Shoulder subluxation is a partial or incomplete dislocation that usually occurs due to changes in the mechanical integrity of the joint. In subluxation, the head of the humerus comes out of the scapula as a result of weakness in the rotator cuff muscles or a blow to the shoulder area. Subluxation can be of three types: anterior (directed anteriorly), posterior (directed posteriorly) and inferior (directed downward).
Clinically Relevant Anatomy
Of all the joints, the shoulder (or glenohumeral) joint has the greatest range of motion. Since it is also the most commonly dislocated joint, it perfectly demonstrates the principle that stability must be sacrificed to achieve mobility.
The shoulder joint is formed by three bone structures: the humerus, the scapula and the clavicle. These bones make up a total of 3 synovial joints: the glenohumeral joint, the sternoclavicular joint, and the acromioclavicular joint. In addition, the subacromial and scapulothoracic joints are distinguished.
The size of the glenoid cavity is increased by the fibrous cartilaginous labrum, which continues beyond the bony edge of the glenoid cavity of the scapula. The bones of the shoulder girdle provide some stability at the top of the joint because the acromion and coracoid process extend laterally above the head of the humerus. However, most of the stability is provided by the surrounding skeletal muscles through their associated tendons and ligaments.
Friends, this and other questions will be discussed in detail at the seminar Diagnosis and treatment of problems of the glenohumeral complex.
The main ligaments that help stabilize the shoulder joint are the glenohumeral, coracohumeral, coracoacromial, and acromiohumeral ligaments. The acromioclavicular ligament strengthens the acromioclavicular joint capsule and supports the superior portion of the glenohumeral joint. The largest ligament is the glenohumeral ligament, which is usually damaged or strained when the shoulder joint is subluxated.
The muscles that move the humerus stabilize the shoulder more than all the ligaments and capsular fibers combined. Muscles originating in the trunk, shoulder girdle, and humerus cover the anterior, superior, and posterior surfaces of the capsule. The supraspinatus, infraspinatus, teres minor, and subscapularis tendons strengthen the joint capsule and limit range of motion. These muscles, known as the rotator cuff, are the primary mechanism for supporting the shoulder joint and limiting range of motion.
Basic treatment methods
What to do if the shoulder joint pops out, the traumatologist decides after studying the results of instrumental studies. Conservative treatment methods are most often used. Pharmacological drugs are used to eliminate painful sensations. Traumatologists prescribe NSAIDs in tablets and ointments (Voltaren, Nurofen, Fastum), and external agents with a warming effect (Capsicam, Viprosal, Apizartron). Patients are advised to take a long-term course of chondroprotectors (Teraflex, Artra, Chondroxide), which stimulate the strengthening of the ligamentous-tendon apparatus.
Chondroprotectors.
Therapy for chronic instability involves changing the nature of physical activity. Movements that place stress on the shoulder joint should be minimized. These include:
- throws with a wide swing;
- bench press;
- intense rotation of the joint.
If painful or other uncomfortable sensations arise during movement, they should be done as rarely as possible. Changing your physical activity helps prevent further tissue damage.
Physiotherapeutic procedures are also used in the treatment of the disease - UHF therapy, acupuncture, magnetic therapy, laser therapy, applications with ozokerite and paraffin. Patients are advised to perform special exercises daily to build muscle corset, strengthen ligaments and tendons. And only if conservative treatment is ineffective, surgery is performed.
| Surgery to correct chronic shoulder instability | Surgical technique |
| Open surgery | It is performed in cases of severe damage to articular elements and the development of complications. A wide dissection of the connective tissue structures is performed to provide access to the surgical field. Torn ligaments are repaired to improve the fixation of the shoulder |
| Arthroscopy | The soft tissue is repaired through microscopic incisions using arthroscopic instruments. In most cases, minimally invasive surgery is performed on an outpatient basis. The patient is immediately discharged for further rehabilitation at home. |
Animation of a surgical operation:
A person suffering from chronic instability often moves the joint back into place on their own. Traumatologists strongly do not recommend doing this. The pathology is characterized by a recurrent course, so another attempt to straighten the shoulder may result in the development of severe complications. Self-medication leads to damage to large vessels, bleeding, capsule rupture, compression or injury to nerve trunks.
Clinical picture
The main problem with shoulder subluxation is instability of the glenohumeral joint. The anatomy of this joint allows for a large range of motion, which is accompanied by a loss of stability. A study conducted by Basmajian determined that the supraspinatus muscle and also the posterior fibers of the deltoid muscle play a key role in preventing humeral subluxation. Chaco and Wolf also confirmed in their study that the supraspinatus muscle is very important in preventing inferior subluxation of the humerus. Shoulder subluxation occurs during abduction and external rotation.
Other studies indicate that the most important ligamentous structure for maintaining proper alignment of the humerus and also for preventing shoulder subluxation is the inferior glenohumeral ligament. This ligament is most important in external rotation and abduction during the throwing movement.
Shoulder subluxation can lead to soft tissue damage because traction can occur due to gravitational forces and a weak shoulder provides poor protection. This is usually quite painful and may be accompanied by partial numbness in the shoulder, arm and hand.
