To restore range of motion, strength, and mobility in the leg after a shin bone fracture, rehabilitation is often done through physical therapy.
The tibia contains two long bones that run parallel to each other. The tibia runs along the inside of the lower leg. The fibula runs along the outside of the lower leg. The ends of these two bones converge and participate in the formation of the knee and ankle joints.
The tibia is the only bone in the lower leg that supports the weight of the body. Tibial fractures are the most common injuries to the long bones of the human body. However, because the tibia and fibula are connected, fibular fractures can occur when the tibia is injured.
The lower leg also contains important nerves and blood vessels. The common peroneal nerve wraps around the upper end of the fibula and can be damaged by fibular fractures. Damage to large arteries in this area can also lead to significant blood loss.
Fractures of the shin bones
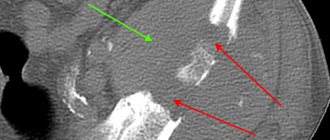
Fractures of the tibia or fibula require a period of immobilization to heal. In some cases, such as if the bone breaks into several pieces or the bones cannot be realigned by hand, surgery may be required. This procedure, known as open reduction (open reduction of bone fragments) and intramedullary osteosynthesis (intraosseous fixation), involves the application of plates reinforced with screws to maintain the correct position of the bone. Sometimes fractures are fixed externally with temporary pins or other fixation devices that are removed after the bone has healed.
Rehabilitation after fractures usually begins with training a special way of walking. In most cases, you will not be able to put weight on the injured leg for at least four weeks. After this, you will be allowed to touch the ground with your finger, then partial weight bearing is allowed at a certain percentage of your body weight, and then full weight bearing. Resuming normal walking after a tibia or fibula fracture may take two to four months, depending on the nature of the injury.
Application of massage procedures
Massage sessions are carried out at different stages of treatment. In combination with other therapeutic methods, they are especially effective because they:
- elimination of stagnation;
- elimination of remnants of muscle atrophy;
- increasing the elasticity of muscles and ligaments;
- improving the mobility of the foot joints.
The use of massage procedures is possible in the presence of plaster. Methods:
- massage the part of the leg that is without plaster;
- light and infrequent tapping on the plaster;
- light pressure on the area of the leg near the cast.
After removing the plaster, the procedures are mainly carried out by specialists, but you can learn the technique of self-massage. Stroking movements are performed with the fingertips on both sides of the ankle, across and along the limb. You need to move from the shin to the toes. Discomfort should not be allowed; massage should not cause pain.
Recovery exercises
Physical therapy for a fractured tibia and/or fibula can begin as early as a week after the injury. Rehabilitation exercises for a broken leg can begin while the leg is still in a cast. Exercises such as bending and straightening the leg at the hip and knee joints maintain normal function of these joints and help maintain some strength in the legs as the bone heals.
Straight leg raises
These lifts strengthen the muscles in the hip and knee areas.
Doing the exercise. Lying on your back, bend your uninjured leg at the knee. Straighten the injured leg completely and lift it up to the height of the bent knee of the uninjured leg. Slowly lower your leg. Repeat 10 times, performing up to 3 sets in a row.
Foot rotation
Active foot exercises can begin after the cast is removed. They develop the ankle joint and help reduce swelling. Exercises are performed 2-3 times a day.
Doing exercises.
- Sit on a chair or on the edge of a table. Perform circular movements of the foot clockwise, then counterclockwise. 10 times in each direction.
- Point your toes down toward the floor, then extend them up toward the ceiling 10 times.
- Draw the alphabet in the air with your big toe, moving your foot as far as possible in each direction without pain.
Passive stretching exercises
Passive range-of-motion exercises are first performed by a kinesiotherapist and can then become part of your home exercise routine.
Doing the exercise. Sit down, wrap a towel, a belt, or best of all, an elastic compression bandage around your foot and hold one end in each hand. With your leg straight out in front of you, gently pull the towel to point your toes toward your head. Stop when you feel a stretch in the back of your shin. Hold for 20 to 30 seconds; then relax.
