© sementsova321 — stock.adobe.com
Share:
Shoulder and arm rotations are a necessary warm-up exercise before any strength training or morning exercise. They prepare joints and ligaments well for stress. Most training injuries are due to lack of warm-up.
Do not forget that in addition to the joints, you also need to prepare the muscles for work - for this, warm-up approaches are performed with light weights.
Shoulder, shoulder girdle and shoulder joint[edit | edit code]
The shoulder girdle consists of the collarbone and scapula. The proximal end of the clavicle forms with the sternum the sternoclavicular joint, the only joint connecting the shoulder girdle with the axial skeleton. This joint is strengthened by the anterior and posterior sternoclavicular, costoclavicular and interclavicular ligaments. The distal end of the clavicle and the acromion form the acromioclavicular joint, which is strengthened by the coracoclavicular and acromioclavicular ligaments.
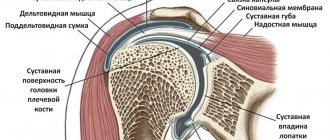
The glenoid cavity of the scapula and the head of the humerus form the shoulder joint. This is a very mobile and therefore rather fragile spherical joint, reinforced by the articular labrum, articular capsule and articular-brachial ligaments.
Movements of the arm in the shoulder joint (Fig. 5.1) occur under the action of many muscles. Flexion is carried out by the clavicular part of the pectoralis major muscle and the anterior part of the deltoid muscle. Extension occurs due to contraction of the latissimus dorsi muscle, teres major muscle and the sternocostal part of the pectoralis major muscle. Abduction is provided by the deltoid muscle and the rotator cuff muscles (subscapularis, supraspinatus, infraspinatus and teres minor). Adduction occurs due to the contraction of the pectoralis major muscle (sternocostal part), the latissimus dorsi muscle and the teres major muscle. The subscapularis and pectoralis major muscles internally rotate the humerus, while the supraspinatus, infraspinatus and teres minor muscles externally rotate the humerus. Horizontal adduction is accomplished by simultaneous contraction of the coracobrachialis, pectoralis major, and anterior deltoid muscles, and horizontal abduction is accomplished by contraction of the infraspinatus, teres minor, and posterior deltoid muscles.
Figure 5.1.
Range of motion in the shoulder joint.
A.
Flexion and extension.
B.
Abduction and adduction.
B.
Rotation outwards and inwards.
D.
Horizontal abduction and adduction.
Figure 5.1
(end). Range of motion of the scapula.
D.
Raising and lowering.
E.
Outward and inward rotation.
G.
Abduction and adduction.
The rotator cuff is the muscles immediately adjacent to the capsule of the shoulder joint (subscapularis, supraspinatus, infraspinatus and teres minor).
Simultaneously with the movements in the shoulder joint, movements of the scapula occur, namely its abduction, adduction, rotation outward or inward, as well as elevation and descent. Abduction of the scapula is carried out by the pectoralis minor and serratus anterior muscles, adduction by the rhomboid muscles, rotation of the lower angle outward by the serratus anterior and trapezius muscles, rotation of the lower angle inward by the pectoralis minor and rhomboid muscles, elevation by the levator scapulae muscle, and descent by the pectoralis minor muscle. .
How to do the exercises?
All movements are performed with straight legs standing shoulder width apart.
Forearms
The arms are positioned at right angles to the body. The movement is carried out in a circle, the center is at the elbow. The number of repetitions is 30 times towards yourself and away from you. Do not do the exercise in jerks, start smoothly and speed up a little towards the end.
Hands
In this variation, the arms rotate completely with maximum amplitude relative to the body. The brush rotates 360 degrees. You should perform 20 repetitions from yourself and to yourself, as well as a similar number of simultaneous rotations in different directions.
Shoulders
The arms are parallel to the body and motionless; only the shoulder muscles work. Repeat 20 times in the direction away from you and towards you.
Read also[edit | edit code]
- Examination (arthroscopy) of the shoulder joint
- Damage (tear) of the rotator cuff
- Subacromial bursitis
- Biceps tendinitis
- Biceps rupture
- Torn pectoralis major muscle
- Shoulder instability
- Shoulder dislocation: symptoms, treatment
- Labral rupture
- Shoulder capsulitis
- Clavicle fracture: symptoms, treatment
- Humerus fracture
- Clavicle dislocation
- Brachial plexopathy
- Long thoracic nerve neuropathy
- Suprascapular nerve neuropathy
- Musculocutaneous nerve neuropathy
- Axillary nerve neuropathy
- Thoracic outlet syndrome
Exercises for shoulder capsulitis
This disease most often develops gradually, but doctors distinguish three degrees of the disease. The first is accompanied by acute pain and partial limitation of mobility of the shoulder joint. The pain is especially severe at night, when at rest. In the second stage, joint stiffness and pain intensify, and the range of motion is reduced to a minimum. The third stage, subject to proper treatment, moves into the stage of improvement. The high-risk group is quite large - people over forty years old, especially women with diabetes, heart disease, and vascular disease. The exact causes of this disease are still unknown, but most often it occurs in those who have previously received any kind of shoulder injury.
