Styloiditis of the wrist
Styloiditis is an inflammation of the styloid process (from the Latin processus stiloideus) of the radius or ulna.
Accordingly, depending on which process is inflamed, the disease is called ulnar or radial styloiditis. The olecranon process is located on the lateral surface of the wrist joint on the little finger side, and the radial process is located on the thumb side. They are palpated as bone “bumps” in the indicated areas.
Actually, it is not the process itself that becomes inflamed, but the places where the ligaments and tendons attach to it or the tendon sheaths. The disease is also called “wrist styloiditis”.
Styloiditis of the radius (De Quervain's disease) occurs most often, because in this area is the tendon sheath of the abductor pollicis muscle, the narrowing of which predisposes to the onset of the disease.
Causes
Styloiditis appears due to regular overload of the joints as a result of daily monotonous work. The disease is occupational for certain groups of people. These include volleyball players, conductors, miners, milkmaids, programmers, that is, people who perform the same hand movements day after day.
Monotonous work associated with constant tension in the tendons of the hand or elbow leads to the appearance of microtraumas that do not have time to heal. As a result, the nerve fibers become torn and become inflamed, leading to a narrowing of the canal and pinching of the vessels and the median nerve passing through it. Because of this, inflammation occurs and styloiditis develops.
In addition to regular tendon overload, provoking factors that lead to the onset of the disease are:
- arthritis;
- diabetes;
- gout.
Severe injuries to the wrists and elbows also lead to inflammation and fibrous degeneration of the ligaments. This provokes loss of motor activity of the joints, impaired ability to do flexion and extension.
Radiation styloiditis
The main manifestation is pain. It occurs in the area of the wrist joint on the radial side (thumb side). Pain can occur either acutely (for example, due to injury) or increase gradually (with chronic overload). Characteristically, there is pain when moving the wrist joint or thumb. Pain at rest is much less common and can occur with very severe inflammation or with a chronic long-term course of the disease.
There are usually no changes upon external examination. In rare cases, a slight swelling may be found above the styloid process. There is practically no redness of the skin.
Palpation in the area of the styloid process is painful. Movement in the wrist joint and/or thumb is moderately painful.
There are several tests for diagnosing radial styloiditis.
Symptoms
Styloiditis develops slowly, without showing clear signs for a long time. A person, after performing long-term monotonous work associated with movements of the elbows or wrists, feels slight discomfort, fatigue, stiffness, and heaviness. But after a short rest, all signs disappear.
This goes on for a long time. But this does not mean that the inflammation has disappeared. It exists and gradually the inflammatory process provokes the appearance of scar tissue on the ligaments, which in turn leads to poor circulation in the elbow or hand. The vascular bundle through which nerve impulses pass is gradually compressed. As a result of disruption of innervation, the affected area constantly becomes numb, and the functioning of the upper limb worsens. With constant loads on the joint and tendons, salt deposits appear at the site of the microfracture; the tissue located between the tendons becomes ossified, and spines and bone growths form in its place.
The main symptoms of styloiditis include:
- constant aching pain in the elbows, fingers, wrists, worsening at night or after physical exertion;
- swelling and redness of the affected joint;
- periodic loss of sensitivity of the limb, disturbance of its motor activity;
- aches and pains when weather conditions change;
- crunching when moving joints;
- swelling of the affected area, redness of the skin in this area;
- the occurrence of piercing pain when trying to move the thumb to the side;
- difficulties when trying to work with small objects (if the radius is affected).
If you leave everything to chance and do not consult a doctor, styloiditis will gradually become chronic. The tendons will begin to thicken and calcify. All this contributes to a deterioration in blood supply to the joint, the appearance of increasing pain, and a reduction in motor activity.
Ulnar styloiditis
Local symptoms with styloiditis of the ulna are similar to those with radiation injury. One of the differences is that pain with ulnar styloiditis can radiate to the 4th and 5th fingers of the hand. This is due to pinching of the ulnar nerve in the inflamed tissue. There is also a difference in diagnostic tests.
The finger test and the Filkenstein test are not performed for this disease. When performing a test with abduction of the palms, pain and limitation of movements will occur when abducted to the radial side (towards the thumb).
Who is more likely to get De Quervain's tendinitis?
As a rule, the occurrence of tendonitis in the wrist is associated with an increase in the load on the hand. Athletes who have started working with heavier weights often seek help. First-time mothers often come with similar complaints. They also have a significant increase in the load on their hands; when lifting a child by the armpits, the muscles of the radial side of the forearm become very tense, and their overload may occur. However, it is not always possible to find a clear connection with the load; tendon slip may worsen due to systemic diseases (rheumatoid arthritis, gout, etc.), and an increase in the frequency of tendinopathies is noted in women after 45 years. This may be due to hormonal changes in the body.