Repeat three times. Do not stretch until it hurts, as this may cause further damage to the healing bone.
Strengthening leg muscles
In addition to the foot rotation exercises described above, another resistance exercise can be added to strengthen the muscles as part of physical therapy for a tibial fracture.
Doing the exercise. Sit down and straighten your leg. Wrap a rubber bandage around your foot. Hold the ends in your hand or tie it to a secure object, such as a table leg.
Perform resistance exercises in four directions: down-up, left-right. Repeat 10 times in each direction, performing up to 3 sets in a row. Since the exercise becomes easier over time, increase the resistance of the band by folding it in 2-3 layers.
Toe workout
Toe strengthening exercises can help improve walking after a tibia or fibula fracture.
Doing exercises.
- Sit on a chair with your feet on the floor. Place balls made of metal, marble, etc. on the floor next to your feet. Using your toes, grasp the ball, lift it, and place it in the cup. Repeat this step with each ball. The exercise is performed within a few minutes.
- Place a towel on the floor and squeeze it with your toes. Then raise your legs and hold the towel for 2-3 seconds. Relax. Repeat the exercise 10 times.
All the exercises described here can be performed if you have suffered a fracture of the lower leg bones. Each of these exercises can be performed at home. However, this does not mean that you should not seek the help of specialists in exercise therapy and/or kinesiotherapy.
Each injury has its own specific characteristics, so only a specialist can tell you what you need to do to speed up the process of restoring lost functions.
Restoration of walking in patients with tibial fractures after osteosynthesis
In the process of restorative treatment of patients with shin fractures after surgery during the period of consolidation of the fractures, we used the physical rehabilitation method developed by us, which included the following means: exercises on the arthromote, exercises for the muscles of the lower leg and foot, and exercise machines.
After rehabilitation measures, we examined the biomechanical features of gait. The study included 25 patients. The patients were divided into two subgroups with right-sided and left-sided damage. We studied the temporal characteristics of the step, such as the step cycle time, the support period, which includes the period of single and double support. The study was carried out on the MBN-Biomechanics software and hardware complex, before and one month after rehabilitation.
When analyzing the time characteristics of a step, initially in healthy individuals, in the support period, the period of single support is most represented, which demonstrates their good ability to lean on one limb for quite a long time, while transferring the other; the step cycle time is, on average, 1.2 seconds. , the support period is 60% of the step cycle time, the transfer period is 40%.
In patients, a violation of the temporal characteristics of the step is observed mainly on the affected side. These patients have an increase in the time of the step cycle, with an increase in the proportion of double-support periods (up to 40%) when the patient relies on both limbs. In this case, there is a reduction in the period of single support on the affected side (up to 25%). On the healthy side, there is an adjustment decrease in the proportion of single-support periods and an increase in the proportion of double-support periods: right-sided lesion (ratio of left and right sides before treatment). Left side: TsSh-1, 27+0, 20, PO-68, 19+4, 97, DO-36, 00+6, 68, OO-32, 54+2, 42. Right side: TsSh-1, 28+0, 19, PO-67, 41+2, 58, DO-37, 27+6, 05, OO-29, 69+4, 06; left-sided lesion (ratio of left and right side before treatment). Left side: TsSh-1, 19+0, 11, PO-65, 96+2, 96, DO-34, 99+6, 96, OO-31, 03. Right side: TsSh-1, 19+0, 11, PO-68, 17+3, 93, DO-35, 04+6, 29, OO-33, 59+3, 13.
