Many people are afraid of anesthesia. And many are hesitant to undergo knee arthroscopy, being sure that it is performed under anesthesia. But if you understand the medical terminology, it turns out that this is not so. Intrigued? Well, then let's figure it out.
Looking in any dictionary of medical terms, you will read that anesthesia is a deliberate inhibition of the central nervous system (CNS), the purpose of which is to “disconnect” the patient from the feeling and awareness of pain impulses. That is, for example, the effect on the patient’s brain with special drugs. In this case, an artificial coma occurs, muscles relax, some reflexes turn off and pain sensitivity disappears.
Anesthesia involves completely putting a person to sleep in order to turn off the central nervous system. However, not every patient is put to sleep during arthroscopy. Anesthesia is used only in special cases. And most arthroscopic interventions are performed under local, spinal and conduction anesthesia. These types of pain relief do not require “switching off consciousness”, so they frighten patients less.
Why is anesthesia needed for knee arthroscopy?
Anesthesia is a general concept that refers to the process of suppressing pain sensitivity with the help of drugs. It is necessary to relieve a person from pain, stress and discomfort during surgery.
Anesthesiologists distinguish several types of anesthesia:
- General (anesthesia) - effects on the central nervous system, the brain and consciousness of a person. Anesthetics are administered intravenously or by inhalation, through a laryngeal tube or mask.
- Spinal and epidural - blockade of the nerve roots that innervate the lower extremities. Painkillers are injected into the spine, at the level of the spinal cord.
- Conductor (regional) - involves blocking the nerve trunks and nerve plexuses, which are located above the operation site. Arthroscopy usually involves blocking the femoral and sciatic nerves.
- Local (infiltration) - blockade of sensory receptors of peripheral nerves. It involves the infiltration of periarticular tissues with anesthetics, as well as their introduction into the joint cavity.
Different types of anesthesia differ in strength, degree of analgesic and muscle relaxant effect. When choosing an anesthesia method, a number of factors are taken into account: the patient’s age, his state of health, the presence of concomitant diseases, the degree of trauma and pain of arthroscopic intervention, etc.
Spinal and epidural anesthesia: advantages
Let us dwell in more detail on certain types of regional anesthesia - popular and in demand today.
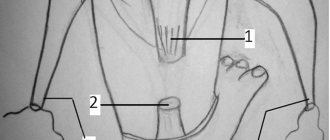
You will come across some medical terms that you cannot do without. To begin with, we want to show you some drawings reflecting the structure of the human spine. Note the two sectors: the subarachnoid space and the epidural space, and their location in relation to the spinal cord:
Figure 1 and 2. The spinal cord and its membranes shown in a cross-section of the spine
The spinal canal has three connective tissue membranes that protect the spinal cord: the dura mater, the arachnoid mater, and the pia mater. The spinal cord and its roots are covered by a well-vascularized pia mater, and the subarachnoid space is delimited by two adjacent membranes - the arachnoid and dura mater.
Figure 3. The spinal cord and its membranes in another plane.
Figures 4 and 5. The spinal cord membranes in a three-dimensional image. In Figure 4, the epidural space extends down to the dura mater (gray cylinder), and the spinal cord lies within this cylinder.
General rules of anesthesiology
Adequate pain relief is an important condition for restoring limb function after surgery. Therefore, certain requirements are imposed on anesthesia during arthroscopic operations.
The main ones:
- sufficient intraoperative pain relief;
- adequate pain relief in the early postoperative period;
- minimal impact on the muscle tone of the operated limb.
It is extremely important that the patient maintains muscle strength and muscle tone in the lower extremity after surgery. This is necessary for early loading of the leg (full or dosed). If muscle strength is maintained, the person begins to walk soon after surgery, which allows him to be discharged from the hospital faster.
How does meniscus repair work?
Arthroscopic interventions are performed without opening the joint cavity, which significantly reduces postoperative rehabilitation. With arthroscopy, tissue is damaged much less than with other operations. And the scars remain almost invisible due to the small size of the incisions.
The first few days after the operation, the person is in the hospital, and the attending physician carefully monitors his condition. At this time, the patient takes prescribed medications and performs special exercises under the supervision of medical staff. His post-operative wound is carefully cared for. After discharge from the hospital, the patient continues to exercise and care for the wound, but on his own. At the same time, he follows all the recommendations given by the doctor.