Characteristic features of the pathology
A condition where the shoulder frequently pops out of the socket is called chronic instability due to decreased function of the joint. There is a weakening of connective tissue structures, usually the joint capsule and the ligamentous-tendon apparatus. This leads to excessive range of motion of the bones that form the shoulder joint. The structure of the joint resembles a ball joint. The rosette of the joint is formed by the articular fossa of the scapula, and the head of the humerus bone serves as the spherical support. The elements of the articulation are lined with strong connective tissue - the joint capsule, and are fastened together by ligaments. Holding the shoulder in place while increasing its stability is the rotator cuff, a group of muscles.
A person performing movements with his hands (for example, throwing a heavy object) can injure his shoulder. This situation also occurs with a direct blow, falling forward with emphasis on an outstretched arm. The joint capsule, ligaments, and muscle tissue are affected by a force that significantly exceeds their strength limits. Frequent microtrauma of connective tissue structures causes a violation of their integrity. They lose strength and cease to fully stabilize the joint.
An excessive increase in the range of motion is a prerequisite for constant, habitual dislocations and subluxations. The head of the bone slips out of the articular fossa, shifting relative to the other elements of the articulation.
Report from a conference of traumatologists on the problem under consideration:
Differential diagnosis
Damage to the acromioclavicular joint
AC joint injuries are common and often occur after falls from bicycles, during contact sports, and as a result of automobile accidents. The acromioclavicular joint is located at the top of the shoulder where the acromion and collarbone are located, forming the joint. Several ligaments surround this joint, and depending on the severity of the injury, a person may tear one or all of the ligaments. Damaged ligaments lead to stretching of the acromioclavicular joint or disruption of its integrity.
Recovery after a dislocated shoulder.
Rehabilitation measures take place in several stages. At the initial stage, in the first week after the injury, the patient is given rest with limitation of any actions in the shoulder joint, cold compresses are used, and the doctor prescribes electrophoresis. It is recommended to lightly warm up the hands and wrists (to prevent future atrophy of the arm muscles). At the next stages, exercises for developing the arm are gradually strengthened (a set of exercises is selected individually for each patient), and various physiotherapeutic procedures are prescribed. By strictly following all the recommendations of your doctor, continuing to do gymnastics to develop the joint and observing basic safety requirements, you can avoid serious consequences (for example, repeated dislocation, etc.)
Diagnostics
Symptoms
Patients with shoulder subluxation usually have:
- Pain in the shoulder area.
- Decreased range of motion.
- A palpable gap between the acromion and the head of the humerus (conventionally, this can be measured by the width of the fingers).
Functional tests
- Subluxation test is positive = resistance is encountered when the patient brings the arm into a throwing position, in the direction of internal rotation.
- Pain in the anterior capsule indicates anterior shoulder injury.
- Pressure on the back of the joint (during a resistance test) can cause it to move anteriorly, which can cause anterior subluxation and severe pain. This can be performed at various degrees of shoulder abduction, with or without shoulder support.
X-ray examination is considered the most accurate way to assess the extent of subluxation.
Shoulder instability
V.A. Mitskevich
Institute of Rheumatology, Russian Academy of Medical Sciences, Moscow
Joint stability There are two groups of stabilizers in the shoulder joint: 1) passive: the head of the humerus and the articular process of the scapula, the coracoid process, the clavicle, the capsular-ligamentous apparatus; 2) active: muscles of the rotator cuff and periarticular muscles. The capsular-ligamentous apparatus performs mechanical and neuroinformational functions. The joint capsule provides its mechanical strength. The ligaments of the joint limit movement in the position of extreme flexion, extension and abduction. Flexion and extension are limited by the coracohumeral ligament. Abduction and adduction are limited by the glenohumeral ligaments.
The action of active and passive stabilizers depends on the position of the hand. In positions corresponding to the maximum range of motion, the main stabilizers are ligaments, which, when stretched, keep the shoulder from moving. When the ligaments are stretched, their elasticity decreases. As the range of motion in a joint increases, the tension in the ligaments increases and their resistance increases, resulting in limited movement. During abduction, the most important stabilizer is the inferior glenohumeral ligamentous complex [1]. In it, the upper bundle of the inferior glenohumeral ligament has the greatest strength and thickness. It prevents the head of the humerus from moving anteriorly during shoulder abduction and its external rotation [2]. During external rotation of the shoulder, the upper, middle and lower glenohumeral ligaments, as well as the subscapularis muscle, play a stabilizing role [1].
In the middle position of the shoulder, the ligaments do not perform a stabilizing function, since the degree of their tension is insignificant. The main active stabilizers of the shoulder are the long head of the biceps tendon and the rotator cuff muscles. As a result of the synergistic work of the stabilizer muscles, the head of the humerus is tightly pressed against the glenoid cavity of the scapula with the head centered in the cavity. The coordinated work of the muscle cuff protects the ligaments from overstretching. The pressure of the head is facilitated by the articular labrum, located along the edge of the glenoid cavity. It creates a vacuum effect, “sucking” the head of the shoulder to the shoulder blade, thereby enhancing the stabilization of the joint. The joint is stabilized along the anterior surface by the tendinous part of the subscapularis muscle, and along the posterior surface of the joint by the infraspinatus and pectoralis minor muscles [3]. Displacement of the shoulder during abduction and rotation is prevented by tension in the deltoid muscle, which, according to T. Kido et al. [4], stabilizes the joint along its anterior surface.
