Bone fractures occur frequently in humans. Depending on the severity of the fracture, bones may heal differently. It happens that the recovery process is long and sometimes painful, and the consequences of the injury make themselves felt for many years.
It is known that the vast majority of non-union fractures can be treated surgically. As for the reasons why fractures do not heal and have negative consequences, they include:
- addition of infection;
- impaired blood supply to bone tissue;
- improper patient management and treatment (for example, a splint was applied incorrectly or therapy was prescribed incorrectly, etc.).
All this can lead to different consequences of fractures that appear in people depending on the initial severity of the process, its further course and issues related to treatment and rehabilitation measures.
Main types of fractures and complications
There are several types of limb fractures, but in a broad sense, all fractures are divided into open and closed. Open fractures are especially dangerous, that is, cases where bone fragments penetrate the surface of the skin, tearing it. These types of fractures are also called compound fractures.
Fractures are easy to treat in most cases, but they can all be dangerous. The most common complications of fractures are associated with the fact that the pain syndrome provokes serious shock, which leads to inhibition of the body’s vital system. A fracture triggers neural and reflex response mechanisms that can affect the entire body and in particular the cardiovascular system. It is not uncommon for a person with a fracture to faint, which is why all trauma clinics have ammonia. Fainting can lead to a sharp drop in blood pressure.
It is also worth saying that the location of the damaged limb (especially with open fractures) can impede blood flow to the affected area, and can also cause compression of blood vessels or tissue ruptures. Compound fractures can also cause complications such as infection.
Effect of fractures on soft tissues and bones
Of course, any fracture (“mild” or “severe”) has a huge impact on the bones, which need regular blood flow. If the fracture is extensive, open and complex, this can be fraught with severe blood loss, leading to long-term malnutrition:
- bone tissue cells;
- bone marrow.
It is known that the formation of blood cells occurs in the bone marrow. We are talking about stem cells that are actively involved in the creation of red blood cells and platelets. Thanks to red blood cells, our body constantly delivers oxygen to organs and tissues, and platelets are involved in blood clotting when a person receives an injury or cut.
Many human internal organs are made of soft tissue. Often, when the bones of the skull are fractured, the brain is affected, and when the ribs are broken, the lungs and diaphragm are affected. If a bone is broken and severely damaged, it can threaten the integrity of an organ and often the life of the patient.
Free consultation on training issues
Our consultants are always ready to tell you about all the details!
Leather
With closed fractures, when the skin is not damaged, most often no marks remain on the skin. If the fracture is open, the skin and mucous membranes lose their integrity. The wound may later leave a scar on the skin.
Muscles
With both open and closed fractures, protrusions and bone fragments can damage the muscles surrounding the bone. This is often accompanied by severe pain and swelling. If the patient was prescribed the correct treatment, the swelling subsides after a week or a little more, and the muscles gradually return to normal.
When the patient is in a cast for a long time and the rehabilitation process is long, one can often observe the phenomenon of wasting of the muscles damaged by the fracture. The diseased limb may look smaller than the healthy one, the muscles are flaccid, and movement is difficult. In such cases, physiotherapy, therapeutic exercises, and supportive medications are indicated.
Joints and ligaments
Prolonged immobilization in severe forms of fractures leads to problems with the ligamentous and articular apparatus. Of course, he often suffers from a fracture as such (for example, a fracture may be accompanied by a rupture or stretching of the ligamentous-articular apparatus). Impaired mobility in such cases is typical. If excess connective tissue forms on the ligaments as they heal, a person may experience regular pain and even lameness.
Bones
In complex fractures with displacement of bone fragments and fragments, the phenomenon of crepitation (or crunching) is observed when the damaged parts of the bones rub against one another. Usually the process of fusion in such cases is long and it is far from certain that the bone will heal successfully, even with proper treatment.