The duration of rehabilitation is usually 8-12 weeks. After this period, the patient is allowed to return to their usual lifestyle and even play sports. He can return to office work even earlier - in 2-3 weeks. And to physical labor - after 4-6 weeks.
Early healing stage (first 7-10 days)
After arthroscopy, the patient is allowed to stand up immediately after the anesthesia wears off. At first, doctors recommend using crutches or a cane. At the early healing stage, the person is allowed to walk carefully within the apartment, avoiding the appearance of pain in the knee.
During this period it is also recommended:
- Apply an ice pack wrapped in a towel to your knee 4-5 times a day. It should be kept for at least 15-20 minutes. This will help relieve knee pain and speed up recovery.
- Wear compression garments or bandage the limb with an elastic bandage from the foot to the middle third of the thigh. This precaution is necessary to prevent thromboembolic complications in the postoperative period.
- Give an elevated position to the shin and knee joint. In bed, the operated limb should lie on a pillow, above the level of the heart.
- Perform special exercises at least 2-3 times a day. Each workout should last 20-30 minutes. Daily exercises are needed to train muscles and normal restoration of limb function.
If swelling and redness of the skin appears in the area of the knee joint, it is necessary to reduce the load on the limb or temporarily stop performing exercises. And if swelling persists for more than two or three days, you should see your doctor.
Late healing stage (days 10-14)
At this stage of rehabilitation, weight-bearing exercise on a stationary bike, cycling and resistance exercises are added to physical therapy. In this case, the patient still has to use crutches when walking.
Third stage (starting from the third week)
During this time, a person can perform various exercises, but sports are still prohibited. If there are no contraindications, one month after surgery the patient is allowed to walk in an orthosis with full weight bearing on the operated leg. During the second month, a person performs functional exercises that help restore muscle strength, train endurance and completely restore the range of motion of the limb.
Knee brace.
At the end of the second month, the patient can return to a free motor mode, including sports.
Features of different types of anesthesia
For intraoperative pain relief, various methods of general, regional and local anesthesia, as well as their combinations, are used. Each of them has a number of disadvantages and advantages.
Local
From a technical point of view, local anesthesia is the simplest. Even a traumatologist can perform local administration of anesthetics without the help of an anesthesiologist. However, such anesthesia does not always provide a sufficiently strong analgesic effect. And its quality largely depends on the practical skills of the traumatologist.
Conductor
It is one of the best options for pain relief during arthroscopic interventions on the knee joint. It is technically more complex than local, and therefore requires great skill of the anesthesiologist. The doctor must have a good knowledge of the structure of the peripheral nervous system, master the technique of blocking nerves at different levels, and be able to use special instruments to perform a femoral / sciatic nerve block.
Conduction anesthesia provides long-term pain relief during movement of the lower limb and thereby improves the course of the early postoperative period. However, due to technical difficulties, it is still less common than spinal.
Spinal
Guarantees adequate postoperative pain relief and early restoration of muscle tone. However, a number of complications can occur, including spinal cord or root injuries, radiculopathy, cauda equina syndrome, seizures, etc. The high incidence of side effects (back pain, headaches, hypotension) often reduces patient satisfaction with the quality of such pain relief.
Anesthesia
It is rarely used during arthroscopy, usually in one-day hospitals. Modern intravenous and/or inhalational anesthetics can be used for anesthesia. During surgery, the patient often breathes independently through a laryngeal mask. For special indications, he may undergo artificial pulmonary ventilation (ALV).
Anesthesia has its advantages:
- safety;
- good handling;
- minimal number of side effects;
- no effect on the muscle tone of the limb in the postoperative period;
- possibility of rapid discharge from hospital.
At the same time, anesthesia does not always provide adequate postoperative pain relief. Therefore, in the early stages after arthroscopy, the patient may be additionally administered anesthetics.
Indications
Athletes most often resort to knee arthroscopy after meniscus injuries and ligament ruptures.
The most common indications for arthroscopy are:
- To accurately diagnose pathology, take a biopsy;
- The need for joint rehabilitation;
- Meniscus tears of varying degrees;
- Damage to the cruciate ligaments.