Displacement of the shoulder in the horizontal plane is prevented by the short rotators of the shoulder, the infraspinatus, teres minor, subscapularis and supraspinatus muscles. Vertical displacement of the shoulder is limited by the long head of the biceps tendon and the supraspinatus muscle, which have been called “active ligaments” [5].
Variants of shoulder dysplasia that predispose to the development of instability
| Dysplasia | Comments |
| Additional bone of the humeral process of the scapula, which connects it to the clavicle through synchondrosis or diarthrosis [4] | |
| Change in the shape of the acromion process of the scapula | There are three variants of the shape of the process: flat, curved and hooked. When the rotator cuff is damaged, a hook-shaped process occurs in 73% of cases [6] |
| Increasing the retroversion angle of the humerus | Normally, this angle is 300. Reducing the angle to 200 contributes to instability of the joint (E. Codman, cited in [5]). The rotation of the humerus is caused by the action of the muscles attached to it; it can change during the growth and development of the body. Therefore, the stability of the joint can change during growth [27] |
| Underdevelopment of one of the bony elements of the joint, leading to incongruence of the articular surfaces | There are 3 main options for the relationship between the size and shape of the head of the humerus and the articular process of the scapula: the head of the humerus is smaller than the articular surface of the scapula; the head completely coincides in size with the articular surface of the scapula; the head is larger than the articular surface of the scapula. In the first and third anatomical options, joint stability decreases, while in the second option it is normal [28]. In addition to qualitative changes in the joint, quantitative methods are used to assess dysplasia. The following changes in the bone elements of the shoulder joint are described, which occur in the decompensated form of joint instability [13]: 1) an increase in the angle of the articular process of the scapula more than 150° (normal 140°); 2) a decrease in the length of the articular surface of the scapula to 30 mm (normal 40–42 mm); 3) reducing the size of the humeral head to 25–26 mm (norm 30 mm) |
| Features of the structure of the anterosuperior part of the articular labrum | There are 3 main variants of the structure of the anterosuperior part of the articular labrum [29]: the hole under the lip; attachment of the glenohumeral ligament along the edges of the hole; absence of cartilage in the anterosuperior part of the labrum. These changes predispose to an increase in the amplitude of internal rotation of the shoulder, which contributes to damage to the glenohumeral ligaments and the anterosuperior part of the glenoid labrum [29] |
| Coracoacromial ligament dysplasia | There are 3 main types of coracoacromial ligament: square, wide and U-shaped. Wide and U-shaped ligament types predispose to the development of impingement syndrome at a relatively young age before the onset of degenerative changes in the joint [30] |
| Dysplasia of the middle glenohumeral ligament | Occurs in general GM in the form of underdevelopment of the ligament, which contributes to the forward displacement of the humerus [9] |
| Increasing the volume of the joint capsule | It is observed in both anterior and multiplanar instability against the background of ligament hyperelasticity [9] |
In addition to the mechanical function, the capsular-ligamentous apparatus provides a neuroinformational function due to the presence of proprioceptors. In the shoulder joint capsule there is a disproportion between different types of mechanoreceptors. The Ruffini corpuscles, which function as limiters of the extreme position of the segments, turn out to be smaller than the Pacinian corpuscles, which have a low threshold of excitability, quickly react and adapt to changes in the position of the elements of the joint. Mechanoreceptors provide information about the position of joint elements, which is necessary for contraction of the rotator cuff muscles. When movements in the joint occur, proprioceptors are irritated, which causes contraction of the corresponding muscles that stabilize the joint.
Manifestations of instability Regardless of the etiology, severity, plane of displacement, compensatory reaction, instability of the shoulder joint has a number of characteristic manifestations. A patient with instability of the shoulder joint complains of a feeling of discomfort and displacement in a certain position of the shoulder, as well as clicking and pain in the joint. With instability, subluxation in the joint may occur, which is immediate. In this case, the head of the humerus slides anteriorly relative to the articular process of the scapula, and then independently returns to its original place [6]. Subluxation is characterized by the absence of clear symptoms and blurred clinical picture. With instability, shoulder displacement can occur with inadequately small physical impact. When the joint is unstable, characteristic behavior of the patient is noted. It consists of increased caution and stiffness when moving. A patient with an unstable shoulder joint carefully considers his plastic surgery. He avoids sudden shoulder abduction, large range of motion, vigorous contact with the hands, sweeping handshakes, door pushing, etc. When looking at a patient with instability of the shoulder joint, the general tension of the shoulder girdle and the pressing of the shoulder to the chest are noticeable.
During passive movements of the shoulder, you should pay attention to the patient’s sensations. Instability of the shoulder joint is characterized by the patient's fear of a certain position of the arm, in which subluxation may occur. Anxiety is expressed in the form of muscle tension in the shoulder girdle and resistance to movement. A positive “fear test” indicates the possibility of dislocation or subluxation [7]. With active movements in the shoulder joint, instability manifests itself in the form of uncontrolled displacement of the shoulder, which is manifested by unpleasant sensations. The patient may also complain of a lack of sensation of shoulder movement and discomfort in a certain position of the shoulder [8].
In practice, a number of tests are used to detect instability of the shoulder joint. During passive movements, the shoulder is considered unstable if traction on the arm along the axis can easily reveal subluxation in the anterior or posterior direction [9].
The vertical stability test is performed with the patient in a sitting position with the scapula fixed. Traction is carried out by the hand along the axis. A downward displacement of the humeral head is determined if a depression appears in the subacromial region of more than 1–2 cm.