Separately, it is worth mentioning the problems associated with fractures of tubular bones in childhood. It happens that after an injury, as a result of a serious violation of blood circulation and nutrition, the diseased bone does not grow along with healthy ones (if the fracture is close to the joint). We are talking about the so-called “growth plate” in children and adolescents. It is located at the end of all long bones. As soon as the skeleton finishes growing and forming, the growth plates are replaced with hard bone tissue. Until the period when this happens, the “growth plates” are the most vulnerable places in childhood and adolescent trauma. This means that during a fracture it is she who is damaged along with the bone joint (not tendons, as in adults).
Also, with open fractures, concomitant diseases and general weakness of the body, infection of bone tissue can join all problems. Most often, inflammation of the bone marrow or osteomyelitis occurs. Fungal and bacterial infections of bones should also be taken into account, since an open fracture is a wound surface that is vulnerable to the influence of infectious agents.
Classification of fractures
Fractures can be classified according to different parameters. In general, the word "fracture" refers to when a bone has broken, but bone can break in many different ways, so a fracture can be complete or partial.
Fractures can also be classified based on the reason they occur. Common cases of broken limbs have nothing to do with general health, such as when a person falls off a motorcycle and breaks a leg as a result. But there are cases when the fracture is associated with the patient's condition, for example, osteoporosis in the elderly. This disease (and many other diseases) makes bones weak and brittle, so a person can break a limb simply by carelessly stepping on a step. There are also special sports injuries when a fracture is the result of constant stress on the bone.
In simple fractures, the bone, although broken, is stable and in the correct, even position. But there are also unstable fractures, when fragments of the broken bone are displaced.
Help with an open fracture
An open fracture is a bone fracture in which bone fragments are connected to the external environment through the wound channel. Primary open fractures occur directly during injury due to injury to all soft tissues above the fracture site, secondary open fractures occur during transportation of the patient as a result of poor-quality immobilization or lack thereof, when a sharp bone fragment perforates the skin, as well as during treatment (for example, when secondary necrosis of the skin from the pressure of unrepaired fragments). Open fractures account for about 8-10% of all bone fractures.
The degree and extent of soft tissue damage play an important role in the clinical course of fracture healing and the possible occurrence of complications (shock, wound suppuration, osteomyelitis). Minor tissue damage proceeds favorably and is not accompanied by severe shock; after initial surgical treatment, the risk of wound suppuration is significantly reduced. The more crushed and nonviable tissue occurs, the greater the likelihood of severe wound infectious complications.
To take into account the severity of an open fracture, predict possible complications and the course of healing, several classifications have been proposed. The simplest classification for determining the severity of an open fracture of long bones should be considered the classification of A. V. Kaplan and A. N. Markova. In it, open fractures are grouped according to the type of wound into 3 groups : A (puncture), B (bruises), C (crushed). In addition, according to the size of the wound, each group is divided into 3 subgroups: 1 (up to 1.5 cm), II (2-9 cm), III (more than 9 cm). Separately, group IV is identified, which includes very severe open fractures.
In open fractures of groups I A, II A, III A, the damage to soft tissues is, as a rule, insignificant, and it occurs as a result of perforation of the skin by sharp bone fragments. In such cases, after carefully performed primary surgical treatment, primary wound healing and bone fusion occurs without complications.
Open fractures of group B are characterized by significant damage to soft tissues, hemorrhages and less favorable healing of particularly large wounds.
Group B fractures occur due to direct trauma due to compression, are accompanied by significant crushing of soft tissues and, regardless of the size of the wound and the quality of PSO, are difficult and cause more complications.
Particular open fractures (group IV) are severe due to significant crushing of soft tissue and bone, as well as great vessels and nerves. A large number of patients undergo amputation due to the non-viability of the damaged limb segment. However, amputation should not be rushed if there is no threat to the patient’s life. In addition, you should constantly monitor his general condition, diuresis, laboratory blood and urine values, so as not to miss the onset of the development of traumatic toxicosis (crash syndrome).