The simplest ways to treat this disease are compresses, a course of anti-inflammatory drugs, physiotherapy, and, in extreme cases, surgery. In ordinary cases, patients manage without surgery.
To prevent shoulder capsulitis and treat sprains, a whole set of simple but very effective exercises has been developed. It is worth remembering that in the acute stage of the disease, exercises should be performed with caution, only after consulting the attending physician.
Exercise "Pendulum"
The exercise is indicated for performance after injuries, but with the permission of a specialist. As a result of its implementation, the muscles are stretched and pressure on the tendons is relieved.
The pendulum is performed as follows. Stand up straight, relaxing your shoulders and back. Leaning forward, let your arms hang freely and begin to slowly swing them to the right - left, first clockwise, then counterclockwise, increasing the number of repetitions every day.
Exercise with a towel
This exercise helps restore shoulder mobility by reducing stiffness around the shoulder. You need to prepare a rolled towel about a meter long. We stand up straight, straightening our back, with our right hand we carry the towel behind our back over our shoulder, and with our left we grab it from below. We stretch the shoulder by pulling the towel together with the other hand up and down, creating slight resistance.
Stretching the back and shoulder muscles
This exercise stretches the lateral deltoid muscles, relieving overall tension. You can exercise either sitting or standing, as convenient. Bend your right arm at the elbow, raising it to chest level. With your left hand, carefully raise your bent elbow, stretching the muscles. We stay in this position for a few seconds. Repeat with your left hand.
Back stretch
This stretch will help relax your back muscles while releasing tension in your shoulder girdle. We stand in front of the surface, which is at chest level. Place one hand on the surface and squat a little, stretching the muscles in the armpit area. Perform several squats, each time trying to squat lower and lower. Do the exercise on the other side.
Hand movements
Circular movements of the arms increase the range of motion of the shoulder, accelerate blood flow in the tissues, which helps restore joints. We sit down on a hard surface. Bend your right arm at the elbow, placing your hand on your right shoulder. We perform circular movements, first clockwise, then counterclockwise.
Hands behind your back
We stand up straight, clasp our hands behind our backs. Slowly raise your clasped hands up. Alternatively, you can lean forward a little while raising your arms. Stop at the highest possible point and hold for a few seconds.
Shoulder Curl
The exercise is designed to reduce stiffness, discomfort and prevent capsulitis.
You will need elastic bands that need to be secured above head level. We stand up straight, holding the ends of the tape in our hands. Starting position – hands down. Slowly raise our arms one at a time, holding them in the raised position. Repeat several times with both hands. Author: K.M.N., Academician of the Russian Academy of Medical Sciences M.A. Bobyr
muscles involved in various types of movement of the upper end
Laboratory lesson
"Muscles of the upper limb"
Muscles that
produce movements of the upper limb
. Schematically, the movements of the upper limb girdle (scapula and clavicle) are divided into:
- Movement forward and backward with abduction of the scapula from the spinal column and adduction to it.
- Raising and lowering the scapula and clavicle.
- Movement of the scapula around the sagittal axis with the lower angle to the medial and lateral sides.
- Circular movement of the lateral end of the clavicle and at the same time the scapula.
These movements involve six functional muscle groups.
Forward
movement The forward movement of the upper limb girdle is produced by the muscles that cross the vertical axis of the sternoclavicular joint and are located in front of it. These include:
- pectoralis major, acting on the girdle of the upper limb through the humerus;
- pectoralis minor;
- anterior serratus.
backward
movement is carried out by the muscles that cross the vertical axis of the sternoclavicular joint and lie behind it. This muscle group includes:
- trapezius muscle;
- rhomboid muscle, major and minor;
- latissimus dorsi muscle.
Upward
movement Raising the belt of the upper limb is performed by the following muscles:
1) the upper bundles of the trapezius muscle, which pulls up the lateral end of the clavicle and the acromion of the scapula;
- levator scapulae muscle;
- rhomboid muscles, during the decomposition of the resultant of which there is a certain component directed upward;
- the sternocleidomastoid muscle, which, attaching one of its heads to the collarbone, pulls it, and, consequently, the scapula upward.