The horizontal stability test is performed with the patient in the supine position. The arm is placed in a neutral position, the humeral head is centered due to traction along the axis. The head of the humerus is shifted forward and backward. The degree of head displacement is assessed on a three-point scale [6]. The test for the possibility of subluxation is carried out with the patient lying on his back. The arm will abduct 90° in a position of maximum external rotation. During rotation, the patient complains of a feeling of displacement in the joint and pain. The possibility of displacement of the humeral head forward and backward indicates instability of the joint.
Classification of instability The process leading to instability of the shoulder joint is multicomponent, which creates difficulties in diagnosis and treatment. There are several classifications of shoulder instability.
Classification of instability depending on the plane of displacement 1. Horizontal 2. Vertical 3. Mixed (horizontal + vertical)
Classification of multiplanar instability [10] 1. Instability with hyperelastic ligaments due to congenital connective tissue deficiency (Marfan, Ellers–Danlos syndrome) 2. Multiplanar asymptomatic anterior and inferior instability 3. Multiplanar posterior and inferior instability 4. Multiplanar anterior and posterior instability
Classification of instability of the glenohumeral joint [9] A - static instability A1 - static superior dislocation A2 - static anterosuperior subluxation A3 - static posterior subluxation A4 - static inferior subluxation B - dynamic instability B1 - chronic subluxation B2 - uniplanar instability without hyperelasticity B3 - uniplanar instability with hyperelasticity B3.1 - anterior instability with hyperelasticity B4 - multiplanar instability without hyperelasticity B5 - multiplanar instability with hyperelasticity B6 - single and multiplanar instability with independent shoulder reduction C - spontaneous dislocation
A clinical indicator of instability is the degree of displacement (translation) of the humeral head in the joint. The degree of displacement depends on many factors, in particular physical activity and loads on the joint. According to J. Tibone et al. [8], transmission in the joint appears to be increased in young people who are actively involved in swimming. According to C. Geber et al. [9], the amount of translation in a joint in itself is not an indicator of joint instability, since both healthy people and patients with instability have a large scatter of translation values.
In clinical practice, several classifications of the degree of shoulder translation (displacement of the humeral head in the scapula in response to direct external influence) are also used. Degree of shoulder translation according to Hawkins [11] Degree 0 – no displacement. Grade 1 – mild. The humeral head moves 1 cm forward within the glenoid cavity. Level 2 – average. The head moves from 1 to 2 cm, but does not extend beyond the edge of the glenoid cavity. Level 3 – severe. The head moves beyond the edge of the glenoid cavity by more than 2 cm and returns to its place after the force ceases. In the same person, in the absence of pain, the difference in translation in the left and right shoulder joints can exceed 11 mm. According to J. Tibone [8], the difference in the magnitude of translation in the left and right joints exceeds 3 mm in 84% of healthy people. Degree of shoulder translation according to Lintner [12] Degree 0 – no displacement. Degree 1 – the head does not move beyond the edge of the glenoid cavity. Degree 2 - the head moves beyond the edge of the glenoid cavity, but after the cessation of the external force it returns to its original place. Degree 3 – the head remains in the displaced position after the cessation of the external force. In a healthy person, the difference in the degree of shoulder translation in the left and right joints can be one degree.
Instability of the shoulder joint is a long-term pathological process that leads to changes in the entire musculoskeletal system. In this regard, a number of clinical forms of instability are identified. 1. Compensated form, in which the anatomy and function of the joint are close to normal. 2. Subcompensated form. The patient complains of pain and a clicking sensation in the joint. Mild muscle atrophy, anterior instability, limited external rotation of the shoulder, and decreased strength are detected. 3. Decompensated form. The patient complains of clicking, crunching and friction in the joint. Atrophy of more than 2 cm, anterior instability, decreased strength, and arm sagging are determined [13].
Traumatic dislocation Traumatic dislocation of the shoulder develops when falling on an outstretched arm. In this position, the humerus puts excess pressure on the anterosuperior rotator cuff. This area is subject to stretching or tearing. Based on experimental data, it was found that cuff rupture occurs at an abduction angle of up to 66°, when the pressure of the humeral head on the acromion process reaches 21.5 kg [14]. Traumatic shoulder dislocation accounts for 60% of all joint dislocations [15]. The type of dislocation is determined depending on the displacement of the humeral head relative to the articular surface of the scapula.
Classification of shoulder dislocations [15] 1. Anterior dislocations (account for 75% of all shoulder dislocations): a) subcoracoid b) intracoracoid c) subcondylar 2. Inferior dislocation, subarticular dislocation 3. Posterior dislocations: a) subacromial b) infraspinatus
Frequent injury to the shoulder joint is facilitated by such features of its structure as a narrow zone of congruence between the head of the humerus and the articular process of the scapula; predominance of the size of the head over the size of the articular process of the scapula; the predominance of the size of the joint capsule over the size of the bone elements of the joint; unequal strength of the joint capsule in different parts.