Treatment
Treatment of styloiditis of the styloid process when affected on the radial and ulnar sides is the same and includes:
- Load limitation
- The use of non-steroidal anti-inflammatory drugs (NSAIDs) orally and locally
- Blockades with diprospan or kenalog
- Physiotherapy
- Kinesio taping
It is recommended to remove loads for 1-2 months. As for drug therapy, for wrist styloiditis they begin with taking anti-inflammatory drugs (NSAIDs) orally (Voltaren, Nimesil, etc.) with simultaneous local application (Voltaren-gel, Indovazin-gel).
At the same time, the therapy can be supplemented with kinesio taping and physiotherapy. If therapy is ineffective within 7 days, blockades with diprospan are prescribed (from 1 to 3 with an interval of 5 to 7 days). If the pain syndrome is significantly severe, blockades can be started immediately, without waiting for the effect of NSAIDs.
In general, styloiditis responds well to treatment, but in some cases the disease becomes chronic. For frequent exacerbations that are difficult to treat, surgical intervention may be indicated.
Diagnostics
There are no specific symptoms of styloiditis that could accurately diagnose the disease. Therefore, the doctor is obliged to refer the patient for differential studies:
- Echography;
- X-ray;
- MRI;
- CT;
- Urine and blood tests;
- Ultrasound.
Using the above studies, it is possible to differentiate radiation styloiditis from other diseases that have similar symptoms (aching pain in the wrist, for example).
The reason for ordering additional examinations is:
- Age of the patient;
- His profession;
- Previous injuries to the wrist area.
The risk group includes people over 35 years of age who work:
- On construction;
- In the mines;
- At sewing enterprises;
- Typists;
- Milkmaids, etc.
Nodular tenosynovitis of the finger flexors.
The finger flexor tendons or annular ligament in the area of the interphalangeal joints are affected
. The “snapping finger” syndrome develops, which is associated with the appearance of a nodule on the flexor tendon (a consequence of a primary or secondary dystrophic-inflammatory process), which makes it difficult for the tendon to slide into the vagina at the level of the fibrous canals in the joint area, and then completely blocks movement. Typical complaints from the patient include a clicking sensation when bending and straightening the finger. As the process progresses, the finger freezes in the position of flexion or extension contracture. Upon examination, a nodule is palpated on the palm or palmar surface of the finger in the projection of the flexor tendon.
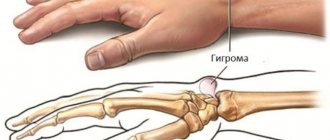
G english (hygroma) is a nodule, the size of a pea or slightly larger, located on the back of the hand or in the area of the wrist joint in the projection of the extensor tendon sheaths. It is a hernial protrusion of the synovial vagina. Pain or discomfort occurs when moving your fingers. The contents of the ganglion are synovial fluid.
Exudative tenosynovitis of the extensor fingers
Exudative tenosynovitis of the extensor fingers often accompanies inflammatory arthropathy of the hand area. It manifests itself as limited swelling on the back of the wrist joint. A differential diagnosis is made with arthritis of the wrist and radio-elbow joints, which are also accompanied by swelling of the dorsum of the hand. To do this, ask the patient to bend and straighten the hand. With extensor tendovaginitis, during extension of the hand, the swelling moves distally, repeating the movement of the tendons.
Stenosing tenosynovitis
With tenosing tenosynovitis of the long abductor and short extensor of the 1st finger (De-Creven's disease). The tendons of the long abductor and short extensor of the 1st finger pass in the 1st canal of the dorsal ligament. The narrowing of this canal due to inflammatory phenomena leads to compression of the tendons and the development of the clinical picture of De Crevin's disease. Currently, the disease occurs in young women in the first months after childbirth (a sharp increase in household workload) and in patients with hypermobility syndrome in the 2nd half of life. The clinic consists of the appearance of attacks of severe pain in the area located 1.5-2 cm above the base of the 1st finger (“anatomical snuffbox”). You can also see swelling in this place.
Radiation styloiditis
Radial styloiditis is a tendoperiostitis of the long supinator tendon of the forearm at the site of its attachment to the styloid process of the radius. Mostly women aged 40-60 years are affected (most often dressmakers). Styloiditis is usually right-sided, which indicates the importance of frequent microtrauma due to the characteristics of professional activity. The main clinical sign is pain in the area of the styloid process of the radius (slightly above the inner edge of the wrist joint), which intensifies with supination of the forearm. Local swelling is often found in this area.
Ulnar styloiditis
L ulnar styloiditis is tenosynovitis of the extensor ulnaris or stenotic ligamentitis of the 4th canal of the dorsal ligament of the hand, in which the tendon of the extensor ulnaris passes. Radiation styloiditis is much less common. The cause of the disease is trauma to this area or professional microtraumatization (for seamstresses, typists, etc.).
Clinically - spontaneous pain in the area of the styloid process of the ulna, intensifying with radial abduction of the hand and radiating to the 4th-5th finger. A local painful swelling is palpated above the styloid process.
Carpal tunnel syndrome.
With pressure on the median nerve under the transverse carpal ligament. The compression of the nerve occurs between three bony walls and a tight ligament that hold the tendons of the muscles that flex the fingers and hand.