All open fractures are contaminated with microorganisms. Therefore, to prevent a purulent-inflammatory process, primary surgical treatment should be carried out in a short time - the first 4-6 hours after injury, that is, before the development of microflora in the wound. Primary surgical treatment is aimed at converting an open fracture into a closed one while preserving living tissue as much as possible. It covers:
1) reliable pain relief, which is carried out using general anesthesia;
2) treatment of the surgical field according to general rules;
3) mechanical cleaning of the wound from foreign bodies with tweezers, and then washing with hydrogen oxide and an antiseptic solution (furacilin - 1: 5000, ethacridine lactate - 1: 1000, etc.);
4) excision of non-viable soft tissues.
For open fractures of small bones, you can use a solution of novocaine (0.5-1%) for conduction anesthesia. Local application of novocaine solution does not provide the necessary anesthesia, since it is poured through the wound canal. Washing the wound with active suction of solutions using a vacuum apparatus allows you to minimize the degree of microbial contamination.
The problem for the surgeon remains determining the state of the damaged tissue (live, dead) and predicting its viability. Removal of non-viable tissues is carried out layer by layer. The skin is cut out sparingly with a scalpel, since due to damage and traumatic swelling of the tissue, however, there will not be enough of it to suture the wound without tension (transform an open fracture into a closed one). Therefore, only clearly crushed and pathologically altered skin is excised.
Damaged and blood-soaked fatty tissue, as a good environment for the development of microorganisms, is radically removed within the healthy tissue.
Pieces of damaged fascia are cut out, healthy fascia is dissected along the fibers far (5-7 cm) beyond the wound, and at the end of PSO it is not sutured. By cutting the fascia, decompression of the swollen muscles is achieved, improving their living conditions.
Muscle tissue, as a highly differentiated tissue, reacts quickly enough to injury. The crushed or pathologically changed (in color, reaction to irritation) section of the muscle is radically cut out. When cut with scissors, normal muscle bundles react by twitching the fibers.
Bone fragments must be perfectly set and firmly fixed. It is advisable to store free bone fragments, regardless of their size, provided that the wound heals by primary intention or if there are no conditions for the occurrence of osteomyelitis.
In doubtful cases, with significant damage to soft tissues, it is more advisable to remove them, deliberately shortening the segment in anticipation of further planned surgery - filling the defect, lengthening the segment (if necessary). In case of severe open fractures of long tubular bones, where there is significant discharge from the wound or tissue swelling, the optimal method of fixation of fragments is hardware (Ilizarov, Kalnberz, Hoffman, etc.). It ensures normalization of lymph and blood circulation, trophism, provides good access to the wound and the ability to monitor the state of the reparative process.
If the main vessels are damaged during open fractures, it is better to use technically simple intraosseous (intramedullary) osteosynthesis or hardware rod osteosynthesis to quickly restore blood flow. To fix fragments of small bones, Kirschner wires are used, which are inserted percutaneously outside the wound.
Before suturing, the wound is cleaned and hemostasis is monitored, it is injected with broad-spectrum antibiotics, and when possible, ultrasonic cavitation is used with solutions of antiseptics and antibiotics (5-second exposure per 1 cm2 of the wound surface). With open fractures of the tibia, difficulties are encountered in closing fragments of the tibia. In such cases, the fibers of the tibialis anterior muscle are moved from the outside and the extensor hallucis longus muscle from the inside of the bone.
Often, lateral loosening skin incisions are also made, followed by closing the defect after moving the flaps or using a free autodermal graft (primary skin grafting). In cases of severe tissue damage, it is advisable not to suture the wounds for 24 hours, to establish a flushing system, or to irrigate it with antiseptics and antibiotics through inflow and outflow.
Complications during the rehabilitation stage
During the rehabilitation stage after a limb fracture, a person may encounter a large number of complications. These complications do not happen to everyone, and they depend on the type of fracture, as well as the patient's level of care and self-care.