After a month of using the rehabilitation technique we developed, patients observed a reduction in step cycle time on both sides, primarily on the affected side. The same applies to the support period, which decreases due to a decrease in the proportion of the two-support period, both the tuning period on the healthy side and the true one on the affected side. The proportion of the period of single support on the affected side increases: right-sided lesion (the ratio of the left and right side after treatment). Left side: TsSh-1, 17+0, 10, PO-66, 01+3, 10, DO-33, 69+6, 87, OO-33, 74+2, 80. Right side: TsSh-1, 17+0, 10, PO-66, 44+4, 40, DO-33, 19+6, 56, OO-33, 21+4, 87; left-sided lesion (ratio of left and right side after treatment). Left side: TsSh-1, 18+0, 07, PO-64, 64+0, 45, DO-29, 91+1, 61, OO-34, 17+1, 59. Right side: TsSh-1, 17+0, 06, PO-64, 43+0, 31, DO-29, 13+1, 19, OO-35, 17+1, 62. The values of the time characteristics are close to the normative ones obtained in healthy individuals.
Thus , as a result of using this rehabilitation method, the temporal parameters of the step improve, which is expressed, first of all, by a reduction in the time of double-support periods and an increase in the time of the single-support period. This leads to an increase in walking speed and increased dynamic stability.
Additional recommendations
To form the natural arch of the foot after an injury and prevent dislocations and fractures, you need to wear orthopedic shoes. It fixes the leg as comfortably as possible and improves blood circulation.
Important. Orthopedic shoes prevent calluses, swelling, fatigue, and help treat bunions and diabetic feet.
Frame insoles are important for rehabilitation after a foot fracture, allowing you to properly distribute the load and reduce pain. Long-term walking significantly reduces discomfort and increases stability.
In combination with exercise therapy and massage, you can use folk remedies , for example, baths :
- 3 tablespoons of chamomile or chamomile are poured into 500 ml of hot water and infused for 1 hour. The liquid is filtered and poured into a warm basin where you need to place your feet. The duration of the procedure is 20 minutes.
- Half a glass of sea salt is dissolved in a bowl of warm water. The feet are kept in the container for at least 15 minutes.
A responsible attitude towards your health and regular performance of complex exercise therapy contribute to a quick recovery and restoration of all functions of the injured foot.
Late rehabilitation
It is carried out after the cast is removed, when the patient is already allowed moderate loads on the limb. During this period, a callus has already formed, but it has not completely strengthened, so measures are aimed at maintaining further regeneration and returning functions to muscles that have been without movement for several months.
Exercise therapy
Physical therapy is the basis for complete rehabilitation after a hip fracture. Gymnastics can be general, which is carried out to improve the health of the whole body, or special. The latest type of exercise therapy includes:
- flexion and extension in the knee and hip joints - in the first days after immobilization is carried out as carefully as possible;
- lifting the limb and bringing the knee to the body;
- learning to walk with a walker, crutches and a cane;
- classes on special simulators.
It is best to visit a medical rehabilitation center for recovery, where the program will be supervised by a doctor. The doctor will be able to select the optimal loads that will help restore lost functions and strengthen bone tissue.
Diet
Nutrition during the recovery period should be enhanced and contain large amounts of protein, calcium and magnesium. You also need to avoid fatty foods, because during immobilization almost no calories are consumed and problems with excess weight may appear.
The diet should include:
- boiled lean meat and fish;
- boiled eggs;
- low-fat milk, cheese, cottage cheese;
- jelly, jellied meat, jelly;
- legumes in limited quantities;
- greens, vegetables and fruits.
It is better to eat often, but in limited portions. Overeating is unacceptable; it is better to leave the table with a slight feeling of hunger. It is also undesirable to overeat before bed.
Physiotherapy and tekar therapy sessions
Physiotherapy procedures are prescribed from the 10th day and are carried out for several months for complete healing. Such rehabilitation after a fracture of the femur is recommended for all patients; at the initial stages, the doctor may prescribe medicinal electrophoresis, then supplement the sessions with shock wave therapy or warming up.
Tecar therapy shows good results:
- the therapeutic effect is achieved due to the penetration of radio waves into the tissue and heating of the tissue;
- energy is transmitted without radiation, thereby achieving maximum effect;
- after several sessions, blood flow improves in the affected area and tissue regeneration is stimulated.
Due to such sessions, it is possible to reduce the rehabilitation period after a hip fracture. Patients show noticeable improvement; this innovative method perfectly complements the rehabilitation program.