Causes of the disease
Blount's disease is the second most common after rickets among musculoskeletal pathologies in children.
Most medical guidelines classify this pathology as rare, but some orthopedists believe that mild forms of the disease are often not diagnosed or are considered as rickets-like deformities. Girls are affected more often than boys. The causes of Blount's disease have not been fully established. It is assumed that impaired development of epiphyseal cartilage is caused by local osteochondropathy or chondrodysplasia. The disease can be combined with other congenital developmental anomalies, and familial inheritance cannot be ruled out. Predisposing factors are considered to be excess body weight, early walking and endocrine imbalance. The trigger point is an overload of the unprepared musculoskeletal system in combination with a certain anatomical variant of the structure of the lower limb.
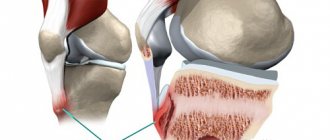
Varus alignment of the tibia causes overload of the internal or external condyle of the tibia, as a result of which the epiphyseal zone expands, bevels, and moves inward and downward. Due to the uneven distribution of the load, not only bones, but also soft tissues are exposed to increased pressure, which leads to the occurrence of neurodystrophic disorders. As a result, the function of the limb is further impaired, and pathological changes in the pineal gland are aggravated. The ossification process is disrupted, cartilage cells either turn into bone tissue more slowly than normal, or transform into inferior bone, unable to withstand normal loads. The condyle grows at an angle, a beak-like protrusion appears in the area of the metaphysis, and a curvature is formed below. In the lower parts, the lower leg remains almost straight, the foot rotates medially.
Symptoms and course of the disease
Most often, the first signs of the disease are observed in a child of 1-2 years old, when he begins to walk. Parents may notice a slight curvature of their baby's legs, as well as incorrect varus position of the feet (when the emphasis is not on the entire foot, but on its outer side). Shortened lower limbs and lameness when walking may also indicate the onset of Blount's disease.
A clumsy “duck” gait is characteristic, caused both by the direct curvature of the legs and by loose ligaments of the knee joint. With bilateral damage, after some time a disproportion in the length of the upper and lower limbs becomes noticeable - the legs are relatively shortened due to curvature, so the arms look unnaturally long. In some cases, the fingers can reach the knee joints.
Patients have height below the age norm due to the relative shortening of the lower extremities. An external examination reveals a bayonet-shaped curvature of the legs in the upper part in combination with straight diaphyses. A coracoid protrusion is found in the upper parts of the tibia. The head of the fibula will survive. The shins are internally rotated, the degree of rotation can vary widely (from 20 to 85 degrees). Flat feet, atrophy and decreased tone of the lower leg muscles are also detected.
Classification of Blount's disease
There are two forms of Blount disease:
- Infantile. The first signs of the disease appear at the age of 2-3 years. Characteristic is symmetrical damage to both legs.
- Teenage. Symptoms of the disease appear after the age of 6 years. Usually one lower leg is affected.
Taking into account the type of deformation, they distinguish:
- Varus curvature of the legs (O-shaped legs). Occurs in most cases.
- Valgus curvature of the legs (X-shaped legs). Rarely detected.
Taking into account the degree of deformation, four variants of Blount disease are distinguished:
- Potential. The angle of curvature does not exceed 15 degrees, marginal sclerosis is detected (usually on the inside, less often on the outside) in the upper part of the tibia.
- Moderately expressed. The angle of curvature is 15-30 degrees, destruction and fragmentation of the proximal epiphysis of the tibia are determined.
- Progressive. Extensive fragmentation and expansion of the proximal epiphysis in the middle part is revealed.
- Rapidly progressing. The growth zone in the medial section closes, and a bone bridge appears between the metaphysis and epiphysis.
What can Blount's disease be confused with?
- in a child under 2 years of age – with physiological norms;
- with rickets and rickets-like diseases, phosphate diabetes;
- in rare cases - with achondroplasia, hypochondroplasia, TAR syndrome.
When evaluating a child with suspected infantile Blount disease, teamwork is essential for success. The minimum that the orthopedist should not neglect is a consultation with an experienced pediatrician (who will prescribe a list of laboratory tests for your child). You may also need: examination by a nephrologist, endocrinologist, geneticist.
Etiology of the disease
The exact cause of the development of the pathological process has not been established. Doctors believe that disruption of the formation of the epiphyseal part of the bone is caused by osteochondropathy or chondrodysplasia. The syndrome is often combined with other pathological abnormalities. Erlacher Blount disease has a hereditary predisposition. If one of the relatives suffers from the disease, then the child is at high risk of developing leg deformities. The onset of the disease can be provoked if you start teaching a child at an early age, when the skeletal system has not yet become stronger. Often, curvature of the legs is observed in babies with increased body weight.