Many complications during the rehabilitation stage are associated with fractures that required surgical intervention. For example, during a surgical procedure, blood vessels or soft tissues may be injured, and after the operation, bleeding or suppuration of the wound may occur.
Complications such as improper healing of the fracture or the formation of a false joint, as well as skin necrosis, embolism, thromboembolism, etc. are possible.
Complications during the rehabilitation process are rare if treatment is carried out competently and the patient is well monitored. But the occurrence of complications also greatly depends on the person himself, so he must strictly follow the instructions of his doctors and observe the motor regimen prescribed to him.
First aid for fractures
Not only the health, but often the life of the injured person depends on the timely provision of first aid immediately after a fracture.
Immediately at the time of injury, or immediately after a fracture, complications may develop, so every person should know how to properly provide first aid for fractures.
A fracture is a disruption of the integrity of a bone due to trauma. Depending on whether or not there is damage to the skin directly above the fracture site, closed or open fractures are distinguished. When an injury develops, bone fragments may be in a physiological position (non-displaced fracture) or there may be a discrepancy between the resulting fragments (displaced fracture).
Traumatologists distinguish between absolute and relative signs of fractures. Absolute signs of a fracture reliably indicate that an injury has occurred, and upon examination the diagnosis does not cause difficulties. Such signs include an open wound above the fracture site, bleeding, the appearance of mobility in the part of the body where there should be solid bone, the detection of a characteristic crunch when trying to palpate the damaged limb, and the presence of bone fragments in the wound. Relative signs of a fracture indicate only that an injury has occurred and that there is a dysfunction of the limb.
First aid for fractures can be provided by witnesses to the incident (first aid) or provided by a specialist (medical aid). Even if first aid is provided correctly, the patient must be sent to a traumatologist, who will provide full medical care, accurately diagnose and prescribe appropriate treatment for the identified fracture.
After providing first aid, the emergency doctor will also take the patient with a fracture or suspected fracture to a specialized hospital.
How to provide first aid for a fracture?
The basic rule of providing assistance for a fracture is adherence to the principle “Do no harm.” If an injury occurs, you need to make sure that the victim is not in additional danger, and if possible, the patient should not be moved until the ambulance arrives. If there is still a danger to the victim, then he can only be moved on a rigid stretcher (this is very important if a spinal injury is suspected or a fracture of large bones - the pelvic bones, femur).
It is necessary to carefully examine the victim and try to determine which damage is most dangerous to the patient’s life. If there is bleeding, you need to try to stop it; to do this, you can raise the bleeding limb, apply a bandage that will compress the bleeding site, or compress the limb with a tourniquet. If there is slight bleeding, you can immediately apply a sterile bandage directly to the wound. Severe bleeding is stopped by applying a tourniquet, and for arterial bleeding the tourniquet should be applied above, and for venous bleeding below the wound site.
The maximum time that the tourniquet can be on the limb is no more than two hours, while every half hour you need to loosen the applied tourniquet for several minutes - this is done to prevent tissue necrosis due to restricted blood circulation.
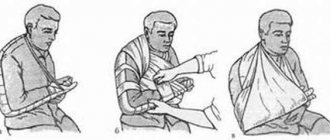
If the examination reveals reliable or probable signs of a fracture of the limbs, then first aid for a fracture will consist of applying an improvised splint, which will prevent further displacement of the fragments. When applying such a splint, it is necessary not only to fix the immediate site of the fracture, but also the two joints closest to the site of the fracture. You can make an improvised splint from scrap materials, and in the complete absence of such materials, you can bandage the injured leg to the healthy one, and the injured arm can be bandaged to the body.
After completing all these measures, you must definitely call an ambulance, whose specialists will be able to apply a more durable fixation splint and take the victim to the trauma department, where further treatment will be carried out
Author
Zelenkin Ilya Viktorovich
traumatologist-orthopedist
Doctor of the highest category
Experience 27 years
+7