeably limited. These people need help with self-care;
- severe lameness on the affected leg when walking;
- rapidly progressive hypotrophy of the muscular frame of the thigh on the affected side;
- shortening of the thigh.
Necrosis of the right hip joint
Risk of developing avascular necrosis due to trauma
One of the main reasons for the development of ANFH is fractures of the head or neck of the femur. The greatest risk is a transepiphyseal fracture (impaired blood supply to the proximal fragment up to 97.6%), subepiphyseal fracture (impaired blood supply to the proximal parts of the head up to 97.4%), subcapital fracture (impaired blood supply up to 92%).
There are several types of fractures:
Type 1: abduction, subcapital, incomplete fracture without displacement. It occurs due to the action of diverting tension. During a fracture, the neck and diaphysis of the femur are directed towards the head. The bone fragments are firmly wedged, and the fracture surface line is close to horizontal. The disturbance of blood supply is minimal (up to 10.2%). The prognosis for recovery is good.
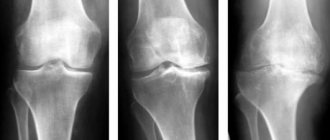
From left to right: subcapital, transcervical, basicervical fractures.
Type 2: adduction, subcapital, complete fracture without displacement. The fracture is located in a vertical plane, passing through the femoral neck. Trabeculae and lower cortex are torn, without displacement. Microcirculation is impaired by 23.6%. The prognosis is favorable.
Type 3: adduction fracture with incomplete displacement of bone structures. It is characterized by varus deformity of the femoral neck, but the fragments remain connected due to the posteroinferior block. The distal bone fragment is in a position of external rotation and abduction with an angle open anteriorly. There is a comminuted fracture of the posterior surface of the neck. The trabeculae and lower cortex are torn. Vascularization disorders reach 42.8%. Risk of developing avascular necrosis.
Type 4: adduction fracture with complete displacement. The head is deprived of all connections with the synovial membrane of the capsule, as a result of which the fragment becomes free. The disturbance of blood supply is maximum (54.4%). The risk of aseptic necrosis is increased.
To summarize: in the event of a potential injury to the hip joint, you must go to the nearest emergency room and have an x-ray taken. Early diagnosis can save the joint from destruction and maintain a high quality of life!
Minimally invasive endoprosthetics in the Czech Republic: doctors, rehabilitation, terms and prices.
Find out more
Reasons for development
There are many factors that can lead to the development of ANFH. These include:
- dislocations of the hip joint, fractures of the femoral neck and the head itself, as well as surgical interventions;
- long-term use of corticosteroids, especially those intended for systemic use (tablets);
- alcohol abuse, which leads to metabolic disorders;
- long-term use of painkillers and NSAIDs;
- autoimmune diseases, including scleroderma, hemorrhagic vasculitis, systemic lupus erythematosus;
- decompression sickness, characteristic of divers, miners and representatives of other professions, which require them to work in conditions of rapid decrease in the pressure of the inhaled gas mixture;
- radiation sickness or radiation therapy performed to suppress a malignant tumor;
- cauda equina syndrome, caused by entrapment of the spinal roots at the level of the lumbosacral vertebrae.
However, in approximately 30% of patients, it is not possible to determine exactly what exactly caused the development of ANFH.
ANGKB stages according to ARCO
However, in Russia the classification into five stages is more common:
- There are no radiological signs. The histological specimen shows signs of necrosis of the spongy substance of the head and bone marrow structures. Clinically expressed by aching pain and stiffness in the joint, increasing muscle weakness.
- multiple impression fractures. Against the background of necrosis, many microscopic fractures occur. The radiograph shows a homogeneous darkening of the femur, its height is reduced, the surfaces of the head in places are in the form of compacted facets, the joint space is widened. MRI data indicate a necrotic defect in the head.
- sequestration. The articular head is flattened and looks like structureless isolated fragments with different shapes and sizes. The neck of the bone shortens and thickens, and the joint space widens even more.
- reparative. The spongy substance of the femoral head is restored. On X-ray, sequestration-like zones are not noticeable; the shadow of the head is outlined, but with rounded cyst-like clearings.
- secondary deforming arthrosis. The bone structure of the femur begins to be traced, significantly changed, the congruence of the articular surfaces is disrupted.
Disease in dynamics.