- Arthritis.
Arthroscopy allows you to simultaneously clarify the diagnosis and perform treatment of the knee joint within the framework of the operation. This is an important advantage of this method of surgical intervention.
Choosing a pain relief method
Today, most arthroscopic interventions are performed under spinal anesthesia. For short-term operations, a 2% lidocaine solution is injected into the patient's subarachnoid space. For arthroscopy lasting more than 1.5 hours, a 0.5% solution of isobaric or hyperbaric spinal marcaine is used. Note that spinal anesthesia can cause hemodynamic complications if the patient is hypovolemic. Therefore, in gerontological patients, an epidural is often used instead.
In recent years, diagnostic and therapeutic arthroscopy has increasingly been performed under general anesthesia. It is less expensive, less likely to cause side effects, and produces greater satisfaction among patients and trauma surgeons.
In emotionally labile patients, intravenous anesthesia with mechanical ventilation or spontaneous breathing through a laryngeal mask is often used.
Local anesthesia is used only for low-pain arthroscopic interventions, for example, when removing foreign bodies from the joint cavity. “Classical” anesthesia with intubation and muscle relaxation is also used extremely rarely, only if there are special indications.
Historical reference.
The first diagnostic arthroscopy has already celebrated its centenary. It was performed by Kenji Takagi in Tokyo 100 years ago (1919). Earlier in 1912 At the Congress of Surgeons in Germany, the famous Danish doctor Severin Nordenfort reported on his research in this area. Also making a major contribution was the Swiss politician and physician Eugen Bircher, who shared his own experience of arthroscopic diagnosis of knee injuries in his works published in the 1920s. Dr. Masaka Watanabe developed the first arthroscope for mass production. Over time, through the work of many scientists and surgeons, this device was significantly improved, and now surgeons use its improved modern version in their practice.
In Leningrad in 1986, for the first time, arthroscopy on a fresh knee injury was successfully performed by Professor, Doctor of Medical Sciences Igor Aleksandrovich Kuznetsov, now vice-president of the Russian Arthroscopic Society, current member of ESSKA and chief physician of the Sports Clinic. For more than 30 years, Igor Aleksandrovich has performed over 10,000 arthroscopic operations.
Contraindications
The greatest number of contraindications exist for general anesthesia. When administered systemically, anesthetic drugs can negatively affect internal organs. Therefore, anesthesia is contraindicated for arrhythmias, heart defects, bronchial asthma, bleeding disorders, renal, hepatic and cardiovascular failure.
Contraindications to spinal and epidural anesthesia may include infection at the injection site and allergy to anesthetics. These types of pain relief will not be used even if there are no contraindications. This is possible if the patient himself refuses them.
Possible complications after surgery
Arthroscopy is one of the safest knee surgeries. However, even after it, complications, both early and delayed, can occur.
These include:
- Complications caused by anesthesia. They may occur as a result of individual intolerance to drugs, the patient’s serious condition, or errors by the anesthesiologist.
- Hemarthrosis is a massive hemorrhage into the joint cavity. It occurs extremely rarely and practically never occurs after arthroscopy.
- Thromboembolic complications. With adequate prevention and wearing compression garments, they are rare. In exceptional cases, patients experience thrombosis of the veins of the lower extremity or pulmonary embolism (TEPA).
- Joint fluid leakage. With excessively rapid resumption of physical activity, synovial fluid can leak from the joint cavity and enter the periarticular tissue. To avoid this, early loading of the limb should be avoided.
- Nerve damage. Damage to nerve branches during surgery can cause paresthesia in the knee joint. In this case, the patient may feel a “crawling sensation” after arthroscopy.
- Sprained medial collateral ligament. Occurs rarely if the surgeon performs enhanced manipulations, increasing the distance between the femur and tibia for better access to the meniscus.
- Deforming osteoarthritis. Develops late after arthroscopy, as a result of progressive damage to articular cartilage. It is difficult to treat and over time can lead to impaired function and mobility of the knee.
Infectious complication.
The risk of complications largely depends on the experience and skill of the operating surgeon, as well as the level of the institution where the operation takes place. If you want to protect yourself, try to be treated in the best clinics, and choose the best specialist as your attending physician.