Downward
movement Lowering is facilitated by muscles that go from bottom to top, from the chest or spinal column to the bones of the upper limb girdle:
- pectoralis minor muscle;
- subclavius muscle;
- lower bundles of trapezius muscle;
- inferior teeth of the serratus anterior muscle.
In addition, the muscles that go from the torso to the shoulder, namely the pectoralis major muscle and the latissimus dorsi muscle, help lowering, mainly through their lower parts.
Rotation of
the scapula ( movement of the lower angle inward and outward )
Rotation of the scapula inward, with the lower angle to the spinal column, produces a pair of forces formed by:
- pectoralis minor muscle
- the lower part of the rhomboid major muscle.
Rotation of the scapula outward, with the lower angle from the spinal column to the lateral side, occurs as a result of the action of a pair of forces generated by the upper and lower parts of the trapezius muscle.
This movement is supported by:
- serratus anterior muscle with its lower and middle teeth;
- teres major muscle with a fixed free upper limb.
Circular
movement
Circular movement of the upper limb girdle occurs as a result of alternate contraction of all its muscles.
Muscles
producing movements in the shoulder joint
, movements around three mutually perpendicular axes are possible:
- abduction and adduction around the anteroposterior axis;
- flexion and extension around the transverse axis;
- pronation and supination around the vertical axis;
- circular motion (circumduction).
These movements are provided by six functional muscle groups.
Shoulder
abduction The shoulder abductor muscles cross the sagittal axis of rotation at the shoulder joint and are located lateral to it. The humerus is abducted by the following muscles:
- deltoid and
- supraspinatus.
Shoulder
adduction There are no special muscles that would cross the sagittal axis of the shoulder joint and are located medial to it, therefore shoulder adduction according to the parallelogram of forces rule is carried out with simultaneous contraction of the muscles located in front (the pectoralis major muscle) and behind the shoulder joint (the latissimus and teres major) . These muscles help:
- infraspinatus;
- small round;
- subscapular;
- long head of the triceps brachii muscle;
- coracobrachial muscles.
Shoulder
flexion The shoulder flexor muscles cross the frontal (transverse) axis of the shoulder joint and are located in front of it.
Shoulder flexion (moving it forward) is produced by the following muscles:
- deltoid, its anterior part;
- pectoralis major;
- coracobrachial;
- biceps brachii muscle.
Shoulder
extension The muscles that perform shoulder extension (moving it backwards) cross, like the shoulder flexors, the frontal axis of the shoulder joint, but are located behind it. Shoulder extension is produced by the following muscles:
- its deltoid posterior part;
- latissimus dorsi muscle;
- infraspinatus;
- small round;
- large round;
- long head of the triceps brachii muscle.
Shoulder
pronation Shoulder pronation, i.e. turning inward, produced by muscles; which cross the vertical axis of the shoulder joint, attaching in front of it. These include:
- subscapular;
- pectoralis major;
- deltoid, its anterior part;
- latissimus dorsi muscle;
- large round;
- coracobrachial.
Supination
of the shoulder
Supination, i.e. turning the shoulder outward is produced by muscles that, like the pronators, cross the vertical axis of the shoulder joint, but are located behind it:
- posterior deltoid muscle
- teres minor
- infraspinatus muscle
- biceps brachii
Forearm
flexion Forearm flexion is produced by muscles that cross the transverse axis of the elbow joint and are located in front of it. These muscles include:
1) biceps brachii;
2) shoulder;
3) brachioradialis;
4) pronator teres.
Brachial muscle -
when flexing the forearm, the muscle clearly protrudes and can be easily felt above the skin. This muscle is not only a flexor of the forearm, but also a supinator (if the forearm is pronated), and if it is supinated, then it is a pronator.
Pronator teres –
participates in two movements of the forearm: flexion and pronation.
Circular
movement of the shoulder
With the alternate action of all the muscles located in the circumference of the shoulder joint, a circular movement occurs in it. Looking at these muscles, it is easy to notice that they lie unevenly, namely: there are no muscles inside and below this joint, instead there is a depression called the axillary fossa.
Axillary fossa
its shape is somewhat reminiscent of a pyramid, with its base facing downward and outward, and its apex upward and inward. It has three walls, of which the anterior one is formed by the pectoralis major and minor muscles, the posterior one by the subscapularis, teres major and latissimus dorsi muscles, and the inner one by the serratus anterior muscle. In the depression between the anterior and posterior walls lie the coracobrachialis muscle and the short head of the biceps brachii muscle.