Important: collapse of the femoral head occurs in an incredibly short period of time - 5 months.
Diagnostics
If you experience pain in the hip joint, it is important to contact an orthopedic traumatologist as soon as possible. This symptom may indicate the development of various joint pathologies, only one of which is ANKB. Therefore, the doctor must prescribe instrumental research methods:
- X-ray of the hip joint in 3 projections. The method makes it possible to establish not only the presence of ANKB, but also the stage of development of the disease. But it must be taken into account that at stage 1 there are no radiological signs of necrosis of the femoral head. This may cause a diagnostic error. Therefore, it is important to repeat the X-ray of the hip joint after six months.
- CT. It is prescribed, if necessary, to obtain layer-by-layer images of the hip joint and examine the characteristics of blood flow.
- MRI. The method allows you to detect the slightest changes in the condition of the hip joint, especially hyaline cartilage and other soft tissue structures.
- Densitometry. This diagnostic method makes it possible to measure bone density and detect signs of osteoporosis in the hip joint.
Additionally, biochemical blood and urine tests may be prescribed. The greatest attention is paid to the level of calcium, phosphorus, magnesium, DPID, pyridonine, osteocalcin.
Study of the blood circulation of the femoral head
Laser Doppler flowmetry and microsensory intraosseous pressure transducers are used. Histological examination makes it possible to diagnose the disease, differentiate it from other pathologies and determine the pathogenetic paths of development of the process.
As the disease progresses, the bone structure undergoes changes. In the subchondrial zone and the zone of necrosis, the activity of osteoclasts increases, and in the zone of sclerosis, on the contrary, the activity of osteoblasts increases.
With ANFH, laboratory parameters such as prothrombin time, aPTT (activated partial thromboplastin time) are normal. However, in a comparison of patients with non-traumatic necrosis and healthy volunteers, significant deviations in the concentration of coagulation factors in the blood plasma were revealed.
In people with ANFH, the level of ghrelin is reduced, the level of von Willebrand factor, plasminogen activator inhibitor-1 (PAI-1), and C-reactive protein is increased, which indicates the involvement of these factors in the mechanism of pathogenesis.
The use of certain laboratory parameters as markers for the diagnosis of ANFH is a promising method.
Treatment
For each stage according to ARCO, the duration of each of them is determined. For stage I and stage II - up to 6 months, stage III - 3-6 months and an immediate transition to stage IV.
Early initiation of treatment, while symptoms reveal only minor discomfort in the periarticular area with irradiation to the groin area and knee joint, is extremely important.
Tasks during the treatment period:
- For patients with a history of trauma, intoxication, and those at risk (taking glucocorticoids, cytostatics), use the diagnostic algorithm for ANFH in the early stages. It includes early clinical manifestations, information analysis of cardiac signals using the Screenfax system, MRI/CT, radiography, laboratory tests of markers of bone metabolism, scintigraphy, X-ray/ultrasound densitometry.
- Using a non-surgical treatment method, improve metabolic processes in the lesion, regenerate the elements of the femur and restore the function of the joint itself.
Taking into account the fact that ANFH is a multifactorial pathology, it is necessary to use an integrated approach in diagnosis, treatment and rehabilitation aimed at restoring:
- optimal functioning of all systems and organs;
- microvasculature and hemocoagulation parameters;
- neuroregulatory factors;
- immune reactions;
- myodiscoordinate processes and biomechanics of joints.
Treatment of stages 1-2
Seems most effective for a favorable prognosis. The most important condition for successful treatment is strict adherence to the regimen. You should give up bad habits (alcohol and smoking), avoid overloading and hypothermia of the affected joint.
Therapy is directed in several areas: medication, physiotherapy and exercise therapy.
Drugs . For aseptic necrosis, the following groups of drugs are prescribed:
- Bone resorption inhibitors (bisphosphonates). They slow down the destruction of bone tissue and prevent compression and deformation of the femoral head.
- Calcium and vitamin D preparations. In the form of active forms, they facilitate the formation of bone structures and their mineralization. The dose is selected individually.
- Additional sources of minerals and phosphates (ossein-hydroxyapatite).
- Since blood coagulation factors change in ANFH, antiplatelet drugs (chimes, dipyridamole, xanthinol) are necessarily prescribed.