Diseases of this group are found in many professions, including such industries as construction, mining, engineering, and agriculture. They are caused by chronic functional overstrain, microtraumatization, and the performance of fast, similar movements.
The carpal tunnel is located at the base of the hand and is surrounded on three sides by the carpal bones and in front by the transverse carpal ligament. This canal contains the median nerve, the flexor tendons of the fingers and hand, as well as the synovial membranes of these tendons.
The sheath of tendon is a sheath of connective tissue that surrounds part of the tendon. In the gap between this sheath and the tendon there is a small amount of lubricating fluid to reduce friction (synovial fluid), which is produced by synovial cells (lining the cavity of the sheath from the inside).
The transverse carpal ligament is a strong cord of dense connective tissue, which is attached on one side to the ulnar eminence and the other to the radial eminence of the wrist. It turns the carpal groove into the carpal tunnel, which contains the digital flexor tendons and the median nerve.
The radius nerve is one of the three main nerves of the arm (the other two are the radial and ulnar nerves). It originates from the brachial plexus. On the hand, this nerve supplies sensory fibers to the skin of the tubercle of the thumb, the palmar surface of the thumb, index, middle and half of the ring finger and fibers of internal sensitivity to some muscles of the hand (responsible for coordinating the movements of these muscles), motor fibers to these muscles of the hand, as well as vegetative fibers to local arteries (affects the constriction and dilation of blood vessels, for example, depending on temperature) and sweat glands.
syndrome is caused primarily by compression of the median nerve at the wrist due to thickening or swelling of the flexor muscle synovium. As a result of chronic inflammation of the connective tissue due to constant repetitive stress, it becomes rougher, thicker, and swollen, which increases the pressure inside the carpal tunnel. Increased pressure causes venous congestion and edema, which leads to ischemia (impaired blood supply) to the nerve.
Clinical manifestations of carpal tunnel syndrome.
Numbness and tingling . Most often, patients complain of “switching off” their hands or that objects fall out of their hands against their will, as well as numbness and a “tingling” sensation on the skin of the hand, usually in the thumb, index, middle and, sometimes, ring fingers. Symptoms tend to be intermittent and associated with specific activities (eg, driving, reading a newspaper, drawing). Due to the resulting numbness and pain, the patient is sometimes unable to hold on to the upper handrails in public transport; talk on the phone for a long time, which is why he has to change the receiver to his other hand; hold the steering wheel of a car for more than 10 minutes while driving; read a book or newspaper, holding it in front of you, etc.
Pain . The above-described sensitivity disorders are often accompanied by burning pain on the palmar surface of the wrist and in 1-3 or 1-4 fingers of the hand. The pain may spread (“transfer”) toward the palm and fingers, or, more commonly, toward the palmar surface of the forearm. Pain in the area of the epicondyles of the elbow joint, shoulder or neck is often associated with other lesions of the musculoskeletal system, which are sometimes combined with carpal tunnel syndrome.
The place where symptoms are felt. Complaints usually concern the palmar surface of the first to fourth fingers and the adjacent palm (which corresponds to the zone of innervation of the palm by the median nerve). If the numbness occurs mainly in the little finger or extends to the back of the hand, this indicates another disease. In many patients, numbness extends higher due to damage to the autonomic nerves.
Night symptoms . Carpal tunnel syndrome is characterized by nocturnal symptoms that may cause the patient to wake up, especially if the patient is able to relieve them by shaking the hand and wrist. The patient may find relief from lowering and rubbing his arms, swinging them in a lowered position. You may feel stiffness in your fingers in the morning.
The affected side. Bilateral involvement is common, although the dominant hand (ie, the right hand in a right-handed person, the left in a left-handed person) is usually affected earlier and more severely than the other hand.
Autonomic symptoms . Often patients have complaints regarding the entire hand. Many patients with carpal tunnel syndrome also report a feeling of tightness and swelling in the hands and/or changes in temperature (i.e., persistently hot or cold hands). This is due to local dysregulation of vasoconstriction/dilation. Some patients experience sensitivity to changes in ambient temperature (usually cold temperatures) and changes in skin color. In rare cases, local sweating disorders occur. All these symptoms are associated with damage to autonomic fibers (the median nerve carries autonomic fibers for the entire hand).
Weakness/imprecision of movements . Patients with carpal tunnel syndrome experience loss of muscle strength in the hand (particularly when gripping with the thumb); however, in practice, loss of feedback due to sensory impairment and pain are more important causes of weakness and imprecision of movement than loss of motor function itself. At the same time, coordination of movements and hand strength are impaired (“everything falls out of your hands”).
If left untreated, carpal tunnel syndrome can lead to complete, irreversible damage to the median nerve, followed by severe impairment of hand function.
Do you have pain in the hand area? Come, we will help you! appointment with a rheumatologist for an appointment and therapeutic blockade in Samara by calling the phone number on the contacts page.