Why is it important to make a correct diagnosis?
Treatment for Blount disease is, in most cases, surgical. Most children under 2 years of age have a physiological varus (O-shaped) curvature of the legs. An extreme version of this physiological curvature may be mistaken for a bilateral form of Blount's disease. This child will undergo surgery. At the same time, further growth of the child, if surgical intervention is not performed, leads to independent correction of this curvature, and surgical treatment can lead to the formation of valgus (X-shaped) deformity. If we confuse Blount's disease with rickets and rickets-like diseases, then surgical intervention may be ineffective and lead to recurrence of the deformity, because we did not compensate for the missing element (vitamin D, calcium, phosphorus, etc.). Moreover, timely therapy selected by a pediatrician may be sufficient for self-correction of the deformity as the child grows.
Diagnosis of pathology
An important task in making a correct diagnosis is to determine the cause of the curvature, since the curvature of the legs is a secondary pathology. It is necessary to differentiate Blount's disease from rickets. To do this, the child is prescribed a blood test, which determines calcium, phosphorus, and alkaline phosphatase. If the indicators are normal, then the diagnosis is made based on the results of an objective examination and X-ray examination. The doctor asks parents about the time of the first symptoms, clinical manifestations, the age of the child, and hereditary predisposition. The following symptoms are visually determined:
- visible shortening of the limbs;
- characteristic curvature in the knee joint outward or inward;
- reduction of muscle tension;
- development of flat feet.
Diagnosis of pathology
X-rays show certain changes:
- A beak-shaped deformity of the tibia is formed. The pathology is localized in the upper part of the metaphysis or the area between it and the epiphysis.
- The articular surface of the bone is curved inward and beveled. The height of the epiphysis from the inside is three times lower than the normal size, and marginal fragmentation is observed.
- The growth zone expands from the inside, bone plates have unclear boundaries. Adolescents are diagnosed with a prematurely closed bone growth zone.
- Due to rotation, the projections of the fibula and tibia overlap each other in the image.
Leg deformity on x-ray
The pathological process affects not only the bones, but also the tendons and muscle layer. To determine the degree of damage to muscle and ligament fibers, CT or MRI are used. Using tomography, tissues are examined layer by layer, the condition of bones and cartilage is revealed.
Should Blount's disease be treated?
In this case, there is no doubt - it is necessary. The problem is not just an aesthetic issue. If Blount's disease is not treated, then in 100% of cases the patient is doomed to arthrosis of the knee joint with early manifestations, namely, pain symptoms. We can say this with confidence, because... We have repeatedly encountered patients with the infantile form of Blount's disease who did not receive treatment at a young age, but presented at the age of 12-15 years. Most of these children already had pain symptoms that limited their daily activities.
Prevention
To prevent the development of the disease in a child, provided that the pathology is not caused by a birth defect, parents need to follow several rules:
- ensure the intake of vitamin D into the baby’s body, especially in winter;
- teach a child to crawl;
- control weight;
- prevent early walking (up to 10 months);
- Visit an orthopedist periodically.
Following these recommendations will help you notice the first manifestations of the disease.
Regarding the tactics of treating Blount's disease, we fundamentally use the following algorithm in our practice.
- Child under 3 years old. Massage, unloading of the lower extremities. A number of orthopedists prefer plaster corrective bandages or their orthotic equivalent. We do not use these methods, because... From our point of view, it is important to exclude axial load on the affected limb(s), and casts do not allow this.
- For a child under 4 years old, there is confidence in the diagnosis, there are no radiological signs of synostosis (fusion) of the growth plate - hemiepiphysiodesis with figure-of-eight plates (controlled growth). Child over 4 years old, no synostosis, corrective osteotomy, osteosynthesis with wires, plaster immobilization.
- If there are radiological signs of synostosis, and the synostosis does not exceed 40-50% of the area of the growth plate, there is no significant shortening, the child is under 6-7 years old, the child is not large - curettage (resection of synostosis), corrective osteotomy, osteosynthesis with knitting needles, plaster immobilization.
- If there is significant synostosis, shortening of the lower leg, a child over 6-7 years old, we perform epiphysiodesis (closure of the functioning growth zone by drilling), osteotomy (intersection) of the lower leg bones, lengthening and correction of the deformity using transosseous osteosynthesis. A number of orthopedists prefer not to perform epiphysiodesis, but use the so-called. overcorrection (i.e. they create a valgus deformity from a varus one). We are categorically opposed to this method, because In our experience, maintaining a functioning part of the growth zone in the presence of synostosis (closure) on the other leads to a recurrence of the deformity as it grows, and a relapse occurs in the shortest possible time (6-12 months). In our practice, we strive for ideal correction and, if possible, perform “re-lengthening” of the lower leg, counting on the continued growth of the child.