A dislocation in the shoulder joint is accompanied by a number of pathological changes that can be detected using X-ray and ultrasound examinations (ultrasound), as well as magnetic resonance imaging (MRI). 1. Displacement of the humeral head is diagnosed on a standard radiograph in the anteroposterior projection. 2. Damage to the rotator cuff. Ultrasound reveals thinning of the cuff. A complete rupture of the cuff in “fresh” cases can be masked by fluid in the joint. 3. Rupture of the synovial sheath of the long head of the biceps muscle. Ultrasound reveals an unclear structure of the tendon with the inclusion of areas of increased echo density. When the tendon is completely ruptured, its defect is determined. 4. Damage to the cartilaginous lip in combination with rupture of the joint capsule. Ultrasound reveals a flattening in the lip area with unclear boundaries. 5. Damage to the tendon of the subscapularis muscle. Ultrasound reveals an area of reduced echogenicity at the site of attachment of the tendon of this muscle to the humerus. In the presence of a hematoma, a limited hypoechoic structure is determined [5, 7]. 6. Fracture of the greater tubercle of the humerus. It is determined by radiographs and ultrasound [16]. 7. Impression fracture of the humeral head. Ultrasound reveals a depressed defect in the head of the humerus. 8. Bankart injury – a violation of the integrity of the anterioinferior portion of the joint capsule at the location of the inferior glenohumeral ligament (not determined by ultrasound) [16, 17].
The “gold standard” in the study of the shoulder joint is the MRI method [18]. Using MRI, you can identify the condition of structures that are damaged during traumatic dislocation. Particular attention is paid to the integrity of the coracohumeral and superior glenohumeral ligaments, the upper lip [19], the thickness of the rotator cuff, the position of the tendon and the insertion site of the long head of the biceps muscle, the condition of the coracoid process and subacromial bursa, and fluid accumulation [18]. In case of traumatic dislocation, shortening, rupture or complete absence of image of the joint ligaments is determined. A rotator cuff tendon tear is characterized by a high intensity lesion (T1 and T2) and a change in signal intensity around the tendon due to swelling. Acute and subacute hemarthrosis is determined by the appearance of contents in the lower parts of the joint, subacromial and subdeltoid bursae, characterized by a medium-intensity signal in the T1 mode and a high-intensity signal in the T2 mode. Chronic hemarthrosis is diagnosed if there are areas of heterogeneous intensity in the intra-articular fluid. The signal from the central part of such a region has high intensity in the T1 and T2 modes and is surrounded by a low-intensity border [18, 20].
Post-traumatic instability Post-traumatic instability of the shoulder joint develops after a traumatic shoulder dislocation. It occurs 3 times more often in men than in women [21]. Post-traumatic instability can be either single-planar or multi-planar. Uniplanar instability is more common, accounting for 60% of all cases of shoulder instability [9]. Multiplanar instability is characterized by a lack of shoulder stability in all positions. It is characterized by instability in the anterior and inferior directions. Such instability develops after repeated dislocations and subluxations [9].
After a dislocation, as a result of a complex violation of the anatomy and function of the shoulder joint, a pathological condition is formed, which is characterized by a lack of stability of the shoulder joint. Instability may progress over time.
The development of post-traumatic instability can occur as a result of iatrogenic errors made in the treatment of traumatic dislocation. These include rough reposition of the dislocation, undiagnosed fracture-dislocation, reduced rehabilitation time and early intensive rehabilitation. But traumatic dislocation does not necessarily lead to the development of joint instability. Factors that act after repair of a dislocation and contribute to the development of post-traumatic instability include: 1) a decrease in the mechanical strength of the joint capsule and rotator cuff as a result of stretching or tearing; 2) disruption of the flow of proprioceptive information from mechanoreceptors of ligaments in the central nervous system, feedback deficiency [22]; 3) impaired healing of the capsule and periarticular tissues, scar formation, weakening of the capsule, facilitating its stretching; 4) progressive weakening of the joint stabilizing muscles [23]. The development pattern of instability is as follows. The primary disorder is damage to the capsular-ligamentous apparatus of the joint due to dislocation or subluxation. Dislocation entails mechanical instability and proprioceptive deficits. Mechanical instability leads to impaired movement of the glenohumeral joint, resulting in the capsule being unable to withstand the pressure of the humeral head. Proprioception deficits lead to imbalances in the rotator cuff and long head of the biceps muscles, which worsens glenohumeral joint dysfunction. Impaired proprioception, which leads to decreased muscle tone and muscle activity, develops in parallel with impaired mechanical strength of the joint capsule and rotator cuff. Impaired healing of the capsule with the formation of scars leads to its weakening and facilitates the displacement of bone segments in the joint. Instability in the joint predisposes it to mild traumatization and contributes to repeated injuries. Repeated dislocations and subluxations become chronic. A vicious circle is formed that leads to joint degeneration.
The phenomena of post-traumatic instability can be identified using the MRI method. With post-traumatic instability, degenerative changes in the ligaments are determined (uneven contours, thinning and shortening of the coracoacromial and coracoclavicular ligaments), as well as degeneration of the articular labrum. According to MRI data, there are 3 stages of degenerative changes in the labrum [20]: Stage 1 – a pinpoint area of increased intensity; Stage 2 – a high-intensity linear area communicating with the articular surface of the scapula; Stage 3 – fragmentation and thickening of the labrum.
In case of post-traumatic instability of the shoulder joint, a number of pathological changes can be detected using ultrasound, and the sensitivity of this method reaches 100% [24]. Damage to the labrum is detected in 70% of cases. A rupture of the acromial clavicular joint is determined if the joint space is increased by more than 5 mm. It is possible to identify transverse and longitudinal ruptures of the biceps tendon. With ultrasonography, it is possible to detect a partial tear of the rotator cuff in the form of a defect at the location of the muscle tendons.