- Non-steroidal anti-inflammatory drugs (NSAIDs). They have an analgesic and anti-inflammatory effect. The most commonly prescribed drugs are ibuprofen, ketoprofen, diclofenac and their analogues.
- Muscle relaxants to relieve muscle tension around the joint.
- Multivitamin complexes, chondroprotectors.
Physiotherapy. The main task is to stimulate blood flow in tissues and start/accelerate regenerative processes.
- a) hyperbaric oxygenation. The patient is placed in a pressure chamber, where he is exposed to air enriched with oxygen under conditions of high pressure. This procedure improves oxygen supply to the damaged area.
- b) shock wave therapy (SWT). Represents the action of a sound wave. It is carried out pointwise, certainly at the site of damage. It effectively affects pathological tissues that interfere with the healing of diseased joints (calcium crystals or adhesions). UVT improves blood supply to the treated area and thereby enhances the reparative effect.
- c) myostimulation. Allows you to restore muscle tone during developing hypotrophy, which is often found in ANFH. Stimulation relieves spasm of the muscle fibers surrounding the joint and accelerates local blood flow.
Physiotherapy
The initial stage is unloading the affected joint. In this case, the patient is fitted with crutches, which can take up to a year to walk on.
If after therapy the pain has decreased and bone turnover markers have returned to normal, crutches should be discontinued after 2-3 months. But don't rush. Unloading the joint will relieve pain and prevent further destruction of the femoral head. The gentle regime accelerates healing, it is faster and easier.
On the other hand, the patient needs exercise therapy. A special set of exercises will reduce pain and swelling of the joint and increase its mobility. Physical exercise will develop not only the joint, but also the muscles surrounding it, preventing the development of malnutrition.
Obese patients are advised to combine exercise with a specially selected diet. This combination will allow you to achieve better results.
The importance of physical therapy at the rehabilitation stage should be especially emphasized. It will help not only to develop the operated/replaced joint, but also to prevent its instability.
Final diagnosis and MRI
The degree of damage to the hip joint is determined by a comprehensive diagnostic method. When diagnosing, the severity of the disease is noted according to the international ARCO system.
- ARCO 0. Result negative;
- ARCO I. Detection of necrosis by MRI and cintigraphy;
- ARCO II. Detection of necrosis on X-ray and CT. Minor decalcification was detected;
- ARCO III. CT and x-rays reveal a break under the cartilage and deformation of the femoral head;
- ARCO IV. The MRI shows signs of wear on the joint.
- ARCO I and II, as mentioned above, are amenable to therapeutic treatment.
- ARCO III and IV require surgery.
Treatment of stages 3-4 necrosis
If the joint has already entered these stages, then the process of destruction of the femoral head has already begun. Exercise therapy and physiotherapy remain in the same vein as in the initial stages, but drug therapy undergoes changes. This is due to severe pain that patients can no longer tolerate. Stronger painkillers (diclofenac, tramadol) are prescribed.
The therapeutic effect is complemented by intra-articular injections of hyaluronic acid and the introduction of platelet-rich plasma.
Hyaluronic acid is an important component of synovial fluid. Such injections improve the shock absorption of congruent surfaces and facilitate their sliding relative to each other.
PRP.
PRP therapy (injection of platelet-rich plasma) activates the healing process. This is a young but promising direction. Under the influence of platelets, the production of collagen (the main “building material” of cartilage, connective and bone tissue) increases. Integration of osteoblasts occurs, helping to build new tissue, microcirculation improves due to the formation of new vessels.
Important: despite the breadth of possibilities of modern medicine, conservative treatment is effective only in the early stages. At the first signs of destruction of the head, the joint cannot be restored.
In this situation, a decision will be made regarding surgical intervention. Basic combinations of groups of surgical techniques [14]:
- intertrochanteric corrective osteotomy;
- modeling of the femoral head, including with intertrochanteric corrective osteotomy;
- modeling of the femoral head with autoplasty, including intertrochanteric corrective osteotomy;
- subchondral autoplasty of the femoral head, including intertrochanteric corrective osteotomy;
- segmental autoplasty of the femoral head, including intertrochanteric corrective osteotomy;
- reconstruction of the pelvic components, namely: pelvic osteotomy according to Chiari, including with intertrochanteric corrective osteotomy, supraacetabular acetabuloplasty, including with intertrochanteric corrective osteotomy.