Muscles producing
movements in the elbow joint
In the elbow joint with a fixed shoulder, the following are possible :
- flexion and extension of the forearm;
- pronation and supination of the forearm.
Extension of
the forearm
Extension of the forearm is performed by the muscles that cross the transverse axis of the elbow joint and are located behind it. There are two of these muscles:
- triceps brachii and
- ulna.
Pronation
of the forearm
The muscles that produce pronation of the forearm are:
- pronator teres
- pronator quadratus
- brachioradialis muscle.
Supination
of the forearm
The supinators of the forearm are:
- biceps brachii
- supinator muscle
- brachioradialis muscle.
Muscles that
produce movements in the wrist joint and the joints of
flexion. Wrist flexion
involves
muscles that cross the transverse axis and are located in front of it on the anterior surface of the forearm and hand. These include:
1) long palmar;
- flexor carpi radialis;
- flexor carpi ulnaris;
- flexor digitorum superficialis;
- flexor digitorum profundus;
- flexor pollicis longus.
Extension of
the hand
Extension of the hand is produced by muscles that cross the transverse axis of the wrist joint and are located behind it on the back surface of the forearm. These muscles are multi-articular. They produce simultaneous extension in all joints around which they pass. These muscles include:
- extensor carpi radialis longus;
- extensor carpi radialis brevis;
- extensor carpi ulnaris;
- extensor digitorum;
- extensor of the little finger;
- extensor index finger;
extensor pollicis longus.
Adduction
of the hand
There are no muscles located on the medial surface of the ulna and extending onto the hand strictly along the medial surface of the wrist joint. The adduction of the hand occurs according to the rule of the parallelogram of forces with simultaneous contraction:
- flexor carpi ulnaris
- extensor carpi ulnaris
Carpal
abduction The following muscles are involved in wrist abduction:
- flexor carpi radialis
- extensor carpi radialis longus
- extensor carpi radialis brevis
- abductor pollicis longus muscle
- extensor pollicis longus.
Joint capsules
Normal sliding of the tendons of the shoulder joint is ensured by the synovial bursae located in the surrounding tissues. They are cavities filled with intra-articular fluid. The number of bags, their structure and shape depends on the individual characteristics of each person:
- The most common is the subscapularis joint capsule. It is located in the area between the subclavian and deltoid regions or in the area of the neck of the scapula.
- Slightly higher, between the coracoid process and the tendon of the subscapularis muscle, a subcoracoid bursa is formed.
- The largest bag (its dimensions coincide with the palm of a person) is called subdeltoid. It is located on the outside of the shoulder joint, in the area of the deltoid muscle. Represents one large or a large number of small formations.
Joint capsule
The head of the human ball-and-socket joint maintains its correct position due to the ligament system of the shoulder articulation. This strong connective tissue fuses with the thin joint capsule. The thickness of its surface is non-uniform. The densest layer is on the outer surface of the shell. It includes the coracohumeral ligament.
Other areas of the articulation strengthen the less developed articular-humeral ligaments (formed by the upper, middle and lower bundles). Despite the fact that they play a less important role in the functioning of the joint, characteristic thickenings are present in the places where they are dislocated. The segments of the joint capsule located between the ligaments are thinner and weaker.
Periarticular tissues
The shoulder joint is surrounded by three main structures - the cartilage plate, the joint capsule and ligaments. All these tissues differ in their structure, origin and main functions. But thanks to their interaction, a person’s upper limbs are quite mobile. In addition, periarticular tissues perform a protective function, reducing the risk of possible damage.
The cartilage plate smoothes out the difference in size between the head of the humerus and the glenoid cavity. It softens minor shocks and impacts, but its safety margin may not be enough under severe physical impact.
What causes neck pain
Spasms in the muscles of the upper back and neck muscles can occur due to injury, physical strain, such as incorrect postures. Sleeping on an uncomfortable pillow can also cause shoulder and neck pain. Typically, this condition manifests itself as painful sensations and limited neck mobility. Typically, the pain goes away within six weeks. To speed up the process, you can do special exercises, and it is also necessary to eliminate the cause of the pain.
Provoking factors include:
- staying in the same body position for a long time;
- the habit of slouching, holding your back incorrectly while working and walking;
- excess weight;
- hypothermia;
- exacerbation of chronic diseases;
- injuries;
- spine pathologies;
- wearing narrow, uncomfortable shoes with high heels;
- uncomfortable body position during sleep.
Up to contents