Chronic instability leads to frequent repeated dislocations and subluxations in the shoulder joint, which is complicated by its degeneration, the development of glenohumeral periarthritis, deforming arthrosis and impingement syndrome (impact syndrome), which cause pain in the joint [19]. Impingement syndrome is visualized using ultrasound in the form of entrapment of the supraspinatus tendon. An old rotator cuff tear is diagnosed if the size of the tissue defect exceeds 3 mm [24].
Dysplastic instability Dysplastic instability develops due to dysplastic changes in the bone and ligamentous structures of the shoulder joint [25]. The most common cause of dysplastic instability is hyperelasticity of the joint ligaments with joint hypermobility (JH) [26]. The trigger for the development of this type of instability is often a joint injury. The incidence of bilateral dysplastic instability does not depend on gender. Instability of the shoulder joint can develop in the presence of normal ligaments in other joints. In GM joints, the incidence of lesions of the shoulder joints ranges from 4.2 to 6.7%. Instability of the shoulder joint and spontaneous dislocation in childhood and adolescence are not directly related to GM [21].
Signs of bone and soft tissue dysplasia, as well as abnormalities of the shoulder joint with habitual shoulder dislocation occur in 27.7% of cases [3]. According to J. Tibone et al. [8], in patients with habitual shoulder dislocation, in 55% of cases the following signs of dysplasia of bone and non-bone formations are observed: hypoplasia of the articular ends; abnormalities of the attachment of the capsule and ligaments of the joint (the most common cause); anomalies in the structure of the articular labrum. The main types of shoulder dysplasia that predispose to the development of instability are shown in the table.
Instability of the shoulder joint can develop in several planes [9, 31]. The number of planes in which the humeral head is displaced does not depend on the condition of the ligaments. With both normal and hyperelastic ligaments, joint instability can be either single-planar or multi-planar. Uniplanar instability with hyperelastic ligaments is observed in 30% of cases [9]. Instability occurs after a traumatic shoulder dislocation.
More often it occurs during external rotation or when the shoulder is abducted or raised anteriorly. Anterior instability with hyperelasticity is associated with glenohumeral ligament dysplasia. With repeated dislocations in the joint, the capsule is stretched in one direction, and dislocation of the humerus is observed only in one plane [9]. Uniplanar instability is defined by ultrasound as translation of the shoulder in the anteroposterior direction and in the craniocaudal direction within the range of 15–12 mm [31].
With hyperelastic ligaments, multiplanar instability develops less frequently than single-planar instability. Unlike single-plane instability, multi-planar instability is a pathological condition. Multiplanar instability is detected starting in childhood and adolescence. It manifests itself as a bilateral painless dislocation. C. Geber et al. [9] called such a dislocation “controllable.” The authors believed that if a teenager controls the position of the shoulder in the joint, the dislocation does not require immobilization or surgical treatment, since it is not complicated by secondary degenerative changes in the joint. Multiplanar instability, according to G.Brown [21], corresponds to the clinical diagnosis “syndrome of multiplanar ligament hyperelasticity with instability.” With multiplanar instability, an increase in the size of the joint capsule is detected, which is caused by primary hyperelasticity and secondary traumatic changes [9]. Expansion of the joint capsule is detected by arthroscopy [32]. Multiplanar instability is characterized by impaired proprioception, as well as changes in the scapulohumeral rhythm. There are different data in the literature regarding the incidence of multiplanar instability in men and women. According to G.Brown [21], multiplanar instability in men and women occurs with almost the same frequency, and according to C.Geber et al. [9], multiplanar instability accounts for no more than 5% of all cases of instability of the shoulder joint and is more common in women who engage in water sports. The main complaint of patients is the lack of control over the position of the shoulder in the joint. Dislocations and subluxations occur from minor injuries. Arthroscopy reveals an increase in the size of the joint capsule. G.Brown [21] believed that the problem of multiplanar instability is relevant for people actively involved in physical education and sports under the age of 35, after which the number of patients decreases significantly.
With dysplastic instability, both the entire capsule and its individual sections or ligaments can be hyperelastic. With dysplasia, the fixing ability of the capsule is lost and the threshold of resistance to normal physical activity is reduced. This leads to the fact that an injury of inadequate magnitude can lead to dislocation or subluxation of the joint. In a patient with dysplastic instability, normal movements such as carrying a load in the hand, shaking hands, or holding a handrail may be excessive and cause displacement and pain in the joint. Dysplastic instability can be compensated by muscle work. Frequent subluxations lead to progression of ligament sprains and muscle atrophy. When compensatory capabilities are depleted, dysplasia contributes to the progression of instability [15].
Hyperelasticity of the ligaments affects muscle-joint sensation. Stability is based on the coordinated work of the muscles surrounding the joint and ensuring a stable position of the humeral head. Impaired proprioception leads to incoordination of movements in the joint, as a result of which the stabilizing function of the muscles is disrupted. This results in loss of muscle control over the joint. Mismatch of muscle work leads to the fact that under the action of the dominant muscles, displacement of the humeral head can occur, up to dislocation or subluxation [17]. Impairment of proprioception occurs as degenerative-dystrophic changes in the joint develop [18]. Degeneration leads to the development of impingement syndrome, which itself causes pain in the joint and impairs its stability.