No operation guarantees a full recovery. They reduce destructive processes inside the joint and reduce the risk of developing secondary coxarthrosis.
What happens in the bone?
As a result of circulatory disorders, bone cells die, because the blood vessels supplying the head remain blocked.
As a result, the supply of oxygen, minerals and nutrients to the bone of the hip joint is very limited.
The main function of bone cells is to maintain a balance between the decrease and increase of bone during the process of its adaptation to changing loads. The dead bone tissue of the hip joint can no longer support this natural process.
As a result, the bone beams lying inside the bones, which are responsible for the stability and shape of the femoral head, are no longer renewed: the bones affected by necrosis break due to insufficient strength. A hole forms in the bone under the cartilage! The underlying cartilage can be severely damaged and there is a risk of arthrosis of the hip joint! The result is irreversible damage to the joint and bone mass.
Comparing with the frozen surface of a lake, where the ice breaks where its layer is not thick enough, the bone also breaks in the thinnest place.
The biggest problem with femoral head necrosis is that the disease affects the regions adjacent to the joint and therefore leads to joint destruction. Bone infarcts, for example, which are often diagnosed incidentally on x-rays, lie within the bone away from the joint and therefore do not play a major role.
If left untreated
Aseptic necrosis of the head of the hip joint is a severe pathology that will not resolve on its own. If the situation is left without proper attention, the disease can lead to disability. In one case, secondary coxarthrosis may develop, requiring replacement of the joint with a prosthesis (hip arthroplasty). During the operation, the head of the hip joint is removed along with part of the femur and a prosthesis is placed in its place.
Joint replacement allows you to count on a favorable prognosis. The prosthesis allows you to completely restore lost functions.
Another outcome of the disease can be ankylosis - complete immobility in the joint. Complete degeneration of the cartilaginous cover of the articular surfaces occurs with the proliferation of connective fibrous or bone tissue.
Diet
Diet for sore joints
- Efficacy: therapeutic effect after 2-3 months
- Terms: 2-6 months
- Cost of products: 1700-1800 rubles. in Week
Nutrition should be complete. It is important to introduce foods into your diet that provide the body with vitamins, minerals, and collagen .
- There should be more dishes with gelatin in the diet.
- It is recommended to limit the amount of salt you consume.
- It is better not to eat fried, smoked, fatty foods; sweets should also be kept to a minimum.
- It is advisable to eat fractionally - more often and in small portions.
- Protein foods should dominate the diet.
Useful products for aseptic necrosis are:
- Dishes with gelatin.
- Berries, vegetables, fruits.
- Dried fruits.
- Porridge.
- Honey.
- Low-fat dairy products.
- Offal.
- Fish and seafood.
Disability
ANGKB affects all areas of life: health, performance, socialization. With a long duration of the disease at different stages of conservative treatment, patients were forced to change activities with increased physical activity. They choose professions that do not require long periods of being on their feet, moving, or close to their place of residence.
The disability group of such people is determined during a medical and social examination in accordance with the Appendix to the Order of the Ministry of Health of the Russian Federation dated January 27, 1977 No. 33 to the Resolution of the Ministry of Labor and Social Development of the Russian Federation dated January 27, 1977 No. 1: “Classifications and temporary criteria used in the implementation of medical social expertise".
Disability is assigned based on the severity of the disease and decreased quality of life. Changes in the level of disability were carried out only in the case of surgical intervention.
In other words, surgical intervention is most effective in treating aseptic necrosis. Despite the impressiveness of conservative treatment methods, proven effectiveness is questionable.
Where can you undergo surgical treatment of necrosis of the femoral head?
The German Medical Group offers patients the opportunity to choose where to receive treatment in clinics specializing in the treatment of affected joints. We will help you choose among experienced specialists who have received high ratings from patients who have undergone treatment, we will take care of all bureaucratic issues, organize your stay at the clinic, treatment and full support for the patient. Do not waste time on herbal medicine, restore your functionality with modern and effective methods of treating advanced stages of necrosis.
Also, in the absence of a complete diagnostic picture of the disease, we are ready to offer you the opportunity of remote consultation with leading orthopedists in Germany, Austria and Switzerland.
To establish contact with a German Medical Group specialist, fill out the website application form below. We will help you organize treatment, or remotely obtain a second opinion from a doctor.