Meniere's disease code according to ICD-10
ICD-10 is an international classification of diseases, that is, it is a kind of rubricator of diseases and pathologies. Every diagnosis or condition known in the world is assigned a specific code. Each code has an alphanumeric designation. In this encrypted form, it is much easier to store and analyze data on morbidity and mortality obtained from different parts of the world.
Make an appointment right now!
Call us by phone or use the feedback form
Sign up
Once every decade, this classification is revised under the guidance of the World Health Organization (WHO). The number 10 in the abbreviation ICD-10 indicates that the current classification has already been revised ten times.
According to this classification, Meniere's disease is coded H81.0.
Treatment methods
In childhood and adolescence, with timely consultation with an orthopedist, the disease can be cured without consequences for the body. The general treatment regimen depends on the degree of development of the pathology and the age of the patient. At a younger age, bones are more amenable to correction, so the disease goes away faster.
Conservative therapy
To successfully treat a disease, it is necessary to correctly determine its degree. If there is a potential type of change, the doctor recommends:
- physical therapy,
- massage course,
- orthopedic shoes,
- physiotherapy with mud applications and paraffin,
- oxygen mixture therapy,
- stimulation of muscle tone with medications.
For moderate and progressive types of the disease, as well as in young children, plaster casts are often used. Treatment is complemented by exercise therapy and physiotherapy using ultraviolet light.
Surgical intervention
The operation is indicated in cases where the curvature persists until the age of 6 years. The surgeon excises abnormal areas of the tibia and femur. After surgery, the Ilizarov apparatus is applied to the limbs. It fixes the required position of the leg. If the knee joint remains unstable, doctors perform plastic surgery of its ligaments.
Causes
The exact causes of the disease have not yet been determined. However, the risk of its development increases due to damage to the tibia in the area of the epiphyseal cartilage. Doctors believe that this deviation is associated with the following anomalies:
- chondrodysplasia;
- osteochondropathy.
The pathology may be supplemented by other congenital diseases. There is also a hypothesis regarding a hereditary predisposition to the development of the disease. In addition, the provoking factors of Blount's disease include the following:
- excess weight;
- premature onset of walking – due to the absence of the crawling stage;
- traumatic injuries of the legs in infancy;
- complex infectious diseases;
- pathologies of endocrine organs.
The provoking factor in the development of the disease is the increased load on the unprepared musculoskeletal system in combination with the anatomical features of the legs.
Another cause of the disease is considered to be a lack of vitamin D. A lack of the element in food or a violation of its absorption can affect the appearance of the mutation. As a result, this becomes the cause of the disease.
Stages of deformation
What is borreliosis (Lyme disease)
Lyme disease (tick-borne systemic borreliosis, Lyme borreliosis) is a transmissible, natural focal disease characterized by damage to the skin, joints, nervous system, heart, often taking a chronic, relapsing course. Among infectious diseases transmitted by ticks, Lyme disease (LD) is the most common. The name of the disease comes from the name of the small town of Old Lyme in Connecticut (USA), where in the mid-1970s a number of cases of arthritis after tick bites were described. In Europe, Borrelia infection had already been known for a long time under various names (erythema migrans, Bannwart syndrome), but the pathogen was isolated only in 1982.
Symptoms
Until 2-3 years of age, there are no manifestations of pathology. This is due to the fact that the child does not yet know how to walk well. The main symptom of the disease is deformation of the legs. If treatment is not started in time, the curvature will progress.
External manifestations of the disease include the following:
- Shortening of limbs. This causes the arms to appear too long. There are cases when the fingers reach the knees.
- Severe fatigue.
- Duck walk.
- Decreased muscle tone in the legs.
- Development of flat feet.
- Atrophic damage to the leg muscles.
- The appearance of a coracoid protrusion on the affected bone.
- Short stature.
- Clumsy gait and lameness.
Pathogenesis
Varus alignment of the tibia causes overload of the internal or external condyle of the tibia, as a result of which the epiphyseal zone expands, bevels, and moves inward and downward. Due to the uneven distribution of the load, not only bones, but also soft tissues are exposed to increased pressure, which leads to the occurrence of neurodystrophic disorders. As a result, the function of the limb is further impaired, and pathological changes in the pineal gland are aggravated. The ossification process is disrupted, cartilage cells either turn into bone tissue more slowly than normal, or transform into inferior bone, unable to withstand normal loads. The condyle grows at an angle, a beak-like protrusion appears in the area of the metaphysis, and a curvature is formed below. In the lower parts, the lower leg remains almost straight, the foot rotates medially.