Individuals with dysplastic instability do not show characteristic signs of pathology upon examination. The contours of the shoulder joint are not changed. Upon palpation under the acromial clavicular joint, the round head of the humerus is determined. Passive movements are possible in all directions. Movements are painless. Active movements may be limited during abduction. The restriction may be temporary. During abduction, a click or dull jolt is felt deep in the joint. The patient independently limits movements. During the swinging movements of the arm in the joint when walking, there is a feeling of imbalance in the movement of the humeral head in the joint, which is inconsistent. G.Brown [21] identified disturbances in the scapulohumeral rhythm when walking in such patients. With anteroinferior instability, dyskinesia is observed, with posteroinferior instability, an increase in the degree of scapular retraction is determined, and with inferior instability, lowering of the scapula is determined.
Treatment To treat instability of the shoulder joint, the following conservative methods are used: • A course of non-steroidal anti-inflammatory drugs • Brachial plexus block • Intra-articular injection of steroids • A complex of physical therapy, which includes passive movements of the arm using the healthy arm, exercises to strengthen correct posture, exercises to strengthen the rotator cuff muscles shoulder cuffs, movements with resistance, exercises to strengthen the scapular group of muscles and the muscles of the shoulder girdle.
Conclusion The shoulder joint is a complex system that allows arm movement in three planes. The stability of the joint is ensured by the cooperative action of active and passive stabilizers. The stability of the joint during movements within the middle part of the amplitude is provided by the muscles, and during movements of the maximum amplitude - by the ligaments. The degree of displacement of the shoulder in the joint is subject to large individual and interindividual fluctuations. In the same person, the degree of displacement of joint elements on the left and right may be different. There are two main forms of joint instability: post-traumatic and dysplastic. Post-traumatic instability develops after a joint is dislocated. Dysplastic instability occurs against the background of developmental disorders of the bone and soft tissue components of the shoulder joint. However, the provoking factor in the occurrence of dysplastic instability is most often also trauma. Instability of the shoulder joint of both traumatic and dysplastic etiology is a multicomponent pathological process. The complexities of the problem of diagnosing and treating instability of the shoulder joint are reflected in the classification of pathology. Instability can be single-plane or multi-plane. Instability is based on disturbances in the mechanical properties of the joint capsule, as a result of which the position of the shoulder relative to the scapula changes. Multiplanar instability is characterized by impaired proprioception, which leads to muscle imbalances that exacerbate joint instability. Instability is detected using clinical, radiological and arthroscopic methods, as well as ultrasound and MRI methods.
The term “joint instability” replaces the commonly used diagnosis of “habitual dislocation.” The term “dislocation” means displacement of the humeral head beyond the articular surface. In conditions of post-traumatic instability and joint dysplasia, this concept loses its definition. Instability is a permanent anatomical and functional disorder. The essence of the pathology is that when the joint capsule is stretched, voluntary and involuntary movements are disrupted, predisposing to dislocation. The concept of “instability” is relatively broader. It guides the doctor not only to immediate reposition of the dislocation, but to long-term targeted treatment of a multicomponent disease.
References 1. Abboud J, Soslovsky J. Clin Orthop 2002; 400: 48. 2. Ticker J, Bigliany L, Soslowsky L et al. J Shoulder Elbow Surg 1996; 5 (4): 269–79. 3. Matison Yu.A. Medical biomechanics. Riga, 1986; 2: 354–7. 4. Dyachenko V.A. X-ray osteology. M.: Medgiz, 1954. 4. Kido T, Itoi E, Neale P. Am J Sports Med 2003; 31(3):399–403. 5. Cherkes-Zade D.I., Berglezov M.A., Azizov M.Zh. et al. Treatment of habitual shoulder dislocation. Batumi, 1991. 6. Arkhipov S.V. dis. ...Dr. med. Sci. M., 1998. 7. Kapustinsky A.I., Prudnikov O.E., Prudnikov E.E. Morphology and surgery. Novosibirsk, 2000; issue 2, p. 102–3. 8. Tibone J, Lee Th, Csintalan R et al. Clin Orthop 2002; 400:93–7. 9. Geber C, Nyffeler R. Clin Orthop 2002; 400: 65. 10. Pagnani M, Warren R. J Shoulder Elbow Surg 1994; 3: 173–7. 11. Hawkins R, Bokor D. Clinical evaluation of shoulder problem, 1990. 12. Lintner S. Am J Sports Med 1996; 24: 716–21. 13. Povelikhin A.K., Kotelnikov G.P., Kozupitsa G.S. Diagnosis of joint instability in patients with habitual shoulder dislocation (Tutorial). Samara, 1996. 14. Averkiev D.V. Features of the biomechanics of the shoulder joint in case of damage to the rotator cuff. Organization and provision of outpatient care in the armed forces. SPb., 1997: p. 8–10. 15. Krasnov A.F., Akhmedzyanov R.B. Shoulder dislocations. M.: Medicine. 1982. 16. Eskin N.A. dis. ...Dr. med. Sci. M., 2001. 17. McMahon PJ, Lee T. Clin Orthop 2002; 403(Suppl.): 18–25. 18. Cohen R, Williams G. Clin Orthop 1998; 351: 95. 19. Hsu H, Luo Z, Stone J et al. Acta Orthop Scand 2003; 74(1):89–94. 20. Bryukhanov A.V., Vasilyev A.Yu. Magnetic resonance imaging in the diagnosis of joint diseases. Barnaul, 2001. 21. Brown G, Jee Lee Tan, Kirkley A. Clin Orthop 2000; 372: 110. 22. Blasier R, Guldberg R, Rothman E. J Shoulder Elbow Surg 1992; 1: 140–50. 23. Soslowsky L, An C, DeBano C et al. Clin Orthop 1996; 330:40–4. 24. Saltykova V.T. Author's abstract. dis. ...cand. honey. Sci. M., 2003. 25. O'Brien S. The shoulder. 1990. 26. Beighton P, Grahame R, Bird H. Hypermobility of joints. 1989. 27. Tyazhelov A.A., Vasilevsky N.M. Orthopedics, traumatology, prosthetics, 1993; 1:18–23. 28. Saha A. Recurrent dislocations of the shoulder, 1981. 29. Rao A, Kim T, Chronopoulos E et al. J Bone Joint Surg 2003; 85-A(4):653–9. 30. Kopus C, Baris S, Yildirim M et al. J Pediatr Orthop B 2002; 11 (4): 350–4. 31. Lee T, McMahon. Clin Orthop 2002; 403:26–31. 31. Shapovalov V.M., Tikhilov R.M., Trachuk A.P. and others. Vestn. surgery named after Grekova, 2001; 1600(2):53–7. 32. Hempfling H. Arthroscopy. Diagnosis and therapy.1992.
Source: https://www.consilium-medicum.com
Rating scales
Oxford Shoulder Instability Test (OISS)
The OISS is a 12-item questionnaire with five correct Likert responses for each question and has a range from 0 to 48 (with a score of 48 indicating better shoulder function). The OISS was developed and validated to assess shoulder instability and has also been tested to assess sensation in patients with shoulder instability.
Western Ontario Shoulder Instability Index (WOSI)
The WOSI is a 21-item questionnaire with a 100 mm horizontal visual analogue scale below each patient response question and ranges from 0 to 2100 as a percentage, with 100% representing the best possible shoulder-related quality of life. The WOSI is a carefully developed and evaluated instrument for patients with shoulder instability that has been demonstrated to have excellent sensitivity for posterior instability.
Treatment of habitual dislocation
Patients with habitual shoulder dislocations should undergo surgical treatment, since conservative methods in this case are completely ineffective.
Habitual dislocation differs in that stabilization of the shoulder joint can be done openly by making an incision on the anterior surface of the shoulder, as well as arthroscopically, without making incisions, that is, through punctures. A special optical device called an arthroscope . It allows you to examine the joint to identify the presence of damage to the ligamentous apparatus of the joint and determine the specific cause of instability. Through another puncture, special instruments are introduced into the joint cavity, which make it possible to attach the previously torn labrum. Fixation of the articular labrum is carried out using special absorbable clamps - anchors.
Survey
First, the researcher should ask the patient about the medical history. He can then perform an examination, comparing the affected shoulder with the unaffected side. To do this, you can use the following tests.
- Load and displacement test
In this test, the therapist stabilizes the scapula and moves the humeral head posteriorly and anteriorly. This test can determine whether the humeral head will subluxate.
- Push-pull test
The patient's arm is in a position of 90 degrees of abduction and 30 degrees of forward flexion. The examiner grasps the midsection of the patient's shoulder and applies posterior pressure. This test is used to evaluate posterior shoulder instability.
- Protzman test
This test is similar to the load and displacement test, but the examiner's second hand is placed in the axilla to feel the movement of the humeral head as close to the glenoid cavity of the scapula as possible.
Physical therapy
In patients with hemiplegia
Sling/support
Traditionally, support devices in the form of slings or orthoses have been used to manage patients with shoulder subluxation after stroke. The goal is to support the arm by preventing/minimizing downward displacement of the humerus and reducing stretching of the joint capsule. A 2009 Cochrane review concluded that there is insufficient evidence to conclude whether assistive devices are beneficial.
About shoulder subluxation with hemiplegia, see here.
Electrical stimulation
Also, one Cochrane review found that functional electrical stimulation increased pain-free passive external rotation of the humerus and reduced the degree of shoulder subluxation, but did not find a significant effect on upper limb motor recovery.
First aid
Timely first aid will help avoid the formation of inflammatory edema, which significantly increases pain. The victim needs to be laid down or sat down, given a non-steroidal anti-inflammatory drug (NSAID) tablet - Nise, Ketorol, Ibuprofen. What to do next if the shoulder joint is knocked out:
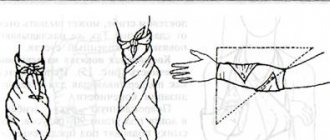
- immobilize (immobilize) the shoulder. To do this, use any available means: elastic or gauze bandage, scarf, scarf;
- provide the joint with functional rest. You cannot make movements that provoke an even greater displacement of the shoulder structures - flexion or extension of the elbow, rotation of the hand;
- apply a cold compress. A plastic bag filled with ice cubes and wrapped in thick cloth will help eliminate pain and prevent the formation of edema and hematoma. It is applied to the joint for 10-15 minutes. The procedure is repeated after an hour.
Now the victim needs to be taken to the emergency room or an ambulance is called.